
Abstract
Two women, aged 19 and 20 years, underwent surgery for hydatid cyst at the right side of the heart. In one patient, the cyst was located on the interventricular septum. It was removed and the defect was closed without capitonnage to avoid blockage. The cavity healed spontaneously. In the other patient, the cyst was at the right atrioventricular groove. It was removed without cardiopulmonary bypass. Both patients recovered well.
Introduction
Cardiac hydatid cyst is an uncommon disease seen in 0.4% to 2% of patients with echinococcosis. 1 It is rarely established at the interventricular septum on the right side of the heart. 2
Case Reports
Case 1
A 19-year-old woman was admitted with dyspnea and chest pain. On physical examination, there was a 2/6 systolic murmur at the pulmonary area. The pulmonary artery was seen on telecardiography to be enlarged. A single cyst was observed on thoracic and abdominal computed tomography. Echocardiography demonstrated a very large hydatid cyst measuring 3 × 4 cm, in the right ventricular outflow tract (Figure 1A). There was an infundibular gradient of 38 mm Hg.
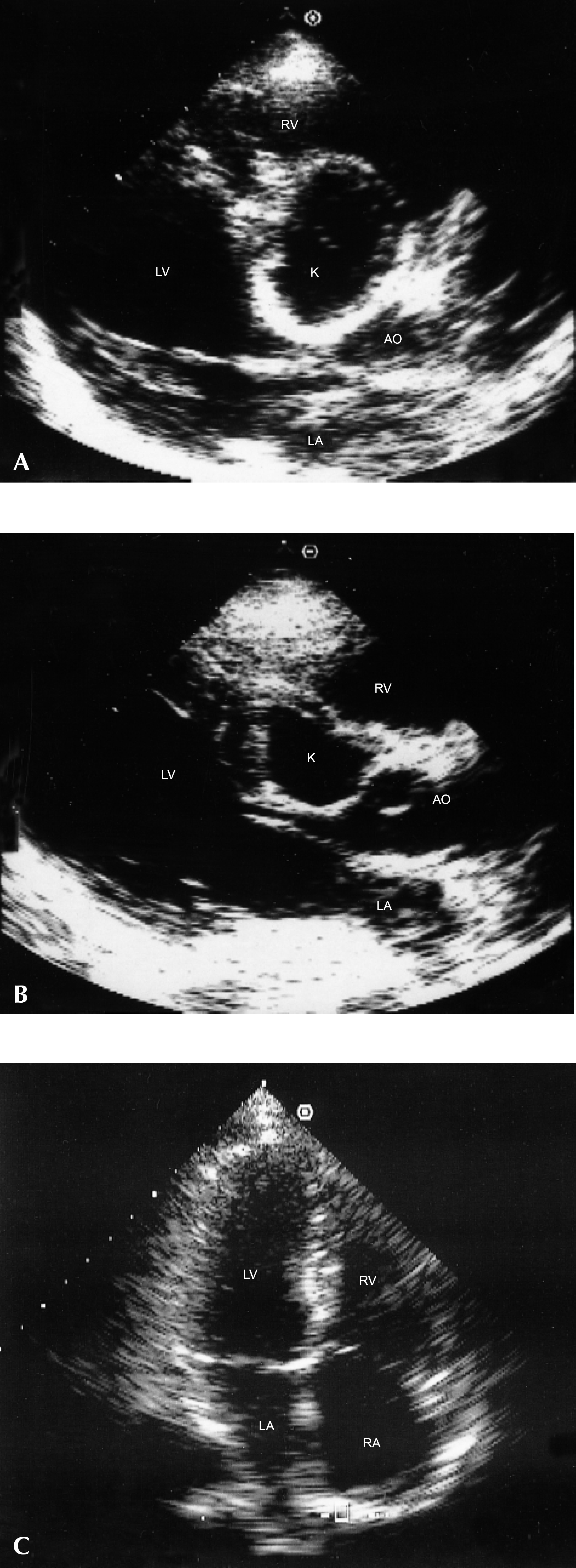
Echocardiography in case 1. (A) The cyst can be seen to the right of the interventricular septum. (B) The residual defect in the septum 5 days postoperatively. (C) The interventricular septum showed no sign of a defect at 18 months postoperatively. AO = aorta, K = cyst, LA = left atrium, LV = left ventricle, RA = right atrium, RV = right ventricle.
Case 2
A 20-year-old woman was investigated for dyspnea, palpitation, and chest pain. No abnormality was found on physical examination. Chest radiography revealed an enlarged heart with a bulge on the right border. Thora-coabdominal computed tomography confirmed the presence of a hydatid cyst on the epicardium, measuring 6 × 8 cm. Echocardiography showed that the cyst was located at the right atrioventricular groove.
Electrocardiograms demonstrated diffuse nonspecific ST-T changes in both patients. Invasive diagnostic techniques were not used. The patients underwent surgery via sternotomy. In the first case, the heart was arrested with cold blood potassium cardioplegia under cardio-pulmonary bypass with mild systemic hypothermia. Needle aspiration of the cystic contents was performed after sterilization with hypertonic saline solution. The right ventricular outflow tract was opened. The cyst which was established in the right ventricle on the interventricular septum was carefully removed from the subendocardial region. The defect was closed with superficial sutures, without capitonnage. The right ventricular outflow tract incision was sutured with 4/0 polypropylene. In the second patient, the cyst was located at the right atrioventricular groove. It was removed very carefully after sterilization and aspiration, without cardiopulmonary bypass. The right coronary artery was intact. The right atrium and right ventricle were not perforated during this procedure. The postoperative course was satisfactory in both patients and they were discharged on the 8th postoperative day without any complications. Echocardiography was performed in the first patient 5 days and 18 months later (Figure 1B); no gradient was observed. The space in the interventricular septum that was not repaired by capitonnage, to avoid the risk of blockage, was seen on the last echocardiogram to have healed spontaneously (Figure 1C). The second patient had echocardiography one year postoperatively. No new lesions were detected in either patient and they are currently in New York Heart Association functional class I.
Discussion
In hydatid disease, the severity and nature of the signs and symptoms are extremely variable and rarely pathog-nomonic, and different clinical syndromes may be present. The helminth usually reaches the heart via the coronary circulation. It grows slowly in myocardial tissue and within 1 to 5 years, it forms the actual cyst. Left ventricular myocardium is the most common site for cardiac echinococcosis because of its relatively greater blood supply. The cyst is less frequently seen in the right ventricle where it is most likely to be found at the interventricular septum; it is seldom located on the right atrial wall. 2 The cyst comprises an outermost protective membrane called the pericystic layer, a laminated membrane, and a germinal layer containing hydatid fluid. Pericystic growth of a viable hydatid cyst may determine outcome such as rupture into the heart chambers or pericardial cavity, compression of the coronary vessels with resultant myocardial ischemia, disturbances of the conduction mechanism of the heart, obstruction of the ventricular outflow tracts, or pulmonary emboli. 1 For these reasons, it must be operated upon as soon as it is diagnosed.
Miralles and colleagues 3 stated that coronary angiography and ventriculography should be performed in all patients. However, we considered that two-dimensional echo-cardiography was adequate in these cases of a single cardiac cyst. Moreover, there is a risk of puncturing the subendocardial cyst when such invasive techniques are employed. 4 For superficial cysts, excision can be performed on a beating heart after emptying the heart by cardiopulmonary bypass. We did not use cardiopulmonary bypass in the second patient because there was good exposure and the cyst had not penetrated the cardiac chambers. Compression of the coronary arteries by a cyst can cause myocardial infarction. 4 However, there was no compression of the right coronary artery in case 2.
Some authors have suggested using albendazole as an adjunct to surgery to decrease the risk of recurrence. 1 However, albendazole was not used postoperatively in these patients and no new cysts were detected on follow-up echocardiography.