
Abstract
Patients with giant left atrium were divided into 2 groups retrospectively. Group 1 comprised 10 patients with compression symptoms who received left atrial plication after mitral valve replacement. Group 2 comprised 31 patients without symptoms of compression who did not mreceive plication. Age, sex, ejection fraction, and left ventricular end-diastolic pressure were similar in the 2 groups preoperatively. Left atrial diameter reduction was not significantly different between the 2 groups. Mean left atrial diameter was 80.41 ± 15.08 mm preoperatively and 66.64 ± 13 mm postoperatively in group 1. In group 2, the mean values were 80 ± 8.95 and 66.1 ± 8.14 mm, respectively. Postoperatively, no differences were observed in ejection fraction or left ventricular end-diastolic pressure between the 2 groups. Left atrial diameter was over 80 mm in 12 patients in group 2 and it did not reduce postoperatively to below 65 mm in 11 of these patients. On the other hand, only 7 of 19 patients with a left atrial diameter below 80 mm preoperatively did not reduce to values below 65 mm (p = 0.04). Therefore, in cases of giant left atrium with a left atrial diameter below 80 mm, plication might not be necessary.
Introduction
Rheumatic mitral valve disease presents as mitral stenosis, mitral regurgitation, or a combination of both. Enlargement of the left atrium (LA) is associated with these entities and when the anteroposterior length is over 65 mm on echocardiography, it is defined as giant left atrium. 1 Enlargement of the LA may create compression of surrounding structures such as the esophagus, pulmonary veins, trachea, left main bronchus, middle and lower lobes of the right lung, inferior vena cava, recurrent laryngeal nerve, and thoracic vertebrae, leading to dysphagia, respiratory dysfunction, peripheral edema, hoarse voice, or back pain. 1 According to some authors, paradoxical movement of the left ventricular posterobasal wall occurs in giant LA and may affect hemodynamics in a negative manner. 2 Left atrial dilatation may also cause atrial fibrillation and thromboembolism. 3,4
Several techniques of left atrial size reduction during mitral valve replacement have been developed to eliminate symptoms of left atrial compression, enlargement, and potential postoperative complications. 3 –5 Left atrial plication may prolong operation time and incur complications such as circumflex coronary artery injury, pulmonary vein obstruction, or esophageal stricture. The rise in pressure due to mitral valve dysfunction may decrease after mitral valve replacement. Decreasing pressure in the LA may eliminate compression of the left ventricular posterobasal wall without plication, but this has not been clarified. This study compared patients with giant LA who underwent mitral valve replacement with plication and those without compression symptoms who underwent mitral valve replacement without plication.
Patients and Methods
Forty-one patients who were operated upon for mitral valve disease between January 1996 and April 1997 and who met the Piccoli criteria for giant LA (anteroposterior left atrial diameter over 65 mm by echocardiographic assessment) were studied retrospectively. 1 The patients were separated into 2 groups: 10 patients with compression symptoms who underwent plication (group 1); and 31 non-plicated patients without compression symptoms (group 2). Patients with aortic valve disease or coronary artery disease were not included in the study. In group 1, 2 patients had pure mitral valve stenosis, 3 had pure mitral insufficiency, and 5 had mitral stenosis and insufficiency. In group 2, 6 patients had mitral stenosis, 2 had mitral insufficiency, and 23 had mitral stenosis and insufficiency. All patients had a history of rheumatic fever. Five patients in group 1, and 6 in group 2 had third-degree tricuspid insufficiency; these cases were treated by Kay annuloplasty. In group 1, 8 patients were in New York Heart Association (NYHA) functional class III, and 2 were in NYHA class IV. In group 2, 16 patients were in NYHA class II, 12 were in class III, and 3 were in class IV. All patients had atrial fibrillation but none had experienced a thromboembolic event. Mean age in group 1 was 39 ± 12 years; there were 6 women and 4 men. Mean age in group 2 was 42 ± 11 years; there were 19 women and 12 men. In group 1, 8 patients received a no. 29 St. Jude Medical mechanical valve (St. Jude Medical, Inc., St. Paul, MN, USA) and 2 had a no. 31 St. Jude Medical valve. In group 2, 24 patients received a no. 29 St. Jude Medical valve and 7 had a no. 31 St. Jude Medical valve. Echocardiographic evaluations were made by an experienced cardiologist using an Ultramark 6 color Doppler echocardiograph (Omega Imaging, Cordova, TN, USA) with a 3.5-MHz electronic probe, in basal conditions at rest.
Cardiopulmonary bypass was established by aortic and bicaval cannulation after induction of general anesthesia. Diastolic arrest was achieved with antegrade potassium cold blood cardioplegia after crossclamping. In group 1, Kawazoe's plication technique was used in addition to mitral valve replacement. 3 Plication was made with 3/0 polypropylene on the left atrial posteroinferior wall (area between the mitral valve ring and the right and left pulmonary vein orifices) in a semilunar shape between the upper edge of the left atrial appendage and the posteromedial area of the mitral valve. At first, several sutures 1 cm away from the mitral valve annulus and 1.5 to 2 cm away from the pulmonary vein orifice were plicated, then the spaces between the area stated above were closed by the continuous suture technique. The plication was completed from the caudal edge of the left atrial appendage lengthways along the atrial cranial side to the right and left pulmonary vein orifices, in a horseshoe shape. The width of the plication was between 35 and 50 mm, as in Kawazoe's technique. 3
SPSS version 9.01 software (SPSS, Chicago, IL, USA) was used in data analysis, and p < 0.05 was considered statistically significant. Preoperative and postoperative values were analyzed with the two-independent-sample t test and chi-squared test.
Results
No mortality was encountered in either of the groups. Pulmonary artery pressure dropped significantly in both groups postoperatively (Table 1). Left atrial diameters showed significant reduction after surgery in both groups (Table 1). When the 2 groups were compared, the postoperative decreases in pulmonary arterial pressure and the left atrial reduction were not significantly different. Extubation times were also similar (10.6 ± 1.89 hours for group 1, and 10.6 ± 1.83 hours for group 2). Reintubation was not required in any of the cases. One patient in group 1 suffered low cardiac output but recovered with inotropic treatment. The aortic crossclamp time was 62.3 ± 9.1 minutes in group 1, and 44.4 ± 11.2 minutes in group 2 (p < 0.05). All patients remained in atrial fibrillation postoperatively.
Echocardiographic Data
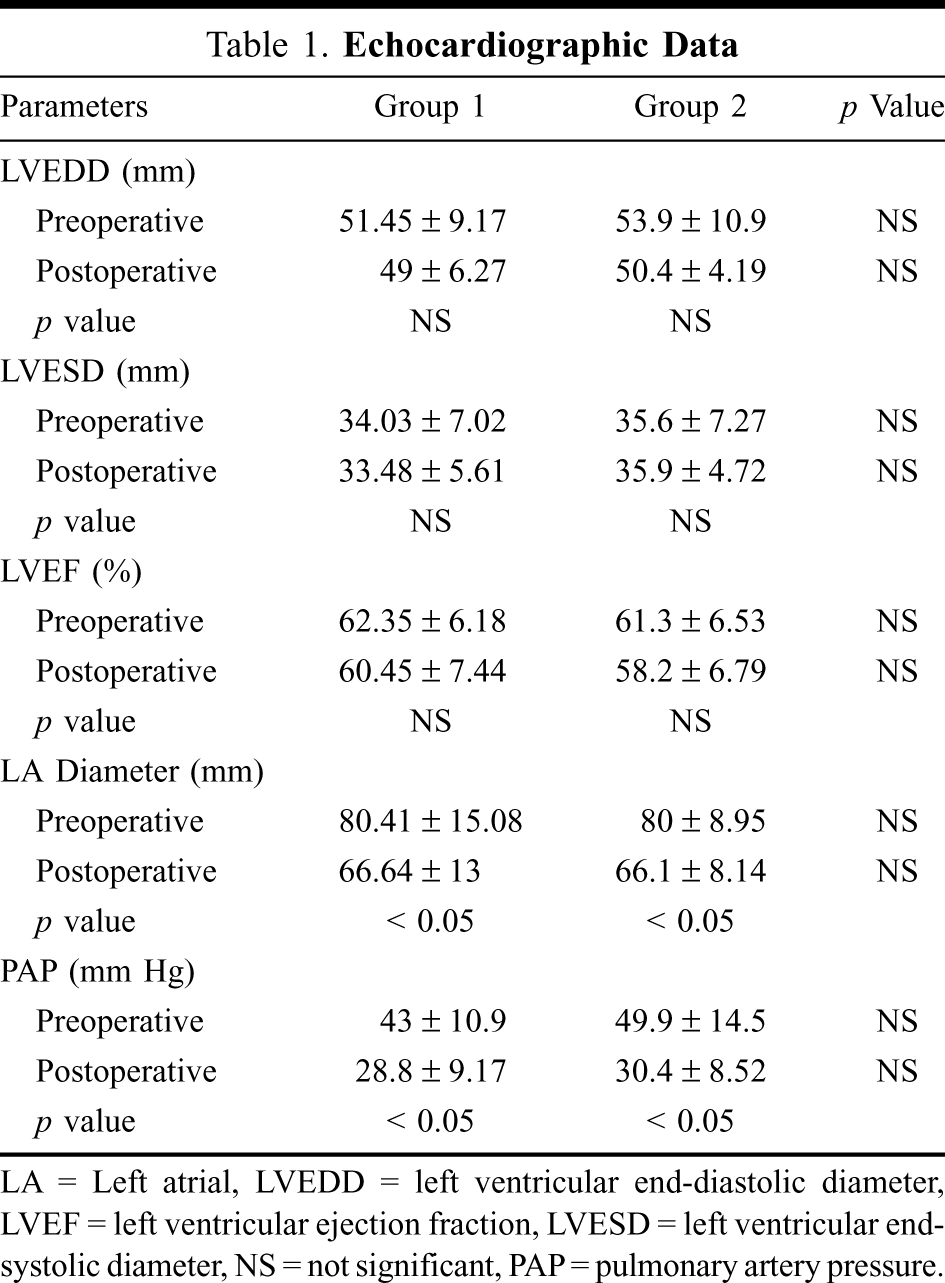
LA = Left atrial, LVEDD = left ventricular end-diastolic diameter, LVEF = left ventricular ejection fraction, LVESD = left ventricular end-systolic diameter, NS = not significant, PAP = pulmonary artery pressure.
In group 2, preoperative left atrial diameters were above 80 mm in 12 patients and they did not reduce below 65 mm in 11 of these (91.7%) postoperatively. Mean left atrial diameter in the preoperative period was 88.47 ± 15.2 mm for these 12 patients. On the other hand, preoperative left atrial dimensions were below 80 mm in the other 19 patients in group 2; mean preoperative left atrial diameter was 70.6 ± 6.39 mm for these patients, postoperative left atrial dimensions were still over 65 mm in 7 (36.8%) of these patients (p < 0.05). In the postoperative period, all patients were in NYHA functional class I. The mean duration of follow-up was 9 ± 2.8 months.
Discussion
An important factor in reduction of left atrial diameter is the effect of the rheumatic process on the elastic fibers of the tissue. This process causes strain and loss of tone, thus the LA does not become smaller. 6 Nevertheless, similar left atrial reduction was seen in both groups in this study. In the study by Johnson and colleagues, 4 left atrial plication with a right thoracotomy had higher incidences of mortality and low cardiac output, and it was stated that this procedure would be effective only to increase lung ventilation. However, Beppu and colleagues 2,3 noted paradoxical movement of the left ventricular posterobasal wall due to atrial compression in their echocardiographic studies on giant LA, and concluded that this would negatively affect hemodynamics. There are two important pathophysiological processes in patients with giant LA: the first is respiratory dysfunction due to compression of the left main bronchus and/or right middle or lower lobes of the lung; the second is excessive enlargement of the LA and compression of the left ventricular posterobasal wall as a result of hemodynamic dysfunction. 3 However, others have found no correlation between left atrial diameter and surgical results. 7 –9 In our study, there was no difference in mortality in patients with or without plication. There were also no significant differences between the two groups in respect of the need for positive inotropic support, postoperative ejection fraction, and long-term functional capacity. These results agree with the findings of Plaschkes and colleagues. 6 All patients were in atrial fibrillation preoperatively and postoperatively, thus reduction of left atrial diameter did not change this arrhythmia, as noted previously. 4 Barnhost and colleagues 10 concluded that atrial fibrillation was not due to increased pressure in the LA but to the injury caused by acute rheumatic fever.
Plication did not cause any complications, but it prolonged the crossclamp time. With regard to hemodynamic changes and reduction of left atrial diameter, there were no differences between plicated and non-plicated patients. Thus, mitral valve replacement without plication reduced left atrial diameter as much as mitral valve replacement with plication. Although thromboembolism was not seen in our patients, anticoagulation was considered to be more important than plication. In some patients with left atrial diameters above 80 mm preoperatively who did not receive plication, postoperative left atrial diameter was below 65 mm. Therefore, plication during mitral valve replacement might not be needed in patients whose left atrial diameter is below 80 mm, even if they have compression symptoms. Most patients with a preoperative left atrial diameter above 80 mm did not achieve a left atrial diameter below 65 mm after mitral valve replacement without plication. More studies are needed to determine whether mitral valve replacement without plication may correct the symptoms in patients with a left atrial diameter above or below 80 mm and with or without compression symptoms.