
Abstract
In a prospective randomized study, aprotinin was assessed in cyanotic children with tetralogy of Fallot undergoing total correction utilizing cardiopulmonary bypass. In group A (n = 25), 20,000 kallikrein inhibiting units of aprotinin per kilogram of body weight was administered before cardiopulmonary bypass and the same amount was added to the pump prime. In group B (n = 25), only a single dose of aprotinin was given before cardiopulmonary bypass. Blood loss and blood product requirements were compared with those in a control group of 25 patients who did not receive aprotinin. Blood loss and blood products used in groups A and B did not differ but the control group had significantly more bleeding and transfusion requirements. A single dose of aprotinin before cardiopulmonary bypass is recommended in cyanotic patients undergoing intracardiac repair.
Introduction
Children with cyanotic congenital heart disease requiring surgery under cardiopulmonary bypass (CPB) are at increased risk of bleeding complications. This is mainly due to acquired coagulopathy (secondary to cyanosis and polycythemia) associated with impaired platelet function, and hemostatic derangements due to CPB. 1,2 Peripheral sludging of blood in polycythemic cyanotic children induces hyperfibrinolysis secondary to intravascular stasis and thrombosis. They have decreased clotting factors, increased fibrinolysis, and a reduced number of functional platelets, as well as decreased plasma volume leading to proportionately reduced levels of clotting factors. 3 Volume replacement with homologous blood products carries the risks of infection and immunological reactions. Aprotinin has been used to maintain physiological balance in the hemostatic system for reoperation or complex surgical repair in pediatric patients. It has been postulated to improve hemostasis by preserving platelet function, and by its antifibrinolytic action. Aprotinin inhibits serine proteases such as trypsin, plasmin, and kallikrein. 4 It has also been used to protect platelet function and integrity in stored blood. 5 Plasmin inhibition by aprotinin occurs at lower plasma levels than those required to inhibit kallikrein or fibrinolysis. The efficacy of aprotinin in reducing blood loss in pediatric cardiac surgery has been assessed, but the most cost-effective dose was not clearly identified. The aim of this study was to confirm the role of aprotinin and compare the efficacy of 2 low-dose regimens in reducing blood loss and blood product transfusions in cyanotic pediatric patients undergoing intracardiac repair under CPB.
Patients and Methods
After institutional review board approval and parental consent, a prospective study was conducted on patients with tetralogy of Fallot undergoing total correction under CPB. Fifty cyanosed patients (systemic arterial oxygen saturation 80% or less) with polycythemia (hematocrit 50% or more) were randomly allocated to group A or B using computer-generated random numbers. Standard anesthetic and surgical techniques were followed in all patients. Premedication consisted of oral midazolam and atropine one hour prior to anesthesia. Anesthesia was induced with sevoflurane (8%) in oxygen, and maintained with oxygen, isoflurane, and morphine, with intermittent positive-pressure ventilation after endotracheal intubation. Anticoagulation was established with an initial bolus of porcine heparin (Biological Evans Ltd, Hyderabad, India) 400 units·kg−1 administered into a functioning central venous access. Additional doses of 100 units·kg−1 of heparin were administered during CPB to maintain an activated clotting time (ACT) greater than 480 seconds. Actalyke (Array Medical, Ashford, Kent, UK) was used to assess ACT with kaolin as the accelerator. ACT was measured before and after heparin administration, every 30 minutes during CPB, and after heparin reversal with protamine. The CPB system included a Sarns pump with a membrane oxygenator (3M Healthcare, Ann Arbor, MI, USA). The arterial catheter had a 40-micron heparin-coated polyester filter covered by a polycarbonate container. The pH, PO2, and PCO2 were assessed every 30 minutes and managed using alpha-stat strategy. Cold crystalloid St. Thomas' Hospital cardioplegia solution was used for myocardial preservation. The CPB circuit was primed with Ringer's lactate solution, 8.5% sodium bicarbonate, and heparin (5 units·mL−1). During CPB, the following conditions were maintained: hematocrit, 20% to 25%; pump flow, 2 to 2.6 L·min−1·m−2; rectal temperature, 24°C to 28°C; and mean arterial pressure, 40 to 70 mm Hg. To antagonize anticoagulation due to heparin, protamine sulfate was administered in an initial dose of 4.5 mg·kg−1 after separation from CPB.
Patients in group A received aprotinin (Bayer AG, Leverkusen, Germany) in the pre-CPB period in a dose of 20,000 kallikrein inhibiting units (kiu) per kilogram of body weight and a similar dose was added to the pump prime. Patients in group B received only a single dose of aprotinin (20,000 kiu·kg−1) before CPB. Pre-CPB aprotinin was administered as a continuous infusion through a central venous catheter over a period of 30 minutes between the end of anesthetic induction and before heparin administration. Patients in groups A and B received aprotinin in a blinded fashion, i.e., the principal investigator (RS) did not know the dose of aprotinin received by a given patient. No attempt was made to prevent or reduce inflammatory reactions during CPB; leukocyte filters and antiinflammatory pharmacological agents were not used. Perioperative laboratory tests included hematocrit, prothrombin time, activated partial thromboplastin time, platelet count, and fibrinogen concentration. Total blood loss comprised intraoperative and postoperative blood loss. Intraoperative blood loss was calculated from swab weights, discarded suction volumes, chest tube output, and volume of salvaged washed red cells. Postoperative blood loss was calculated from the chest tube output at 2, 6, 12, and 24 hours after arrival in the intensive care unit. Blood and blood components were administered to treat postoperative bleeding. After consideration of the rate and volume of blood loss, transfusion therapy was initiated if judged to be clinically indicated, and it was guided by hematocrit and coagulation test results. Postoperative transfusion criteria included a hematocrit of less than 28% or a hemoglobin level less than 90 g·L−1. Patients were monitored for anaphylactic reactions due to aprotinin, and postoperative renal function was assessed by serial estimations of serum creatinine. The following parameters were compared in a matched group of 25 control patients (group C) who did not receive aprotinin: total blood loss, total chest tube drainage, blood, and blood products transfused. Numerical data were expressed as mean ± standard deviation, and statistically analyzed using Student's t test.
Results
There were 25 patients in each group, and the groups were comparable in respect of age, sex, and weight. The demographic and surgical characteristics of the 2 study groups are shown in Table 1. There were no statistical differences between these 2 groups in terms of duration of CPB, aortic crossclamp time, and total heparin dosage. Differences in blood loss and blood product requirements in groups A and B were similar. However, blood loss, chest tube drainage, blood, and blood product use in group C were significantly higher than in groups A and B (Table 2). Perioperative changes in hematocrit in groups A and B showed no significant differences (Table 3). The duration of ventilation was 17.08 ± 4.8 hours in group A and 16.77 ± 5.2 hours in group B. No adverse reactions due to aprotinin were noted.
Demographic and Surgical Data
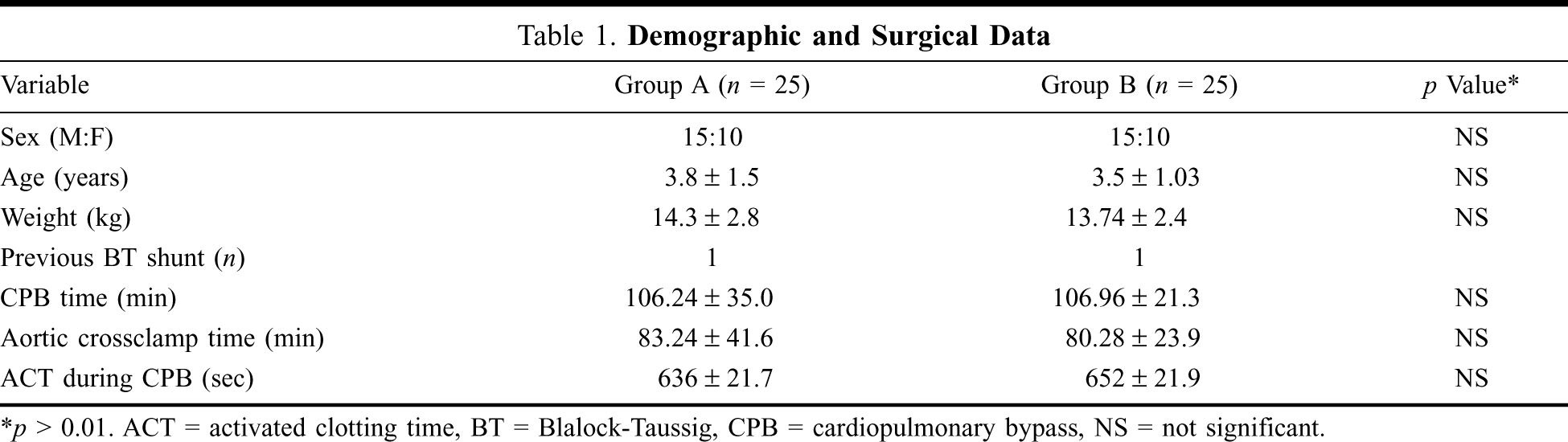
p > 0.01. ACT = activated clotting time, BT = Blalock-Taussig, CPB = cardiopulmonary bypass, NS = not significant.
Comparison of Blood Loss and Blood Product Requirements
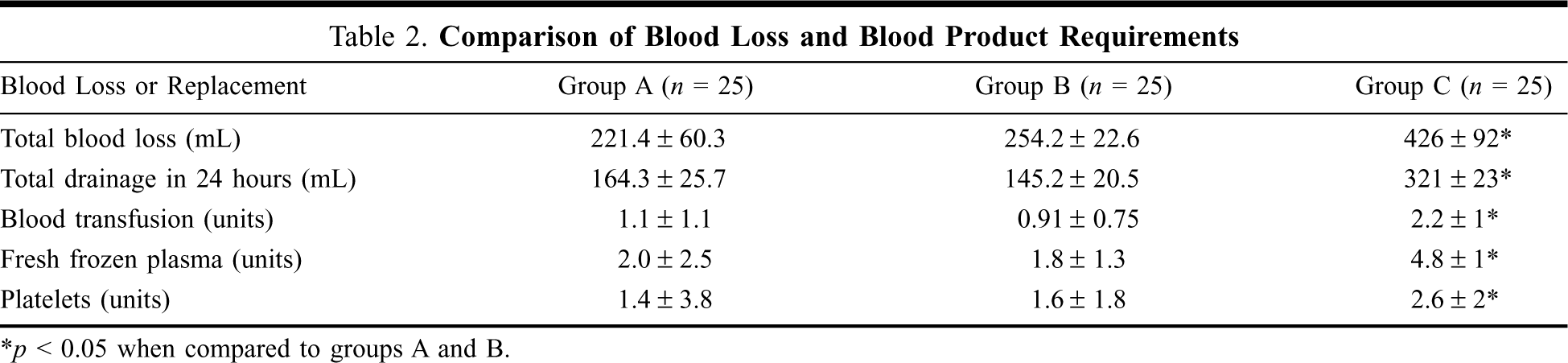
p < 0.05 when compared to groups A and B.
Comparison of Hematocrit

p > 0.05. CPB = cardiopulmonary bypass, NS = not significant.
After surgery, all patients awoke promptly and were extubated after overnight ventilatory support. No patient was reexplored for bleeding or tamponade. There was no incidence of renal failure; postoperative creatinine levels increased by 5 ± 1 mg·L−1 in 24 hours and reverted back to basal levels after 72 hours. There was no mortality in the series.
Discussion
The diversity of causes of platelet dysfunction due to CPB (hypothermia, drugs, fibrinolysis, receptor defect, and contact activation) partly explains the difficulty in reproducibly measuring and mitigating it. Hypothermia to 22°C reversibly inhibits platelet aggregation and slows the thrombin-induced platelet activation that occurs at normothermia. Heparin induces platelet dysfunction through a variety of mechanisms including inactivation of circulating thrombin by active enhancement of anti-thrombin III. The doses of heparin used for anticoagulation during CPB induce a fibrinolytic state that further renders platelets dysfunctional. Fibrinolysis has adverse effects on platelet function and is prevalent during CPB, although its contribution to postoperative blood loss may be di-minished by the widespread use of antifibrinolytic agents.
Aprotinin, a serine protease inhibitor, has been used in pediatric CPB to decrease postoperative blood loss and fibrinolysis. 6 Significant decreases in blood loss and blood transfused in surgical treatment of tetralogy of Fallot were noted. 7,8 This benefit is related to inhibition of plasmin-induced complement activation, thus decreasing fibrinolysis and significantly neutralizing the inflammatory reaction to CPB. Direct platelet membrane receptor protection by aprotinin has also been postulated. 9 A low plasma level of aprotinin (50 kiu·mL−1) inhibits plasmin, but 200 kiu·mL−1 is needed to ensure inhibition of kallikrein. 10 Plasmin influences platelet function and activates platelets. 11 In this study, aprotinin dosage was determined according to body weight, but plasma levels were not measured. The wide range of recommended aprotinin regimens for adult cardiac surgery do not consider body weight or surface area and are based on standard doses, except in 2 recent reports where dosage was based on body weight. 12,13 The benefits of low doses of aprotinin have been demonstrated. 12 –16 Similar benefits were found with 280 mg of aprotinin administered only in the CPB prime, and with high-dose regimens. 13 The clinical efficacy of low-dose aprotinin has stimulated research on its effects on platelet function. It is likely that aprotinin has a regulatory role in the coagulation-fibrinolysis balance or in the mechanism of fibrinolysis. However, the attractive idea of aprotinin as a platelet protector during CPB might be overly simplistic because of the complexity of the hemostatic system. In pediatric cardiac surgery, the optimal aprotinin dosage is still controversial. Our results are comparable to those of Boldt and colleagues 17 showing no significant difference in blood loss and blood product usage with various doses before and during CPB, whereas Penkoske and colleagues 18 found decreases in blood loss, volume of transfusion, and number of units transfused. In pediatric lung transplants, Jaquiss and colleagues 19 observed that high-risk patients receiving aprotinin bled less than or were similar to low-risk transplant patients who had not received aprotinin. Dietrich and colleagues 20 noted reduced early postoperative mediastinal drainage in patients weighing less than 10 kg.
The antiinflammatory properties of aprotinin may enhance postoperative hemodynamic stability and decrease postpump syndrome by attenuating the inflammatory response. Aprotinin modifies the release of systemic endotoxins and tumor necrosis factor, which are implicated in reperfusion injury. In fact, the ability of aprotinin to blunt inflammatory effects is as effective as corticosteroid treatment, but this effect was not evaluated in this study. As a heterologous protein, aprotinin has antigenic properties, but no allergic reactions were noted in our patients. The cost of processing one unit of homologous blood in the blood bank in our centre is the same as the cost of 500,000 kiu of aprotinin. Therefore, we consider that a single pre-CPB dose of aprotinin (20,000 kiu·kg−1) is highly cost-effective and justifiable. Further inves-tigation of aprotinin in the pediatric patient population is needed to optimize dosing regimens and to define its role in the inflammatory process and long-term clinical outcome in cyanotic infants.