
Abstract
A technique for simultaneous cardiac operation and pulmonary resection via a small upper midline sternotomy is described. It was employed in a 62-year-old man undergoing aortic valve replacement and right lower lobectomy for a carcinoid tumor.
Introduction
Minimally invasive cardiac surgery is becoming popular. As well as a small anterior thoracotomy, parasternal, upper transverse, and upper midline sternotomy incisions have been tried. The rationale is to reduce surgical trauma, wound complications, and hospital stay. 1 –3 Noncardiac thoracic surgery has evolved in a similar way and video-thoracoscopy has promoted less invasive surgical access, even for radical treatment of cancer. Cardiac and pul-monary diseases requiring surgical treatment can coexist, and a simultaneous or sequential approach may be decided. There are a few reports of simultaneous pulmonary resection and cardiac surgery. 4 –7 Combined cardiac and pulmonary operations are feasible and safe, and minimal access might be considered in certain patients. The following technique was devised to excise a right lower lobe lung mass in a patient who also required aortic valve replacement.
Technique
A double-lumen endotracheal tube is placed. Through an upper midline “J” sternotomy, the lung mass is visualized and a right lower lobectomy is performed using bronchial stapling. Mediastinal nodes are dissected. Cardio-pulmonary bypass is established with aortic cannulation and a Heartport cannula (Heartport, Inc., Redwood City, CA, USA) in the right common femoral vein. A left ventricular vent is inserted through the right superior pulmonary vein. Cold blood cardioplegia is directly infused into the coronary ostia. The aortic valve is resected and annular debriding is carried out. A 21-mm Carpentier-Edwards pericardial xenograft (Edwards Lifesciences Inc., Irvine, CA, USA) is implanted using 2/0 braided everting mattress sutures. Intracardiac air is carefully removed and the aortotomy is closed. The incision is closed, leaving 2 chest tubes in place.
Discussion
The technique was employed in a 62-year-old man with a history of smoking, hypertension, and duodenal ulcer, who presented with dyspnea and angina, and was found to be in New York Heart Association functional class II. Chest radiography showed a noncalcified right lower lobe mass of 4 cm in diameter. Two-dimensional trans-thoracic echocardiography confirmed calcified aortic stenosis with peak and mean gradients of 80/55 mm Hg, and normal coronary arteries. Computed tomography confirmed a solid noncalcified 42 × 35-mm right lower lobe mass (Figure 1). Biopsy disclosed a pulmonary carcinoid. Lung function was within normal limits. After pulmonary resection and replacement of his stenosed tricuspid aortic valve, the patient came off cardio-pulmonary bypass easily and was extubated after 18 hours. After 5 days, Doppler ultrasound confirmed thrombosis in the right common femoral vein. This was most likely related to the venous cannulation site that was chosen in preference to the right atrium to allow more space to perform the pulmonary resection and any additional maneuvers that might be needed during the operation. The patient was given intravenous heparin; he was discharged on the 11th postoperative day, and oral anticoagulation was prescribed for 6 months. One year postoperatively, he was doing well, in sinus rhythm, and leading a normal life. Transthoracic echocardiography showed a normal functioning pericardial xenograft, a mean aortic gradient of 15 mm Hg, and a valve area of 1.7 cm2. No additional medication was prescribed.
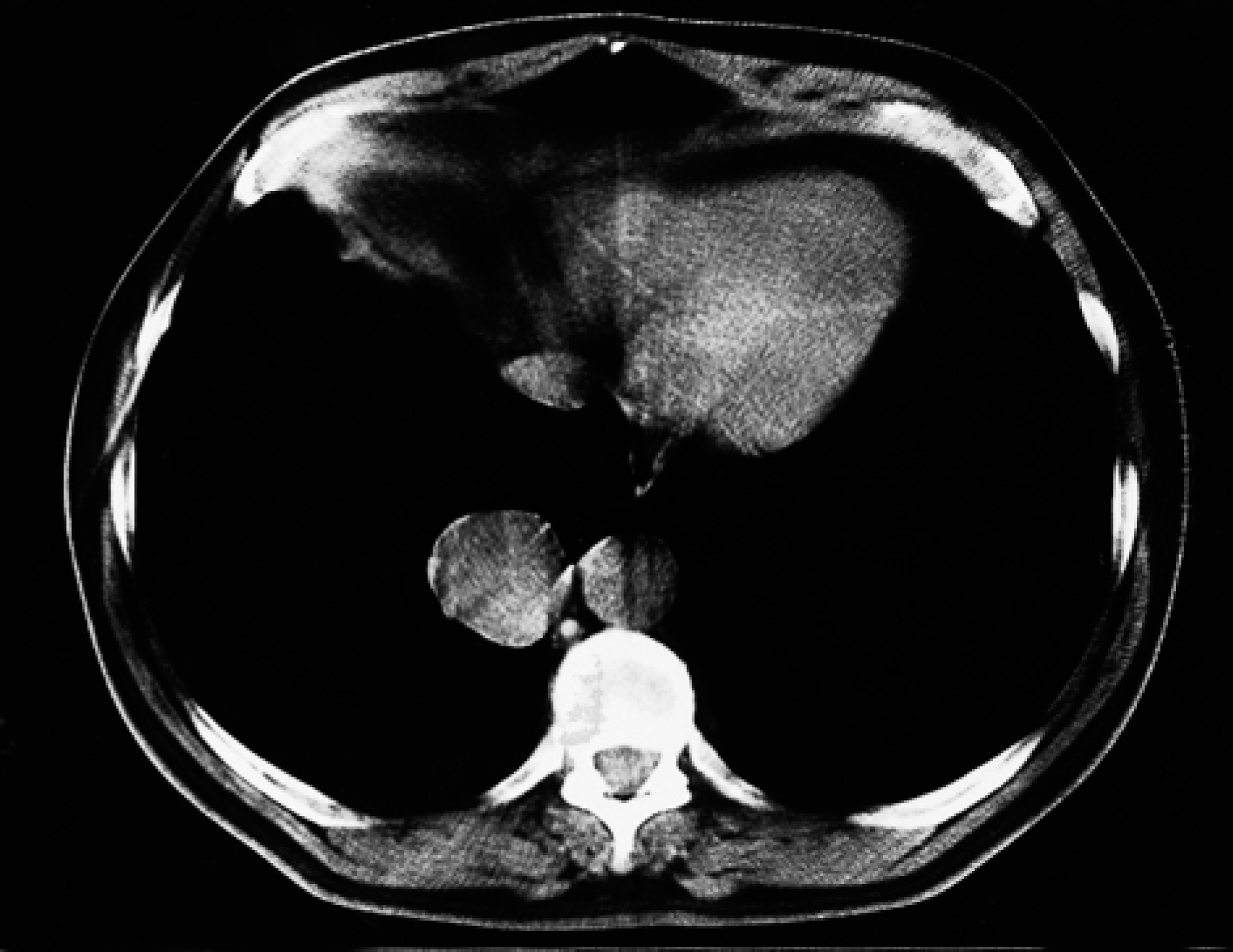
Computed tomographic scan showing a solid pulmonary mass located in the right lower lobe.
Pulmonary resection was performed before heparinization so that bleeding could be more easily controlled in the event of dense pleural adhesions or an extended hilar resection. Rao and colleagues 6 performed 5 pulmonary resections after valve replacement because of the possibility of valve contamination by respiratory pathogens when the airway is open. However, the lack of a large series precludes firm conclusions on the optimal order of the operations. 4 –7 Other aspects of this treatment are also debatable, such as the possibilities of incomplete media-stinal node dissection, technical difficulties, or metastatic spread enhanced by cardiopulmonary bypass. However, this case demonstrates that complete treatment of both cardiac and thoracic diseases was carried out according to the established criteria for neoplasms; mediastinal node dissection was performed, and pathological assessment confirmed a disease-free bronchial resection stump intraoperatively.
We believe that a combined simultaneous cardiac operation and pulmonary resection through minimal access is technically feasible in selected patients.