
Abstract
From April 1999 to July 2000, the Acorn cardiac support device was assessed in 22 patients with advanced heart failure, 10 of whom received mitral valve repair. There was 1 hospital death unrelated to the device, and 2 late deaths at 2 and 8 months postoperatively. The survivors had no device-related complications during a mean follow-up of 10.4 months. Mitral valve regurgitation improved in all patients and none had evidence of constrictive or restrictive physiology on repeat cardiac catheterization at 6 months. Preoperatively, 22% were in New York Heart Association functional class II, 71% in class III, and 7% in class IV. At 6 months postoperatively, 33% were in class I, 56% in class II, 11% in class III, and none in class IV. Ejection fraction increased from 19% ± 8% to 26% ± 10% at 3 months and 24% ± 11% at 6 months. Left ventricular end-diastolic diameter decreased from 74 ± 6.1 mm preoperatively to 68 ± 11 mm at 6 months. These findings indicate that the device is safe and effective in treating heart failure. Additional studies and longer follow-up are needed to confirm these results.
Introduction
Dilated cardiomyopathy of valvular, ischemic, or idiopathic origin is associated with increasing heart size. Clinical experience from dynamic cardiomyoplasty and experimental findings in a model of progressive heart failure showed that the downward course of heart failure could be halted by preventing further cardiac dilatation. 1 –3 As an initial clinical assessment, the feasibility and safety of a cardiac support device (Acorn Cardiac Support Device; Acorn Cardiovascular, Inc., St. Paul, MN, USA), a textile tissue of high elasticity designed to be wrapped around the heart, was evaluated in a nonrandomized study.
Patients and Methods
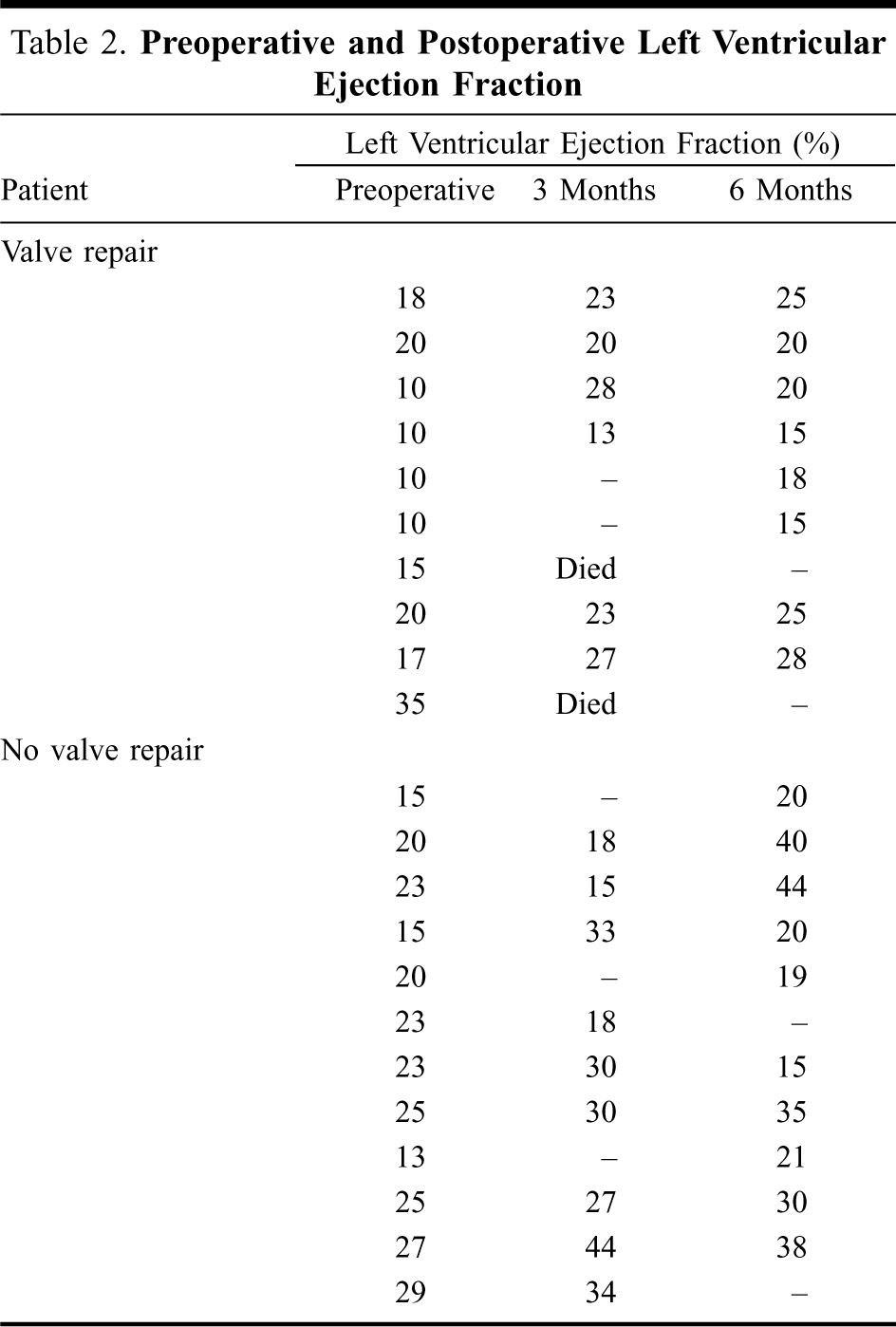
Inclusion criteria for the study were dilated cardio-myopathy of either ischemic or nonischemic origin, 18 years or older, left ventricular end-diastolic diameter > 60 mm or left ventricular end-systolic diameter > 50 mm, New York Heart Association (NYHA) functional class III or IV on at least one previous occasion, and acceptable renal and pulmonary function. Exclusion criteria were existing patent coronary artery bypass graft, significant risk as determined by the implanting surgeon, uncontrolled hypertension or malignant arrhythmias posing significant risk during the perioperative period, hypertrophic obstructive cardiomyopathy, pregnancy, and expected survival of less than one year. After obtaining informed consent and institutional review board approval, 29 consecutive myopathic patients underwent placement of the cardiac support device (CSD) from April 1999 to July 2000. CSD placement was the only measure in 12 patients, 10 underwent concomitant mitral valve repair; the remaining 7 patients required additional extensive cardiac procedures and were excluded from this study. Ages in the study group ranged from 34 to 71 years (median, 60.5 years) and 88% of the patients were male. The median duration of heart failure was 4 years (range, 1 to 13 years). Preoperatively, all patients received angiotensin-converting enzyme inhibitors and diuretics, 90% were on digoxin, and 70% on beta-blockers. There were no ischemic patients in the study. Preoperative cardiac findings are shown in Table 1. Primary endpoints to document the feasibility of the device were ease of implantation and constrictive effects on the heart. CSD implantation would be considered safe for further clinical evaluation if the following criteria were met: a low rate of serious adverse events; no clinically significant deterioration in diastolic function; and no significant impact on coronary blood flow. Extensive cardiac investigations including echocardiography, right and left heart catheterization with pressure volume loops, and coronary flow studies were performed postoperatively.
Preoperative Evaluation of 22 Patients Implanted With a Cardiac Support Device
After median sternotomy and opening of the pericardium, the diameter and length of the heart were determined with a special measuring tool and the appropriate CSD was selected. With the patient on full cardiopulmonary bypass, mitral valve repair with a Cosgrove annuloplasty ring (Baxter Healthcare, Deerfield, IL, USA) was performed first, when appropriate. One patient underwent repeat mitral valve repair. The CSD was then slipped over the heart and attached close to the atrioventricular groove. With the heart raised, 3 sutures of 4/0 polypropylene were used to attach the CSD to the most posterior areas. It was secured to the left and right lateral aspects of the heart under partial loading. With the heart fully loaded, the anterior part of the CSD was fitted, trimmed to size, and secured. Figure 1 shows the operative site after completion of the procedure. Postoperative treatment followed institutional protocols for heart failure patients after cardiac surgery. The preoperative heart failure treatment was resumed soon after surgery. Follow-up was carried out by hospital visits at 3, 6, and 12 months postoperatively. Follow-up was complete with a mean duration of 10.7 months and a total of 18.75 patient-years. Data were calculated as mean ± standard deviation.
Operative site after implantation of the Acorn cardiac support device.
Results
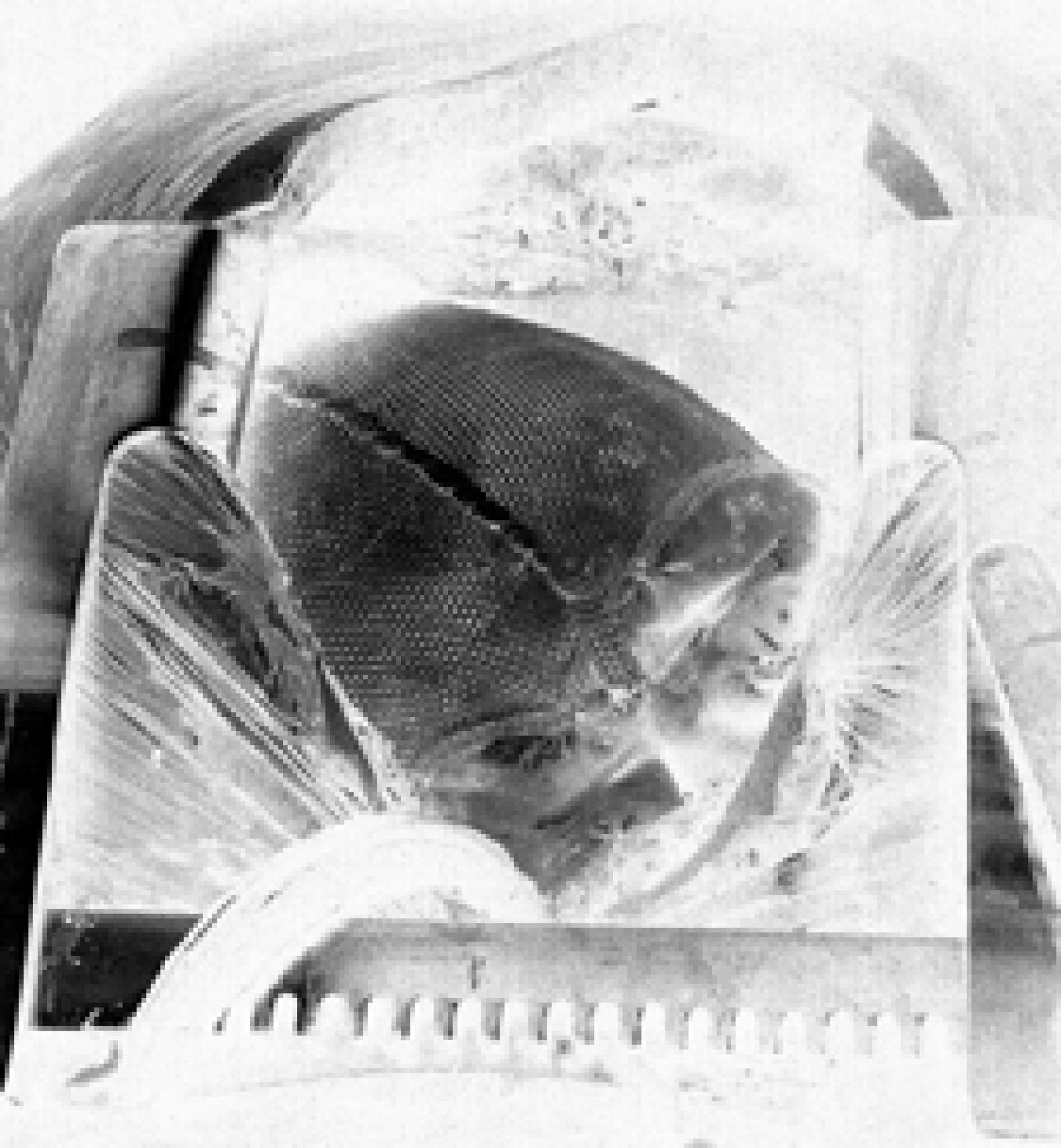
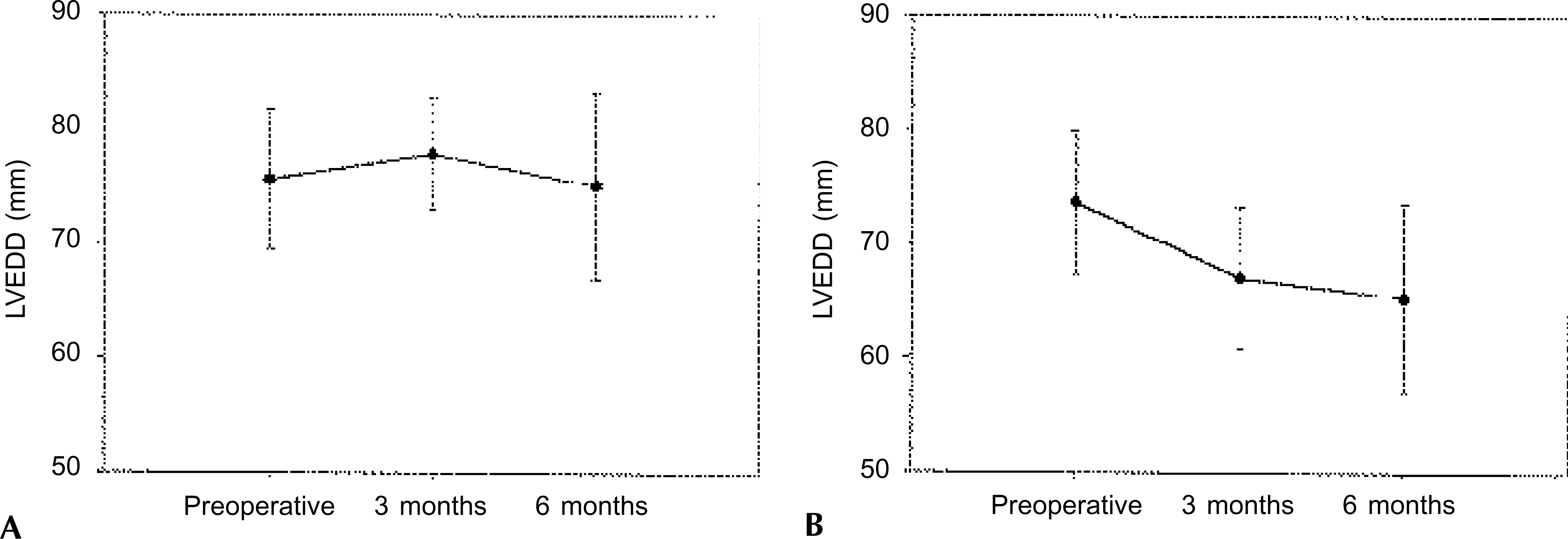
No patient died intraoperatively, 1 early death occurred on the 4th postoperative day due to sepsis. There were 2 late deaths: 1 due to fatal arrhythmias 44 days postoperatively, and 1 due to pneumonia 8 months after surgery. Adverse events were rare and comprised pleural effusions in 3 patients in the second week after the operation, and cerebrovascular accident with only partial recovery in 1 patient. No wound infection or pericardial effusion occurred. Size reduction over 6 months was noted in both groups; however, it was more pronounced in patients receiving CSD placement as the sole surgical measure (Figure 2). Overall, left ventricular end-diastolic diameter decreased from 74 ± 6.1 mm preoperatively to 68 ± 11 mm at 6 months. Left ventricular ejection fraction increased in most patients over time (Table 2). Mean preoperative ejection fraction was 19% ± 8%, increasing to 26% ± 10% at 3 months and 24% ± 11% at 6 months. After 6 months, mitral valve regurgitation had decreased from 2.5 ± 0.5 degrees to 0.7 ± 0.6 degrees in patients who had mitral valve repair, and from 1.1 ± 0.7 degrees to 0.6 ± 0.5 degrees in patients who had CSD placement only. Cardiac catheterization at 3 and 6 months confirmed the echo data indicating decreased heart size and improved cardiac function, and showed no constrictive pattern of left or right ventricular function, as well as demonstrating maintained coronary flow reserve. Detailed analysis of the catheter data have been communicated previously. 4 The NYHA functional class of all patients improved. Preoperatively, 22% were in NYHA class II, 71% in class III, and 7% in class IV. At 6 months postoperatively, 33% were in class I, 56% in class II, 11% in class III, and none in class IV. In those with concomitant mitral valve repair, mean NYHA class improved from 2.7 ± 0.7 to 1.8 ± 0.9 at 12 months postoperatively, and in patients who had CSD only, NYHA class decreased from 2.4 ± 1.7 to 1.7 ± 0.5.
Echocardiographic changes in heart size after implantation of the Acorn cardiac support device. Left ventricular end-diastolic diameter (LVEDD) in (
Preoperative and Postoperative Left Ventricular Ejection Fraction
Discussion
The Acorn CSD is a textile prosthesis designed to support the heart with only a slight size reduction at implantation. It is not intended to reduce cardiac size acutely and thus, similar to dynamic cardiomyoplasty, it gives no immediate hemodynamic improvement. The prospect of containment to prevent further cardiac dilatation and stop reverse remodeling was deduced from results of dynamic cardiomyoplasty that had been shown to improve the patient's condition by preventing further dilatation (girdling effect). 2 In addition, previous animal experiments showed that cardiac function could be improved by measures to contain the heart. 5,6 However, the material used is of utmost importance. Oh and colleagues 7 employed the relatively stiff Marlex and found that the condition of experimental animals could be improved significantly, but they also showed that Marlex induced constrictive physiology during volume loading. The Acorn CSD composed of extremely elastic woven polyester did not exhibit any constrictive physiology in experimental animals. In a model of progressive heart failure caused by repeated intracoronary microembolization, not only could the deterioration be halted but an improvement occurred a few weeks after surgery. 3 The same improve-ment could be seen in the clinical situation. 8,9
The difference in left ventricular ejection fraction in patients who had the CSD only and those who had concomitant valve repair is of interest. In the valve repair group, only minimal improvement of ejection fraction could be seen over 6 months, while those who had only the CSD showed substantial improvement. However, the preoperative condition of the latter indicated less advanced heart failure. Adverse effects were rare and no patient developed clinical signs of constriction. In a study with repeat cardiac catheterization and recording of pressure volume loops at 3 and 6 months postoperatively, Kleber and colleagues 4 could not detect any constrictive effects although an improvement in systolic and diastolic function was documented. During follow-up in this study, mitral valve repair failed in 2 cases and the valves were replaced at 6 and 8 months after the initial surgery. During repeat surgery, the CSD could be identified easily and adhesions were approximately the same as with any redo operation. Of interest also is the fact that the heart was able to decrease in size on cardiopulmonary bypass. Reoperation was uneventful in both cases and the patients recovered rapidly.
The feasibility and safety of the CSD in patients with heart failure were confirmed by this initial study in which there were no device-related adverse events and a low rate of postoperative complications. A positive trend towards patient benefit was observed, reinforcing the experimental results. Thus, a randomized multicenter trial has been initiated to prove the efficacy of this treatment.
Footnotes
Presented at the 8th Annual Meeting of The Asian Society for Cardiovascular Surgery, Fukuoka, Japan, September 6–8, 2000.