
Abstract
A 4-year-old girl with a congenital pulmonary arteriovenous fistula underwent selective ligation of the fistulous tract with the aid of a preoperatively placed endovascular catheter and cardiopulmonary bypass.
Introduction
Large non-diffuse pulmonary arteriovenous fistulas are conventionally managed either by pulmonary resection or radiological intervention. Surgical resection leads to an undesirable loss of normal pulmonary tissue, whereas radiological interventions are fraught with the dangers of incomplete occlusion, systemic embolization of occlusive devices, and pulmonary infarctions. However, easy intraoperative identification, isolation, and selective ligation of a fistulous tract can be performed successfully with the aid of a preoperatively placed endovascular catheter and cardiopulmonary bypass (CPB).
Case Report
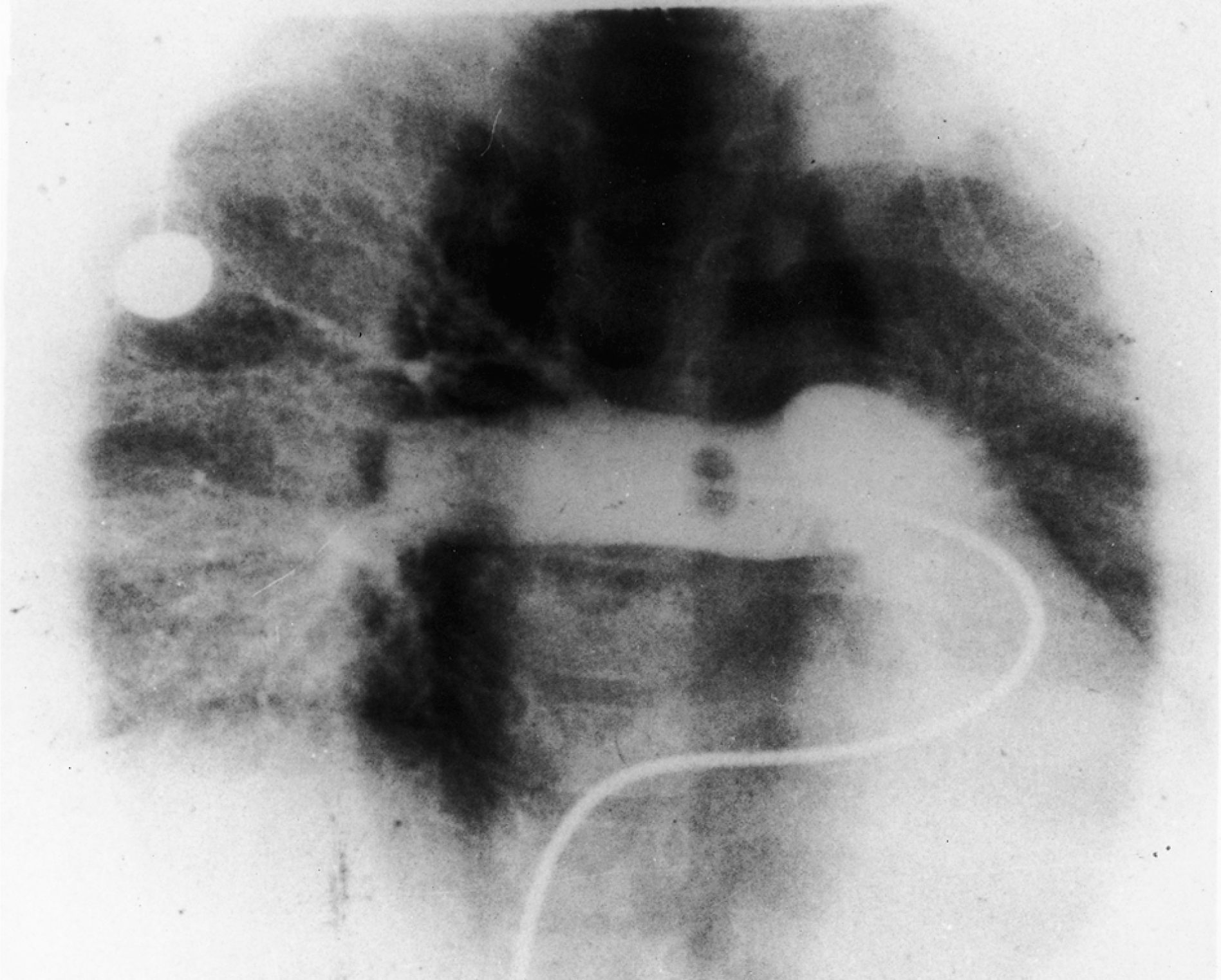
A 4-year-old girl presented with a history of cyanosis since birth and a neurological event in the form of a brain abscess causing seizures and hemipareses. There was no visible telangiectasia, nor a family history of Osler-Weber-Rendu disease. Clinical examination revealed central cyanosis, conjunctival suffusion, and clubbing of the fingers and toes. Chest radiography (Figure 1) showed a right paracardiac homogeneously radiodense shadow. Echocardiography was normal. Contrast echocardiography demonstrated early appearance of the contrast medium in the left atrium, suggestive of a pulmonary arteriovenous fistula. A pulmonary arteriogram (Figure 2) was carried out to confirm the diagnosis of congenital pulmonary arteriovenous fistula. A single large fistula was seen between the interlobar branch of the right pulmonary artery and the proximal right inferior pulmonary vein. A blood sample from the femoral artery showed oxygen saturation of 82%. As the fistula was within the lung, to facilitate its identification during surgery, a 6F flotation balloon catheter was placed across the fistulous tract preoperatively under fluoroscopic guidance (Figure 3). A standard posterolateral thoracotomy was performed in the 5th intercostal space. A large (30 × 10 mm) saclike fistula was seen in the interlobar fissure, within which the previously placed catheter could be palpated. The right pulmonary artery and right inferior pulmonary vein were dilated. The right pulmonary artery was looped for proximal control. Distal control was achieved by opening the pericardium and looping the right-sided pulmonary veins. Clamping these vessels caused tense distension of the sac, making the fistula vulnerable to trauma during dissection. After systemic heparinization, CPB was initiated using aorto-atrial cannulation. This led to decompression of the fistulous sac. Thereafter, the heart was deliberately fibrillated to prevent systemic air embolism that might have occurred due to accidental trauma to the sac with consequent intake of air into the beating left atrium. Thus, safe dissection of the interlobar artery, delineation of its normal branches, and looping of the fistulous tract were made feasible (Figure 4). The balloon catheter was withdrawn from the fistula. The loop around the fistula was tightened and after defibrillation, a trial discontinuation of CPB was made. An immediate improvement in systemic blood oxygen saturation to 100% (on a fraction of inspired oxygen of 50%) was noted. The fistula was doubly ligated in a decompressed state after going back on CPB. The patient was easily weaned off CPB and extubated 6 hours after moving to the intensive care unit. Her postoperative recovery was smooth, and angiography revealed a normally branching right pulmonary artery (Figure 5). The pulmonary veins and left atrium filled only during the levo phase, with no visualization of the fistulous tract. No secondary fistula could be detected. During follow-up, the patient's hematocrit gradually fell from the pre-operative value of 62% (hemoglobin, 190 g·L−1) to 38% (hemoglobin, 125 g·L−1) at 1 year postoperatively.
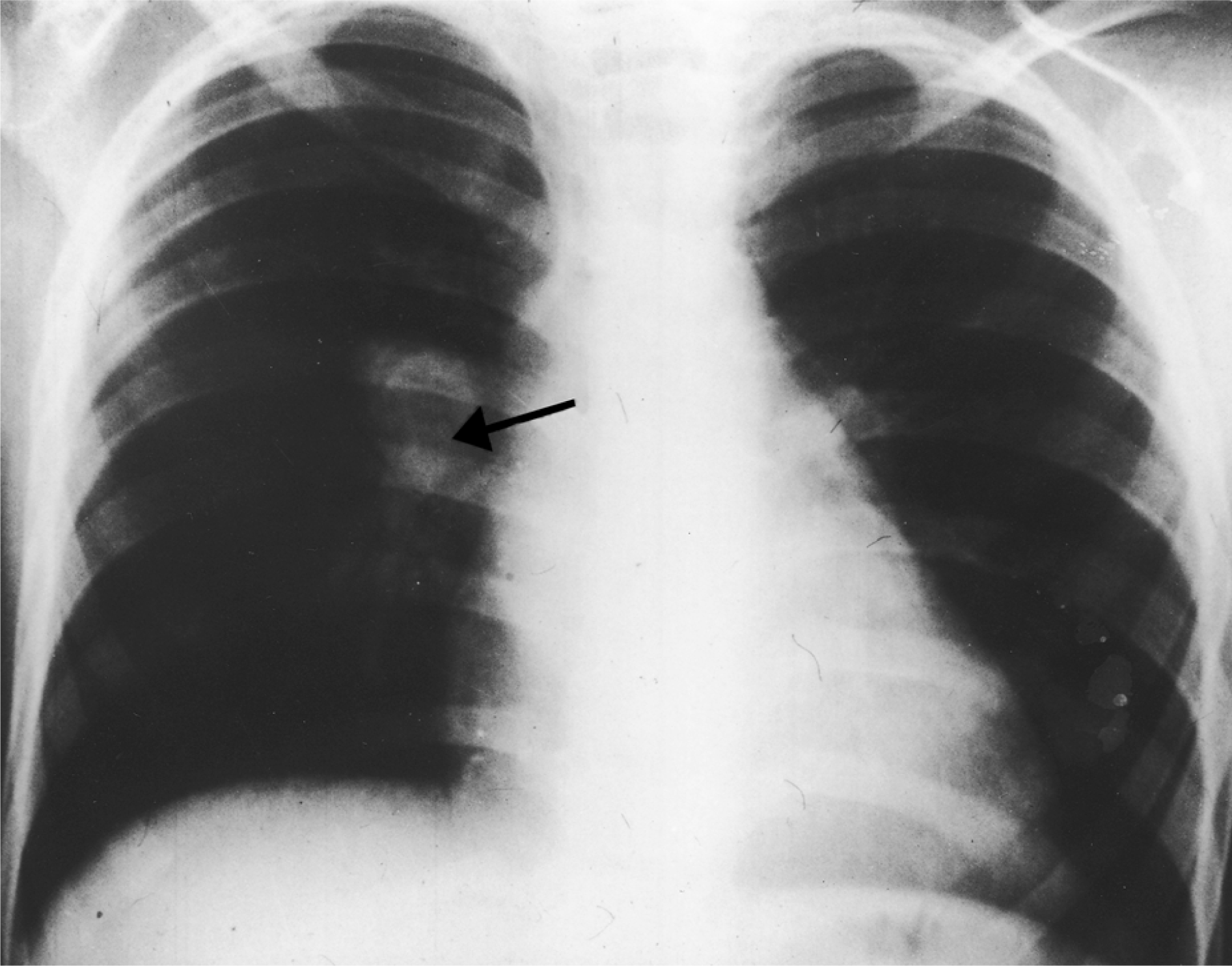
Preoperative chest radiograph in posteroanterior view, showing a large solitary shadow (arrow) in the right paracardiac region.
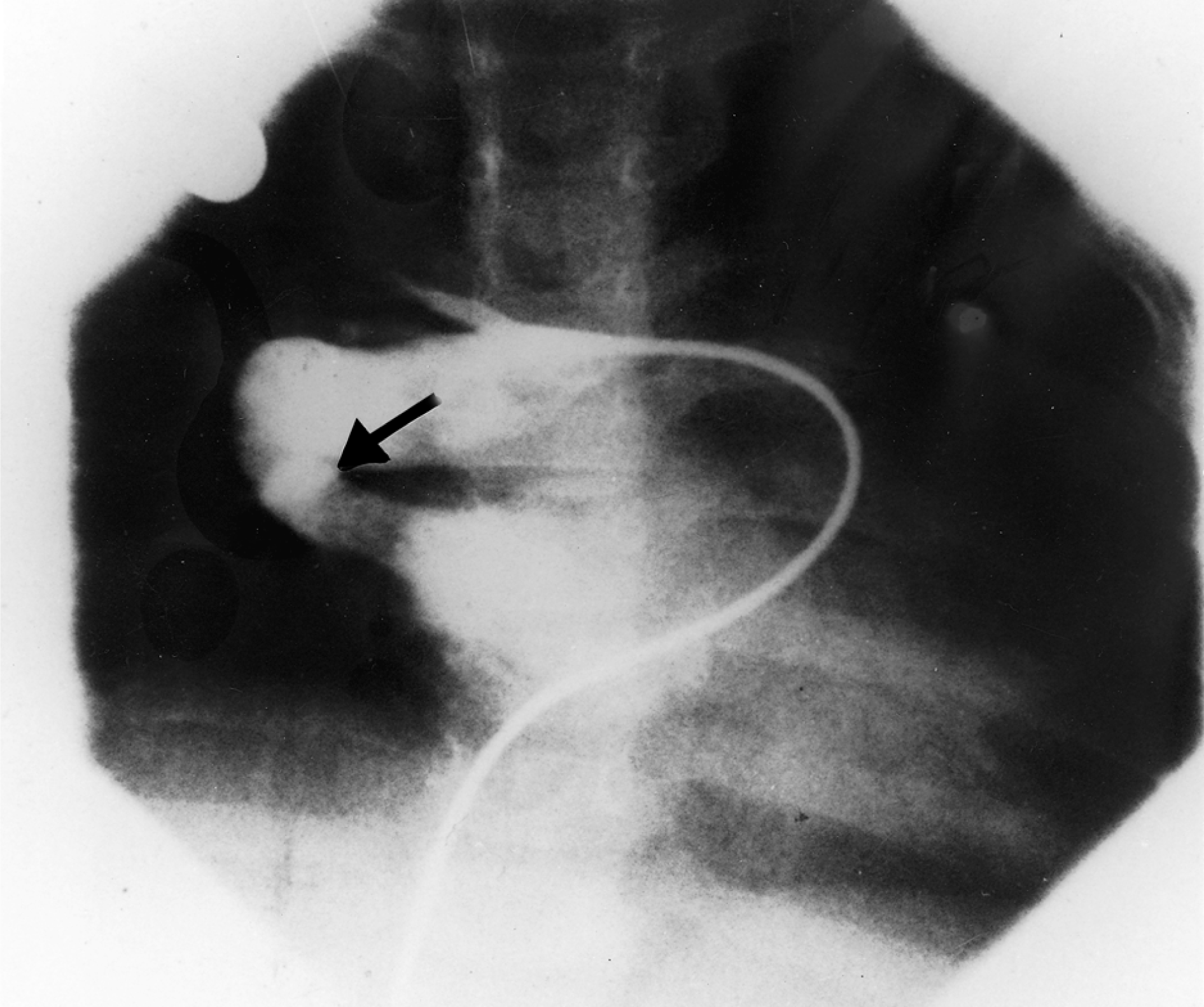
Preoperative arteriogram delineates immediate opacification of the left atrium through the large centrally located pulmonary arteriovenous fistula (arrow).
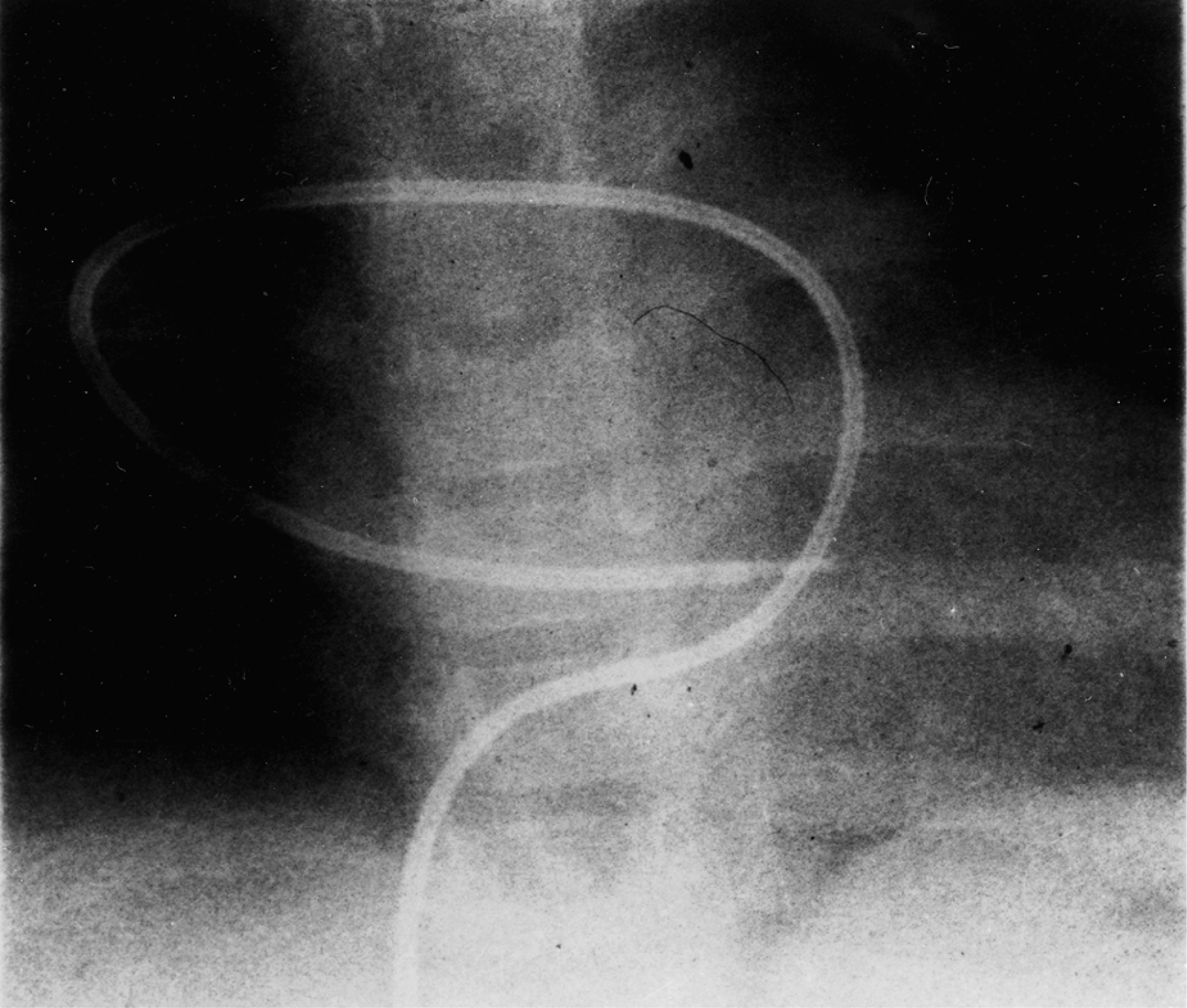
Placement of a catheter across the fistula prior to surgery under fluoroscopic guidance facilitated easy intraoperative identification of the lesion.
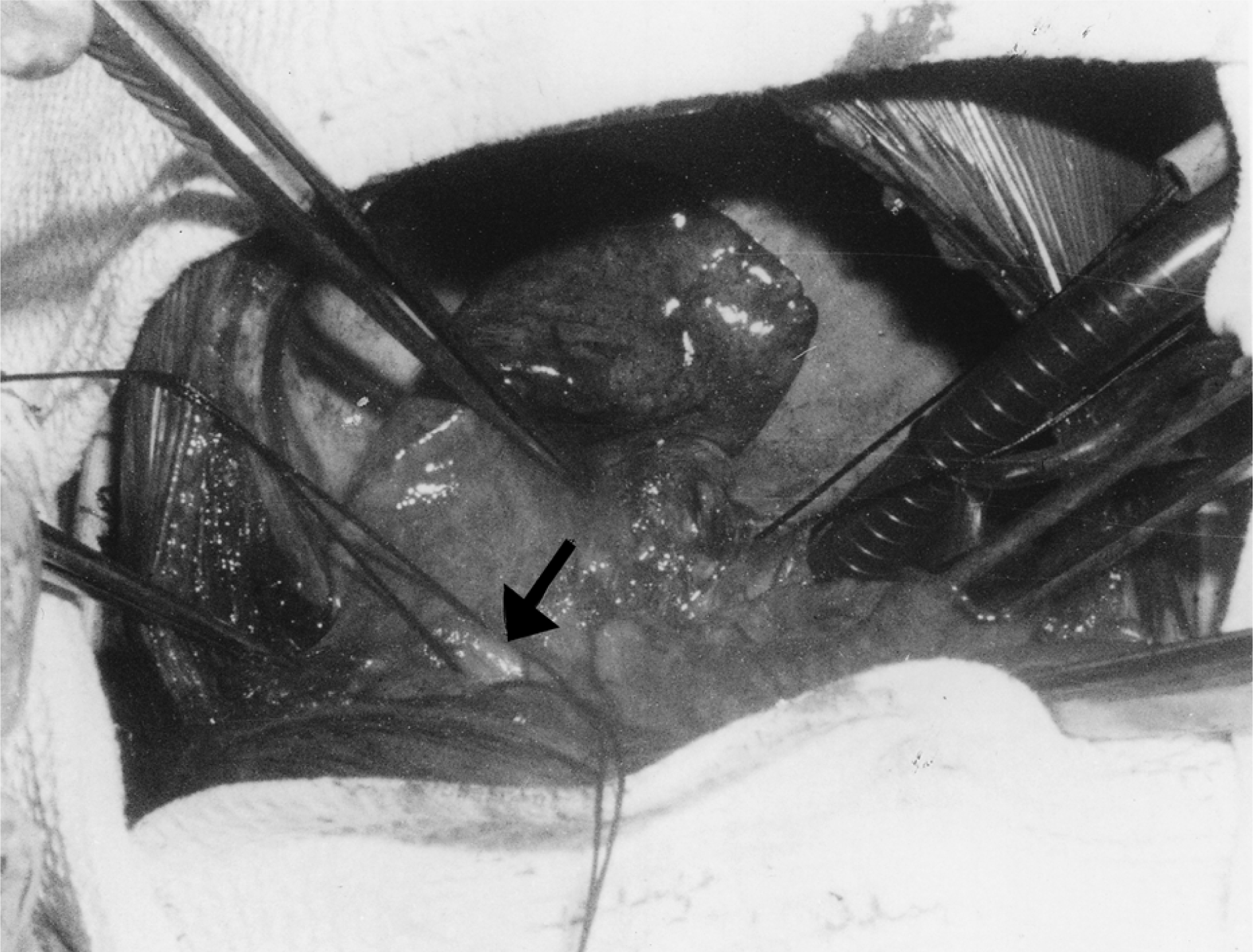
Operative photograph demonstrating the isolated fistula (arrow) looped with silk suture. The pulmonary vasculature is totally decompressed under cardiopulmonary bypass.
Postoperative pulmonary arteriogram showing normal branching of the right pulmonary artery. The left-sided pulmonary veins and the left atrium were seen filling only in the levo phase.
Discussion
Pulmonary arteriovenous fistulas, although uncommon, pose a therapeutic challenge. In 1940, pulmonary resection was proposed as the modality for treating centrally located fistulas. 1 Thereafter, opinion has increasingly favored lung-sparing procedures such as segmentectomy and local excision. In 1976, angiographic embolization was added to the available armamentarium for tackling this entity, further advocating nonoperative treatment of such fistulas. 2 Interventionists have a definite advantage in being able to focus on the localization of the lesion under fluoroscopic guidance, although there are many associated compli-cations, particularly with centrally located fistulas. 3,4
A simple lobectomy could have been performed in this case, but with the intention of complete preservation of the lung tissue, the easily available techniques of endo-vascular catheter placement and CPB were employed. These techniques in the present era of improved safety and efficacy in the conduct of CPB do not subject the patient to any added risk, although there may be differing schools of thought on this issue. In this case where there was a fistula in a low-pressure system (with a limited propensity for recanalization), which was being interrupted in a fully decompressed state, it was thought safe and sufficient to doubly ligate rather than divide and suture. This technique combines accurate localization of the fistula by preoperative placement of the balloon catheter, and precise surgical control of the fistulous tract by maximal decompression of the pulmonary vasculature under CPB. This provides the twin advantages of safe and sure elimination of the lesion and total preservation of normal lung tissue.