
Abstract

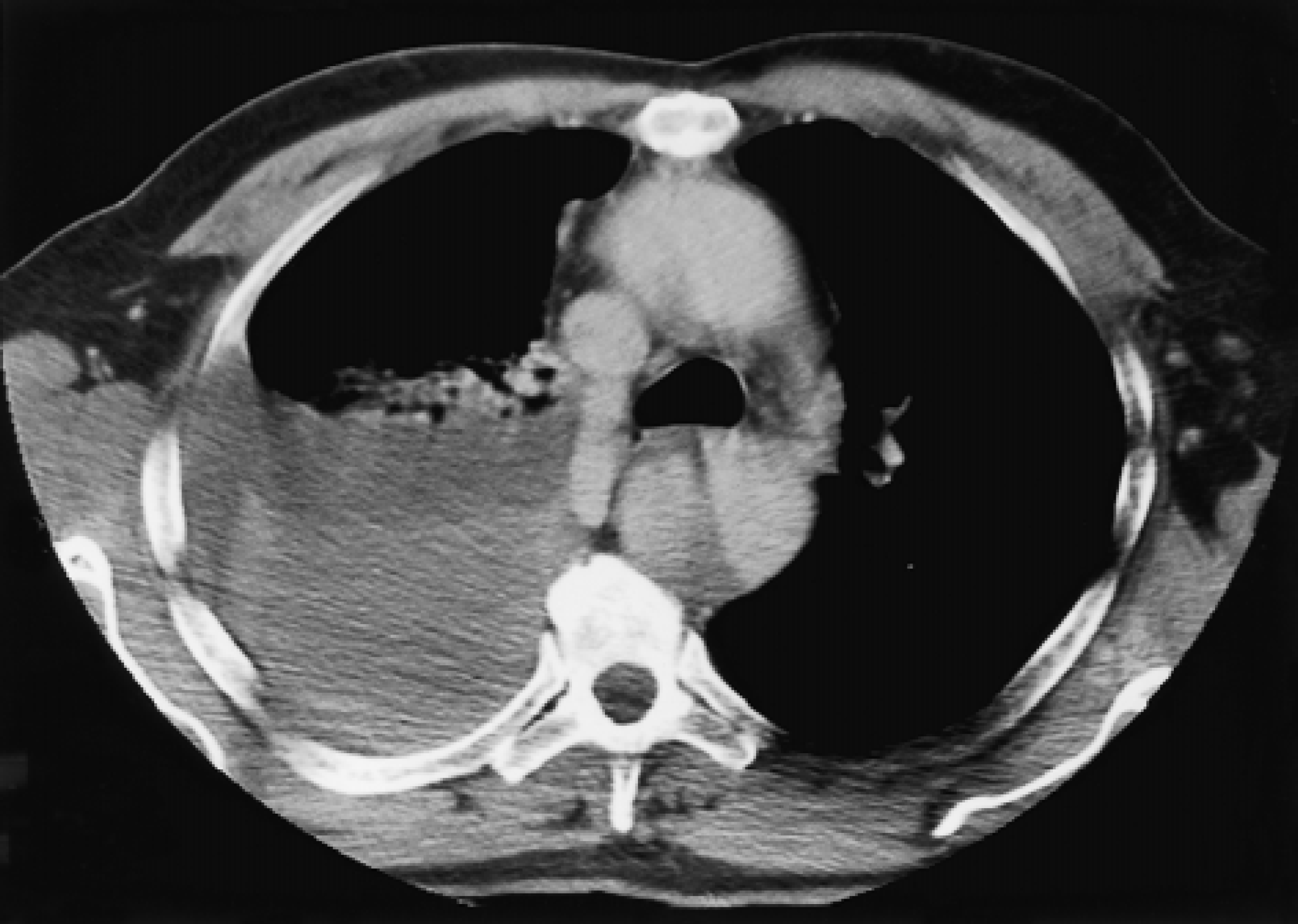
A 62-year-old man presented with acute onset of chest pain and dyspnea. Three years previously, he had undergone aortic valve replacement with a mechanical prosthesis, and 7 months later, the ascending aorta was replaced with an interposition graft for acute type A aortic dissection. Contrast-enhanced computed tomography demonstrated a type B aortic dissection and a right hemo-thorax with a contiguous shadow between the descending aorta and the hemothorax (Figure 1). Severe coagulopathy (international normalized ratio, 7.4) was corrected, the right hemothorax was drained, and the patient was transferred to our unit where he collapsed with further blood loss (2.5 L) from the right chest. Surgery was carried out via a left thoracotomy to replace the descending aorta with an interposition graft under circulatory arrest. The hemothorax was then evacuated through a right thoracotomy. No communication was found between the descending aorta and the right hemithorax. Minimal inotropic support was required postoperatively. The patient recovered well and was discharged after 10 days.
In the context of previous aortic surgery, interpretation of a computed tomography scan can be misleading. Hemo-thorax complicating aortic dissection usually occurs on the left side. In the presence of a right hemothorax, a left thoracotomy is still the approach for surgery on the descending aorta. However, a subsequent right thoraco-tomy to evacuate the blood may be required.