
Abstract
Experience of atrial septal defect closure via a limited posterior thoracotomy is described. From July 1999 to May 2001, 75 prepubertal girls with a median age of 7 years (range, 3 to 13 years) and a median weight of 18 kg (range, 10 to 46 kg) underwent atrial septal defect closure through a limited right posterior thoracotomy. All but 2 patients had an uneventful postoperative recovery. The median duration of ventilation was 13.3 hours (range, 4 to 24 hours). Median hospital stay was 6 days (range, 6 to 8 days). All patients were followed up for 7 to 32 months (mean, 15 months). The wounds healed well without any restriction of limb movement. The limited posterior thoracotomy gave excellent cosmetic results and can be used as a safe alternative approach for atrial septal defect closure in prepubertal females.
Introduction
Improved results with lower mortality and morbidity of surgery for many congenital heart diseases has stimulated renewed interest in surgical approaches to the heart, other than a full midline sternotomy. The primary objective of these alternative approaches is to improve the cosmetic results and shorten the convalescence. However, the concept of cosmesis in cardiac surgery comes into the picture only when the safety of the procedure is beyond doubt. 1 In our institution, a limited right posterior thoracotomy has been employed for atrial septal defect (ASD) closure in prepubertal females, which yields good cosmetic results with standard techniques of cannulation and cardiopulmonary bypass (CPB). The surgical steps and technical modifications for the safe conduct of a limited posterior thoracotomy are described along with an analysis of the outcome.
Patients and Methods
From July 1999 to May 2001, 75 prepubertal females underwent ASD closure through a limited right posterior thoracotomy. Median age was 7 years (range, 3 to 13 years) and the median weight was 18 kg (range, 10 to 46 kg). Sixty-two patients had a fossa ovalis defect, 4 had an inferior vena cava (IVC) type, and 9 had a sinus venosus defect. The ASD closure was performed under fibrillatory arrest in 8 patients and under cardioplegic arrest in the others. During the same period, 965 cases of ASD closure were carried out through a full midline sternotomy, 25 through an anterolateral thoracotomy, and 10 via a partial sternotomy.
As for the standard right posterolateral thoracotomy, the patient was positioned in the left lateral decubitus position with the elbows, knees, and dependent axilla well padded. For the limited posterior thoracotomy, a curvilinear incision was made around the angle of the scapula (Figure 1), avoiding the vertical extent of the standard posterolateral thoracotomy, and limiting the anterior extent of the incision to the posterior axillary line. Only the serratus anterior and latissimus dorsi were incised; the trapezius and the greater rhomboids were not included in the incision. A pad was placed behind the chest to elevate the heart and aorta towards the surgeon. The pleural space was opened through the 4th intercostal space. The lung was retracted posteriorly with a large sponge. The right lobe of the thymus was resected by diathermy dissection. The pericardium was harvested safeguarding the right phrenic nerve. A series of pericardial stay sutures were inserted and anchored to the chest wall with tension. These stay sutures helped bring the heart and mediastinum towards the incision, and kept the right lung retracted. A stay suture in the pericardial fold between the superior vena cava (SVC) and the aorta facilitated visualization of the aorta. Secure fixation of the aortic cannula was considered very important in this procedure. The right atrial appendage was tied with silk and retracted inferiorly to further improve visualization of the length of the aorta. An SVC pursestring suture was placed prior to aortic cannulation. After heparinization, the aorta was partially clamped with a side-biting clamp, and an adequate aortotomy was made. Two pursestring sutures were used for aortic cannulation, and CPB was established with direct SVC cannulation using a right-angled venous cannula (Figure 2). After establishing CPB, IVC cannulation was carried out with a right-angled cannula. The right atrium was opened transversely and the rest of the procedure was similar to that of a median sternotomy approach for ASD closure.
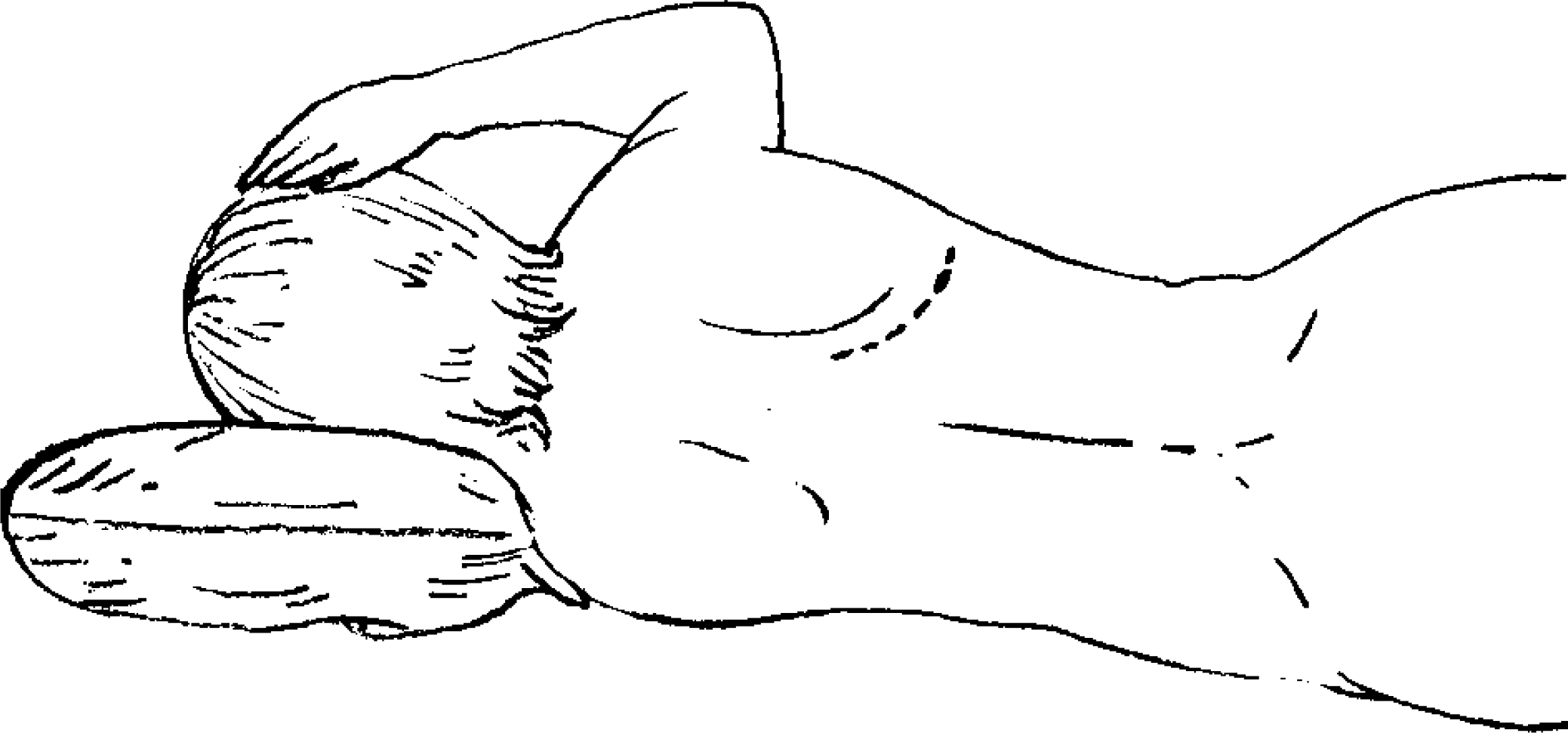
Position of the patient for the limited right posterior thoracotomy.
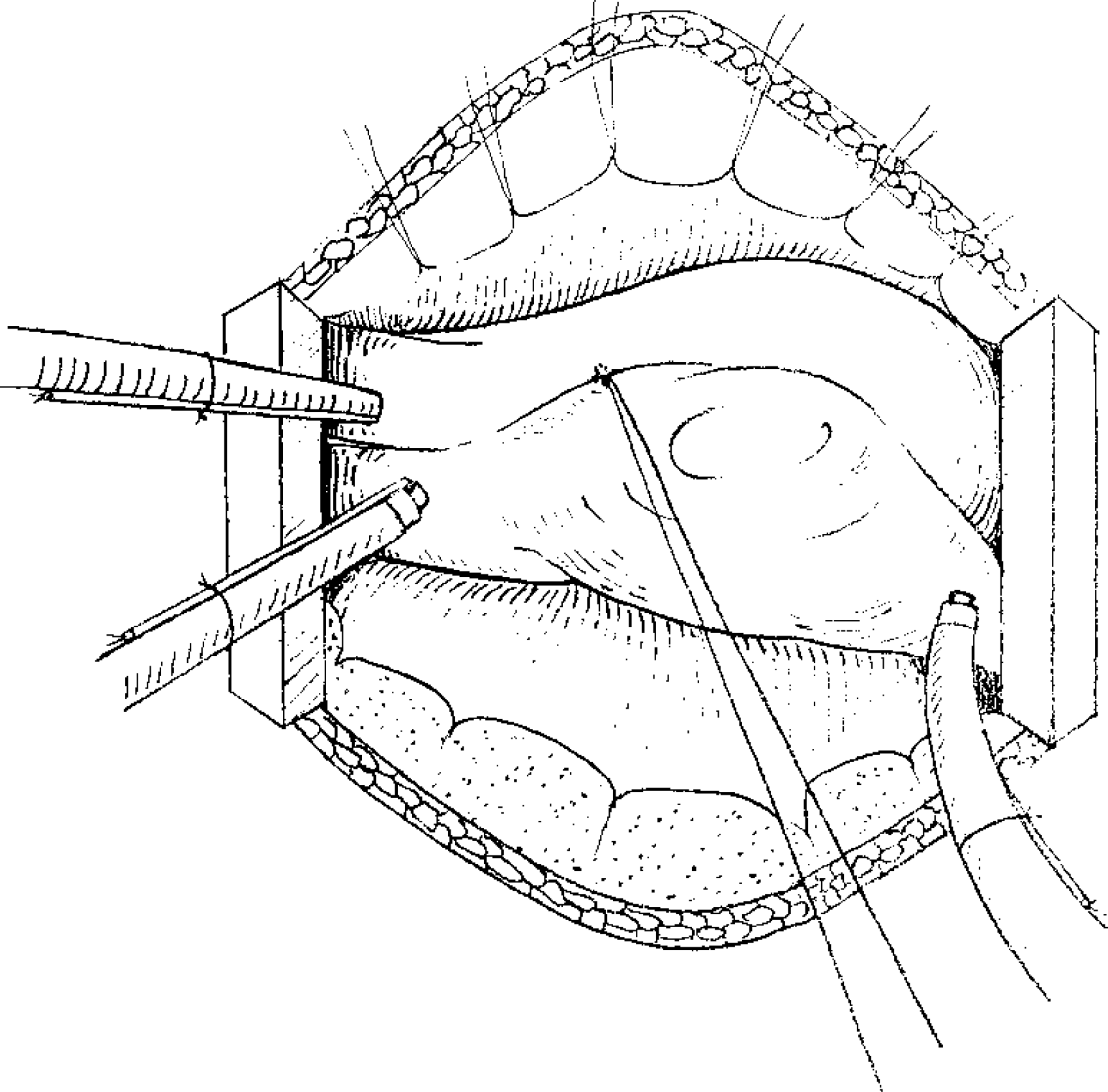
Diagram of the exposure obtained through a limited posterior thoracotomy. The aortic cannula is seen in the cephalad aspect of the field. Caval cannulation is performed with a right-angled tipped cannula.
In 2 patients with an IVC type of defect, the right lower pulmonary vein was found to drain into the upper end of the IVC. The patients were cooled to 18°C and the flow was reduced to 0.5 L·min−1·m−2. The IVC cannula was removed and IVC return was aspirated with a cardiotomy sucker. The defect was repaired with a pericardial patch, with reinstitution of the cannula after ASD closure. Three patients underwent transcaval repair of sinus venosus ASD by this approach. 2 We were able to inspect the mitral valve in 3 patients with mild mitral regurgitation, although none required repair. The presence of a left SVC draining into the coronary sinus was not considered a contraindication to this approach. In 2 patients with a left SVC draining into the coronary sinus, a vent was placed in the coronary sinus and ASD closure was performed by this approach. All patients received a caudal bupivacaine injection prior to surgery. In the postoperative period, they were put on oral analgesics.
Certain technical modifications necessary for the safety of this approach should be highlighted. Direct cannulation of the SVC can be anywhere on the vessel from the lateral aspect of the SVC-right atrial junction upwards, depending on the type of ASD. A simple silk tie on the right atrial appendage helps to retract it and makes aortic cannulation and cardioplegia administration easier. The SVC cannula should be taken behind the aortic cannula before connecting it to the venous line. It is important to retain a fold of pericardium between the aorta and the SVC; posterior traction on this fold facilitates aortic cannulation by improving exposure of the aorta; retracting the fold anteriorly exposes the SVC and aids in cannulation and taping. Cannulation of the IVC was usually carried out with an appropriately sized right-angled cannula after instituting CPB with direct SVC cannulation. Taping should be carried out from the posterior to the anterior of the IVC. A transverse atriotomy aids closure and most defects can be adequately visualized through it.
Results
There were no deaths in the postoperative period. Two patients underwent reexploration because of significant hemorrhage: one had bleeding from the thymic bed; the other had dense adhesions between the lungs and chest wall, which were lysed prior to lung retraction, she had profuse bleeding from chest wall collaterals. The median CPB time was 54 minutes (range, 41 to 94 minutes) and the median crossclamp time was 24 minutes (range, 11 to 42 minutes). This compares well with the CPB time (median, 49 minutes; range, 33 to 90 minutes) and crossclamp time (median, 22 minutes; range, 9 to 40 minutes) needed for ASD closure through a median sternotomy. The median duration of the posterior thoracotomy procedure was 180 minutes (range, 120 to 240 minutes) and this was not significantly higher than the time taken for ASD closure through a median sternotomy (median, 124 minutes; range, 110 to 180 minutes). The median duration of ventilation was 13.3 hours (range, 4 to 24 hours). Median hospital stay was 6 days (range, 6 to 8 days). All patients were followed up for 7 to 32 months (mean, 15 months). The wounds healed well in all patients (Figure 3), with no hypertrophied scars or restriction of right upper limb movement.

The scar from a limited posterior thoracotomy incision in a 4-year-old girl.
Discussion
It is accepted that a median sternotomy provides the best access to the heart. 3,4 However, this incision leaves a visible central scar that can turn hypertrophic or keloidal in patients with intensely pigmented skin, as seen in our country. For better cosmetic results, an anterolateral thoracotomy has been used for various cardiac lesions. 5,6 Although cosmetically superior, experience with the anterolateral thoracotomy over the years has revealed a drawback when it is employed in prepubertal girls. The anterolateral thoracotomy incision occasionally crosses the region of future breast tissue and produces maldevelop-ment of the breast and pectoral muscle. Ipsilateral breast maldevelopment occurs in approximately 7.4% of patients, with periareolar numbness or hypoaesthesia in 38.8%. 5 Tatebe and colleagues 7 described a limited vertical skin incision for median sternotomy. Others have advocated a limited sternotomy for simple cardiac lesions. 8 –10 However, complete visualization of the cephalad structures is difficult with these approaches. Barbero-Marcial and colleagues 11 described a transxiphoid approach for ASD closure, but this requires special instruments and femoral arterial cannulation. The standard posterolateral incision involves a big wound and can impair chest wall development. 12 The recognition of long-term breast and chest wall maldevelopment in prepubertal patients has resulted in a search for an alternative to the standard incisions. A limited posterior thoracotomy, although technically demanding, provides a superior cosmetic result and does not impair future breast or chest wall development. Because of the limited nature of the incision, delayed chest wall maldevelopment is considered unlikely. Our experience indicates that this approach carries no additional morbidity.
The increased technical demand of this procedure is due to the restricted exposure. Meticulous care must be taken to avoid injuring the innominate vein during thymic dissection. Extreme caution is required during fixation of the aortic cannula. Deairing of the leftsided cavities should also be carried out carefully. This is achieved by keeping the cardioplegia site open and filling the left atrium with saline solution until it flows freely from the cardioplegia site, then the anesthetist inflates the lungs to expel any residual air before the continuous polypropylene suture is tied to close the ASD. Applying suction on an aortic root vent is also helpful. Phrenic nerve damage has been reported in as many as 16% of children undergoing ASD closure through an anterior right thoracotomy. 13 In the limited right posterior thoracotomy, the phrenic nerve is encountered during dissection of the SVC and placement of the pericardial stay sutures. The pericardium should be opened at least 1 cm anterior to the phrenic nerve to avoid injury. Access to the aorta and cavae was not a problem in this experience; none of the patients required femoral cannulation.
It was concluded from this study that the limited right posterior thoracotomy carries no additional morbidity and permits closure of an ASD with good short-term results in terms of cosmetic appearance.