
Abstract
Transcatheter coronary arteriovenous fistula occlusion was performed in 5 children with a median age of 5.3 years (range, 0.7 to 11 years). Surgical ligation had been carried out previously in one case, but recanalization occurred during follow-up. Dilation of the feeding artery was observed in 4 patients, with an additional aneurysm of the coronary artery in one of these. Occlusion was attempted three times in 1 patient, twice in 2, and once in the other 2. Detachable balloons were used in 2 procedures, and controlled-release coils in 3. Complete occlusion of the fistula was achieved in 4 patients. In the 5th patient, occlusion of one of two fistulas was unsuccessful, and mild to moderate aortic valve insufficiency developed due to catheter manipulation. Our experience indicates that transcatheter occlusion of congenital coronary arteriovenous fistula is at least as successful as surgical intervention. Multiple occlusion procedures can be avoided by selecting the optimal technique in each case.
Introduction
Congenital coronary arteriovenous fistula is an uncommon anomaly that usually causes no symptoms in young patients but may be associated with congestive heart failure, infective endocarditis, atrial fibrillation, ventricular tachycardia, rupture, angina pectoris, myocardial infarction, and death in older patients. 1,2 Therefore, early surgical closure is generally advocated. Surgery involves a median sternotomy with either epicardial ligation of the fistula or cardiopulmonary bypass and cardiotomy to close the site of drainage. The operation carries low rates of mortality and morbidity. 3 In recent years, catheter-based therapy has been used to occlude these abnormal vascular connections. 4 –8 We describe our experience of transcatheter embolization of coronary fistulas and the problems encountered during the procedures.
Patients and Methods
Between March 1994 and January 2001, 5 patients with a median age of 5.3 years underwent attempted percutaneous transcatheter embolization of coronary fistulas. The clinical data are summarized in Table 1. Surgical ligation had been performed in patient no. 1, but recanalization occurred during follow-up. The youngest patient (no. 3) was taking anti-congestive therapy for intractable heart failure. Two children were referred with palpitations that had been noticed by their families, and there was prominent hypertrophy of the left hemithorax due to cardiomegaly in one of them. Patient no. 5 was asymptomatic and had been referred for evaluation of a heart murmur.
Clinical Data Before Occlusion of Coronary Artery Fistula
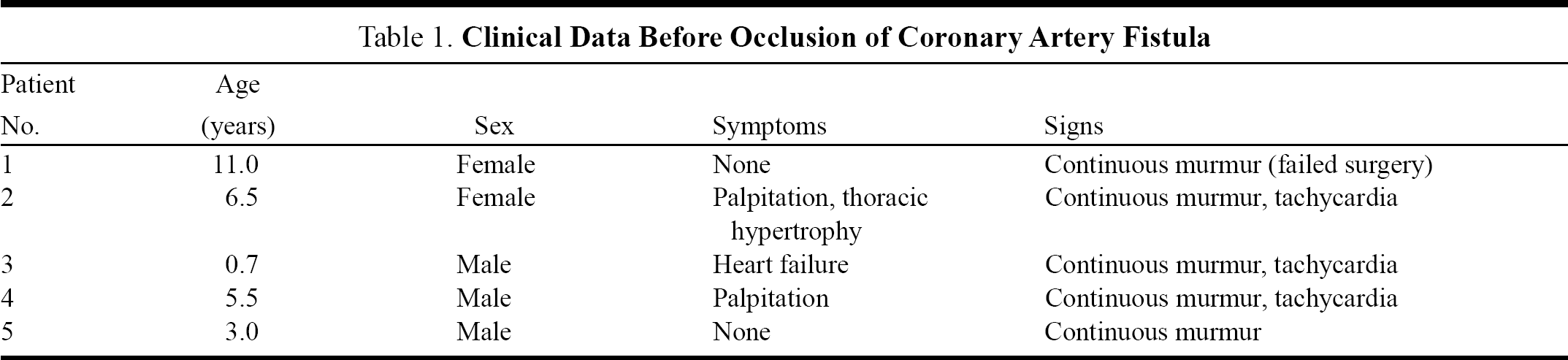
Cardiac catheterization was performed by femoral venous and arterial approaches. Local anesthesia was used in all patients. Heparin prophylaxis for femoral thrombosis was avoided in order to achieve rapid thrombosis in the coils. Selective coronary angiography demonstrated that 3 of 5 fistulas originating in the right coronary artery and 1 of left coronary origin drained to the right side of the heart via a single feeding vessel (Table 2). In patient no. 5, the initial arteriogram showed a single feeding artery from the distal end of the left anterior descending coronary artery to the left ventricle (Figure 1A); the postembolization angiogram revealed another fistula at the end of the second diagonal branch, draining very near to the original fistula (Figure 1B). In patient no. 4, an aneurysmal sac was observed at the distal end of the right coronary artery branch before it drained to the right atrium (Figure 2).
Properties of the Fistulas and Occlusion Techniques
LAD = left anterior descending artery, LCA = left coronary artery, LV = left ventricle, RA = right atrium, RCA = right coronary artery, RV = right ventricle.
(A) Initial angiogram of patient no. 5, demonstrating a single fistulous communication between the left anterior descending coronary artery and the left ventricle. (B) After coil embolization of the left anterior descending artery, another fistula was seen originating from the second diagonal branch of the left coronary artery.

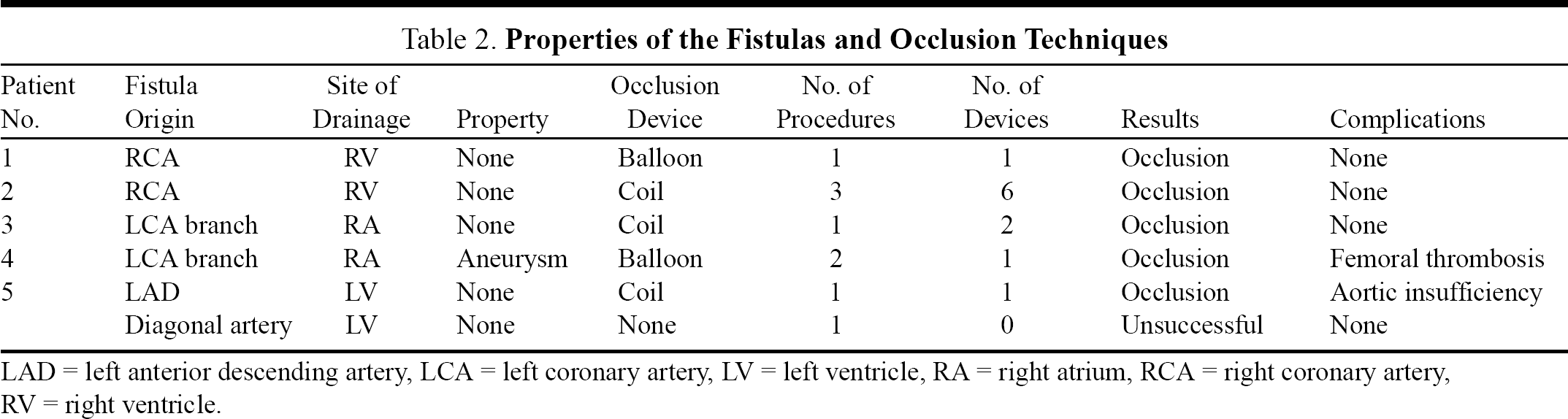
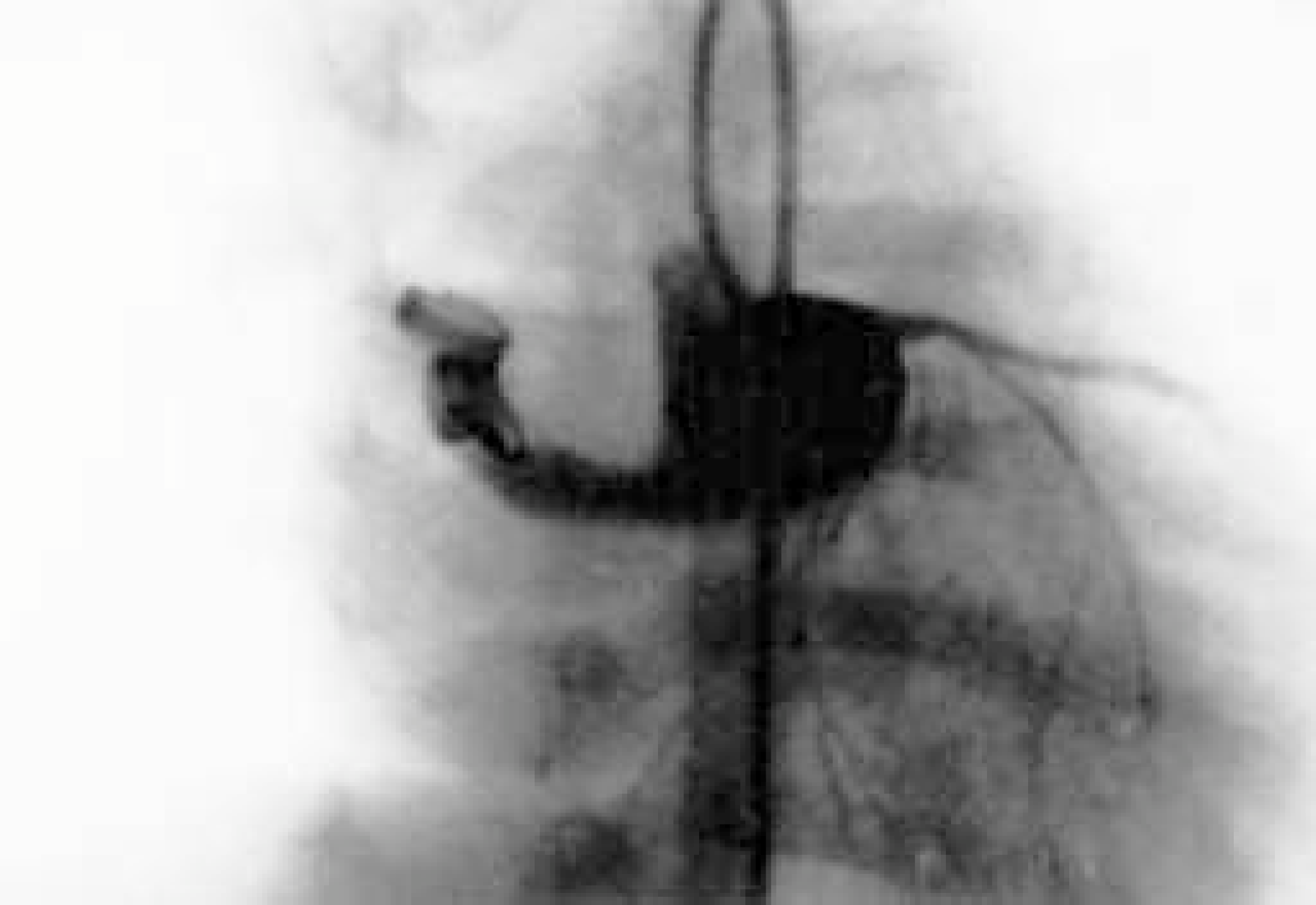
Coronary angiography in patient no. 4, showing an aneurysmal sac in the right coronary artery branch before it drains to the right atrium. Notice that blood flow into the aneurysm is unrestricted.
Occlusion procedures were attempted after ensuring that neither electrocardiographic nor blood pressure changes occurred during a 15-minute test occlusion of the fistulous communication using a Berman balloon catheter (Cook, Inc., Bloomington, IN, USA). A detachable balloon (Haps Emballoon; Haps ICO, William A Cook, Brisbane, Australia) was used to occlude a residual fistula in the first patient (Figure 3) and the distal end of the dilated coronary artery before the aneurysmal sac in the 4th patient. A 6.5F guiding catheter was positioned at the origin of the coronary artery supplying the fistula, and the procedure was performed as described elsewhere. 9 The detachable balloons were inflated with diluted contrast medium. Controlled-release coils, 3- to 8-mm in diameter, with 3 to 5 twists (Cook, Inc., Bloomington, IN, USA) were used to occlude the fistulas in the other patients. A 5F guiding catheter was introduced into the distal end of the coronary artery feeding the fistula. Occlusion was carried out by releasing the coil just in front of the fistula. The number of coils required for complete occlusion ranged from 1 to 6 (Figure 4).
Complete occlusion of a postoperatively recanalized fistula, with a detachable balloon (patient no. 1).
Complete occlusion of a left coronary artery branch-to-right atrial fistula, using 2 correctly positioned coils (patient no. 3).
Results
Post-occlusion angiography revealed complete closure of the fistula after the first catheterization procedure in patient no. 1 in whom a detachable balloon was used, and in patient no. 3 who had 2 coils deployed. In the 5th patient with 2 fistulas, complete occlusion was achieved with a single coil in the left anterior descending coronary artery, but attempts to close the fistula in the diagonal artery were unsuccessful. A second catheterization procedure was performed to close this fistula, but the guiding catheter could not be introduced into the distal end of the feeding artery. In patient no. 4, the initial attempt to occlude the distal end of the coronary artery just before the aneurysm with a controlled-release coil failed when it embolized to the aneurysmal sac before detachment. The coil was retrieved and occlusion was achieved with a detachable balloon in another catheterization procedure a few days later. It was difficult to estimate the exact diameter of the fistula in patient no. 2 because of high blood flow through the fistula. It was decided to occlude this fistula with a 5-mm coil, but it embolized to a peripheral pulmonary artery branch a few seconds after detachment. Without retrieving this coil, the catheterization procedure was terminated after delivering 2 coils (8 and 6.5 mm in diameter) to the distal end of the feeding artery. The patient was catheterized again 3 days later. After transcatheter retrieval of the coil in the pulmonary artery branch, 2 more coils were delivered proximal to those placed initially. A shunt persisted, but the procedure was terminated again because of the expectation of spontaneous thromboembolism. There was no change during 19 months of follow-up, so a third procedure was undertaken. After passing a floppy guidewire through the previously placed coils, 2 further coils were delivered inside the original devices to achieve complete occlusion (Figure 5).

Six coils were necessary for complete occlusion of a wide right coronary artery-to-right ventricular fistula in patient no. 2.
Femoral artery thrombosis occurred in one patient (no. 4), which was responsive to heparin infusion. In patient no. 5 with two fistulas and normal-sized coronary arteries, several attempts were made to catheterize the distal end of the diagonal artery during the first procedure. Post-occlusion echocardiography revealed mild to moderate aortic valve insufficiency that had not been present previously and was attributed to guidewire manipulation; an aortogram during the second catheterization procedure supported the echocardiographic findings. Coronary angiography was not performed in any of the patients during follow-up. Physical examination and electrocardiography showed no evidence of myocardial ischemia during mid- to long-term follow-up. Echocardiography demonstrated the persistence of feeding coronary artery dilation in 4 patients; they remain on low-dose acetyl salicylic acid therapy (80 mg per day).
Discussion
Because a fistulous vessel may gradually enlarge, many patients who are asymptomatic in childhood become symptomatic after the second decade. 10 In their review of 174 patients, Liberthson and colleagues 1 found that 91% of patients younger than 20 years were asymptomatic, compared to 55% of those older than 20 years. Therefore, most investigators advocate early closure of a coronary fistula even in an asymptomatic patient, despite the possibility of spontaneous closure. 11 In view of this recommendation, it was decided to close the fistula in patient no. 5, although he was asymptomatic.
The traditional method of treating coronary fistula has been surgical ligation or internal patching of the orifice. This type of intervention entails at least the inherent risks of a median sternotomy and/or cardiopulmonary bypass and cardiotomy. While surgical fistula closure is relatively safe with a low complication rate in children, operative mortality increases to 7% in adults. 1 Even in very experienced centers, significant complications occur in up to 27% of all patients undergoing surgical closure of an isolated coronary fistula. 3 Recanalization of the main fistulous channel is another potential problem after the ligation procedure, as seen in one of our patients (no. 1). 12 Furthermore, attempts to close a large fistulous channel surgically could result in a small but significant channel being missed (patient no. 5). 13 The cost of the surgical intervention was an additional factor in the development of transcatheter methods.
Advances in catheter and coil technology have made it possible to use 4F or 5F catheters safely in small infants. Mavroidis and colleagues 14 recommended elective coil occlusion in patients who satisfy the following criteria: absence of multiple fistulas, a single narrow drainage site, absence of a large branch vessel, and safe access to the coronary artery (which was not the case in our 5th patient). An aneurysm in the feeding artery, as in our 4th patient, demonstrates another contraindication for coil occlusion, because of the lack of restriction of blood flow. To perform coil occlusion, the guiding catheter should be advanced into or very near to the fistula, either via the coronary artery or a cardiac chamber, to avoid myocardial infarction or embolization that may be life threatening in cases of left-sided drainage. 15 Other techniques using umbrellas or polyvinyl alcohol foam have the same disadvantage. 10,16 –18 Multiple coils may be needed to achieve complete occlusion of large fistulas, and sometimes even of smaller ones, which is another disadvantage. 16 Six coils were used in patient no. 2, so quite a long segment of the distal coronary artery was affected by the occlusion procedure. When a fistula has high blood flow, normal coronary branches may not be clearly visualized because of the “steal” effect of the fistula; these branches may be occluded inadvertently. Thus a detachable balloon seems to be the best mode of treatment in such cases. Advancing the guiding catheter to the distal end is not necessary with a flow-directed detachable balloon when it can be positioned correctly in relation to the direction of blood flow. On the other hand, this technique requires a large guiding catheter that is not suitable for small children with narrow femoral vessels, and there is the possibility of early deflation and peripheral embolization if the balloon is inflated with contrast medium. Therefore, the use of contrast medium is contraindicated for fistulas draining to the left side of the heart.
Our experience shows that transcatheter occlusion of coronary fistula is a safe and effective procedure that is at least as successful as surgical intervention. 15 Nevertheless, the technique may not succeed in every case. It is essential to select the optimal embolization method in relation to the size and location of the fistula, and to have a range of devices available to cope with unexpected requirements and avoid multiple occlusion procedures.