
Abstract
The recommended operative management of unruptured sinus of Valsalva aneurysm consists of closure of the mouth of the aneurysm with or without aortic valve surgery. We report a case of unruptured aneurysm producing right ventricular outflow tract obstruction. Closure of the mouth of the aneurysm failed to relieve the obstruction, which was subsequently achieved by excising the aneurysmal wall overlying the outflow tract.
Introduction
An unruptured sinus of Valsalva aneurysm (SVA) is very rare. It is now accepted that unruptured SVA warrants surgery because of potential complications. The most common complications are caused by compression, leading to right ventricular outflow tract (RVOT) obstruction, complete heart block, or even coronary artery obstruction. Sudden rupture of the aneurysm has also been reported. Surgical treatment involves closure of the mouth of the aneurysm transaortically using a synthetic patch 1 or direct suturing if the mouth is small. 2,3 We report a case of unruptured SVA presenting with RVOT obstruction that could not be relieved by closure of the mouth alone.
Case Report
A 23-year-old man presented with a history of dyspnea on exertion that aggravated to New York Heart Association functional class III in 1 year. On examination, he was hemodynamically stable, although he had frequent ectopic beats at the rate of 6 to 7 per minute. There was a systolic thrill and an ejection systolic murmur over the left parasternal area. The echocardiogram revealed an unruptured SVA compressing the RVOT extending from the infundibular area to the main pulmonary artery across the pulmonary valve. The magnetic resonance image (Figure 1) and computed tomographic scan (Figure 2) revealed the size and extent of the clot-filled aneurysm.

Magnetic resonance image showing aneurysm of the sinus of Valsalva compressing the right ventricular outflow tract. aa = ascending aorta, C = clots in the aneurysm, lpa = left pulmonary artery.
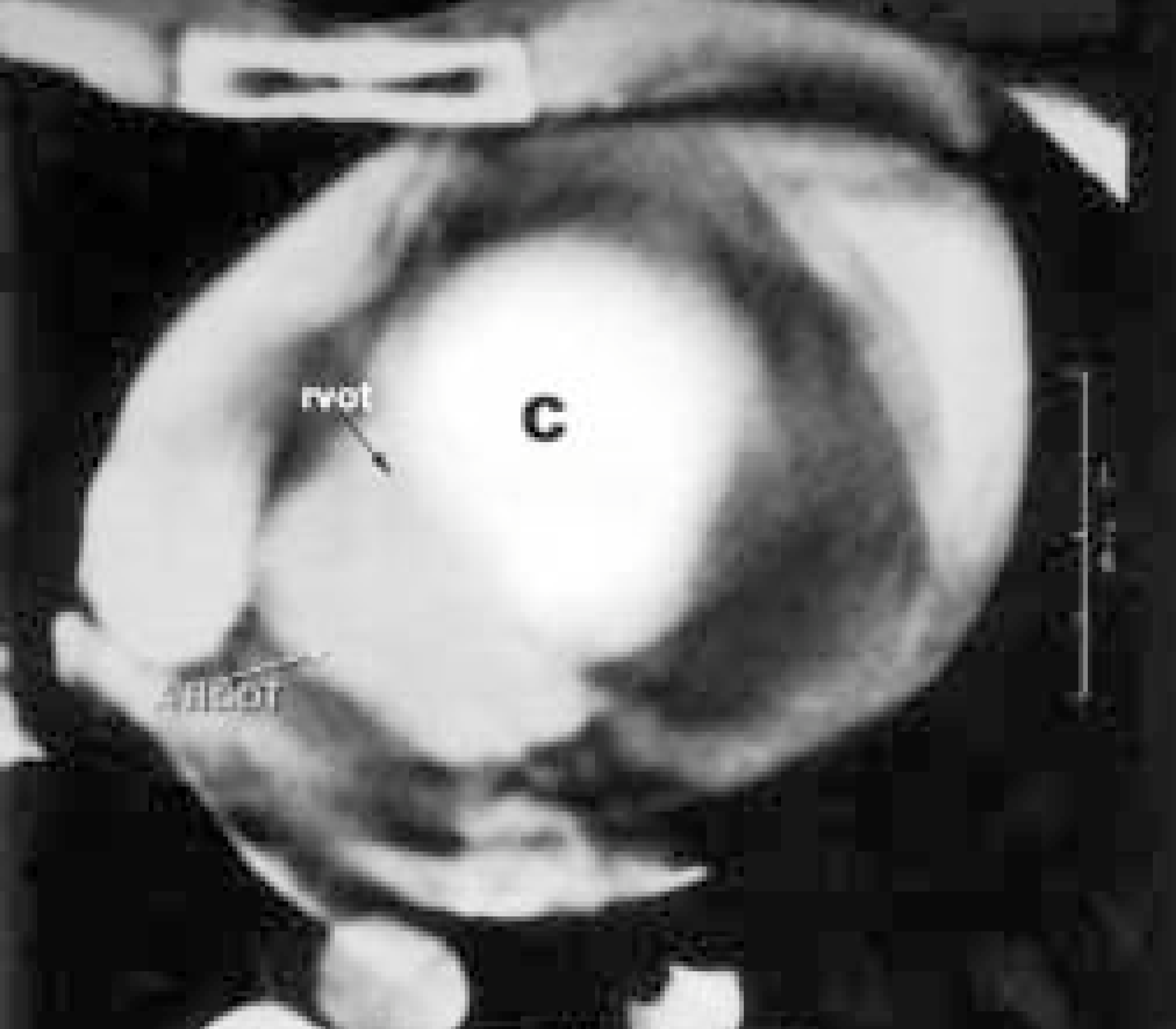
Computed tomographic scan showing the sinus of Valsalva aneurysm arising from the aortic root. AROOT = aortic root, C = clots in the aneurysm, rvot = right ventricular outflow tract.
Early surgery was decided as the patient was symptomatic. A median sternotomy was made and cardiopulmonary bypass (CPB) established cannulating the aorta and venae cavae. Retrograde cardioplegic arrest was achieved after aortic crossclamping. Aortotomy was performed and the mouth of the aneurysm exposed. It was about 1 cm in diameter and in the right sinus of Valsalva. The aneurysm was filled with organized clots. The clots were completely evacuated, and the mouth of the aneurysm was closed with a Gore-Tex polytetrafluoroethylene patch (WL Gore & Associates, Flagstaff, AZ, USA). The aortotomy was closed after deairing, and the crossclamp was removed. However, the patient could not be weaned off CPB. Perioperative transesophageal echocardiography revealed complete closure of the mouth of the aneurysm but that the RVOT obstruction was not relieved. The aneurysmal wall compressing the RVOT was unyielding.
The patient was cooled again, the aorta crossclamped, and the heart arrested with cold cardioplegia. The right atrium was opened and the RVOT inspected. The roof of the RVOT was bulging down, causing narrowing from the middle of the interventricular septal area to 2 cm from the free wall of the RVOT transversely and from the crista to the pulmonary artery. From the outside, the RVOT was obscured by the aneurysm. The aneurysmal wall overlying the RVOT was opened longitudinally. It led to the aneurysmal sac, which was around 12 × 3 cm in size and ovoid-shaped, covering the whole infundibular area of the right ventricle and the anterior aspect of the pulmonary artery. The Gore-Tex patch used to close the mouth of the aneurysm was seen on the medial wall of the aneurysm. Distally, the aneurysm extended beyond the pulmonary valve. The posterolateral aneurysmal wall that was obstructing the RVOT was excised along with the anterior pulmonary leaflet. As the Gore-Tex patch was exposed directly to the RVOT, it was supplemented with a pericardial patch. The RVOT was widened with a pericardial patch and closed.
Subsequently, the patient came off CPB with minimal inotropic support, and inotropes and ventilation could be withdrawn in 6 hours. The postoperative course was uneventful, and he was discharged on day 8 after surgery.
Discussion
SVA was first described in 1840. It is very rare, accounting for only 0.14% to 1.5% of cardiac operations. 4 The incidence in Asian populations is reported to be about 5 times higher than in the West. 5 It is usually congenital and arises from a single sinus as a result of separation of the aortic media and the annulus fibrosus of the aortic valve. Deficiency of normal elastic tissue of the aorta and abnormal development of the bulbus cordis are implicated in the development of SVA.
Unruptured SVA is rare and is usually asymptomatic, unless it causes compression or ruptures suddenly. Its extent can best be assessed with magnetic resonance imaging, while echocardiography will give a diagnosis with 75% accuracy. Since the aneurysm is filled with clots, angiography may not give an accurate assessment of the size.
Only in very few cases was the compression not relieved by closing the mouth of the aneurysm alone, 6 as in this case. Probably, the long-standing compression and organized clots led to dense fibrosis, which prevented the RVOT from dilating. As the part of the aneurysm overlying the RVOT could not be dissected off the myocardium safely, the obstructing aneurysmal wall had to be excised and the RVOT then reconstructed using a pericardial patch. From this experience, we suggest inspection of the RVOT through the right atrium before removing the crossclamp, which will help to identify persistent obstruction.