
Abstract
As peroneal artery bypass surgery is technically demanding, a simplified medial approach was used in 23 peroneal artery reconstructions in 21 patients between January 1993 and December 2001. The outcomes were reviewed retrospectively. Peroneal artery reconstruction was undertaken through a medial skin incision using tourniquet occlusion and saphenous vein grafts. Graft patency was confirmed by angiography or duplex color imaging. Peroneal bypass was possible through the medial approach in 20 cases; in 1 limb, the target was occluded. During a mean follow-up of 43.9 months, there were 4 graft occlusions. None of the failures was due to a technical error related to the procedure. All of the other patients had relief of their symptoms, including those who presented with disabling claudication. Technical improvements have made peroneal bypass a reasonable choice in below-knee arterial reconstruction. This technique should not be restricted to limb salvage.
Introduction
Distal peroneal artery reconstruction can be performed via the lateral approach which requires segmental resection of the fibula. 1 –5 Although most investigators insist that there is little difficulty in walking without the fibula, we chose to undertake peroneal artery reconstruction via a medial approach. 6,7 Using this technique, partial fibular resection is unnecessary, the saphenous vein harvest and anastomoses can be carried out through a single skin incision, and the entire peroneal artery can be isolated. Application of a tourniquet facilitates the anastomotic procedures without the need for clamps that can obscure the operative field. 8 –10
Patients and Methods
Between January 1993 and December 2001, 23 peroneal artery bypass operations were performed in 21 patients, accounting for 32.4% of the tibial artery bypass operations carried out in our institution during this period. The results were reviewed retrospectively. There were 19 men and 2 women, their mean age was 66 years (range, 51 to 83 years). Associated diseases comprised diabetes mellitus in 7 patients, chronic renal failure necessitating hemodialysis in 4, arrhythmia in 5, ischemic heart disease in 2, and cerebral infarction in 2. Preoperative assessment included angiography, ankle brachial pressure measurement, and duplex color scanning in each patient. The etiology of arterial occlusion included arteriosclerosis obliterans (20 limbs) and embolism (3 limbs). The patients in whom embolism was thought to be the etiology had acute onset of symptoms, smooth inflow arteries on their angiograms, and associated arrhythmia. Preoperative symptoms were severe disabling intermittent claudication (7 limbs), intolerable pain at rest (5 limbs), and incurable ulcer or gangrene (11 limbs).
Peroneal bypass was performed when the femoral or popliteal artery was appropriate as an inflow artery with or without proximal reconstruction, and the peroneal artery alone was patent below the knee, with a patent foot artery via the perforator above the ankle. Concomitant arterial inflow reconstruction was undertaken in 11 limbs. All approaches to the peroneal artery were through a medial skin incision. 6,7 However, the target portion of the peroneal artery was occluded in one limb, thus the bypass was performed over the anterior aspect of the fibula through an incision in the interosseous membrane. After the medial skin incision, the soleus muscle was incised and dissected from the tibia. The posterior tibial artery and veins were noted on the surface of the flexor digitorum longus muscle. The flexor hallucis longus muscle was isolated from the posterior tibial vessels and retracted posteriorly. The peroneal artery and veins were identified on the surface of the posterior tibialis muscle (Figure 1). The posterior tibial vessels were retracted posteriorly or anteriorly, depending on branch location. 7,10 The proximal portion of the peroneal artery was approached by dividing the arch of the soleus muscle and dissecting towards the distal tibioperoneal trunk. The entire peroneal artery was thus isolated through the medial skin incision. The anastomoses were created using tourniquet occlusion techniques. 8 –10 Early in the study period, a rubber Esmarch bandage was used as a substitute for vascular clamps, thereafter, a sequential pneumatic tourniquet was employed. In some cases, a roll cuff (Rool Manchette; Pomidor AB, Varnamo, Sweden) was used. In each case, the proximal side was occluded using a standard air-inflated tourniquet. Graft patency was confirmed by angiography or duplex color imaging at the last follow-up examination. Graft patency rates were analyzed by the Kaplan-Meier method.
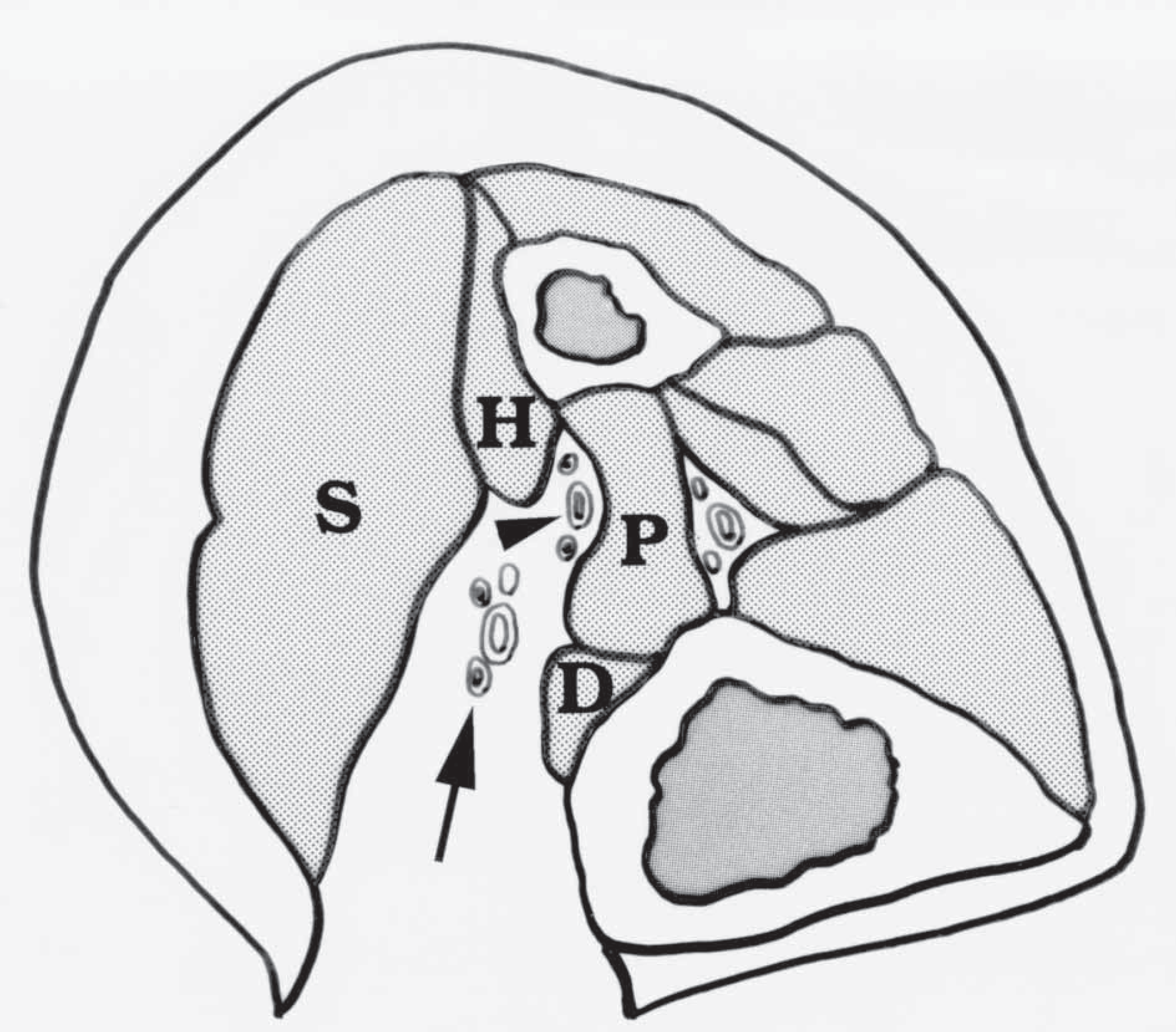
Medial approach to the peroneal vessels: the soleus muscle (S) is retracted posteriorly and the posterior tibial artery and veins (arrow) are observed; the flexor digitorum longus (D) and flexor hallucis longus (H) are divided beside the posterior tibial vessels; the peroneal vessels (arrow head) are observed on the posterior tibialis muscle (P). The peroneal and tibial arteries usually run between the identical veins.
Results
Using the medial approach and tourniquet occlusion, vascular clamps that could obscure the operative field were unnecessary. The field was completely bloodless. The anastomoses were created with ease in the deep narrow field.
The mean follow-up period was 43.9 months (range, 1 to 94 months). There were 4 graft occlusions, and no revision was performed. The primary and the secondary patency rates were 90.4% and 90.4% at 1 year, and 79.7% and 79.7% at 5 years, respectively. The first graft occlusion was due to infection in a patient who died of septicemia after an emergency amputation. Another graft was occluded at 1 year postoperatively in a diabetic patient with poor glucose control. This patient underwent repeat bypass to the anterior tibial artery. A graft occlusion was noted at 1 year due to compression by the tendon of the gastrocnemius muscle in a patient who was asymptomatic. The last graft occlusion occurred at 32 months in a patient who had undergone 3 reconstructions due to repeat occlusion. At the last check-up, the patient complained of coldness of the foot but could walk without symptoms. All 19 limbs in which there was a patent graft were symptom-free, including those in which disabling claudication was the presenting complaint. Postoperative angiography showed an increase in blood flow to the calf via the posterior tibial artery. Direct or indirect blood flow to this artery was observed above the ankle through perforators from the peroneal artery (Figure 2).
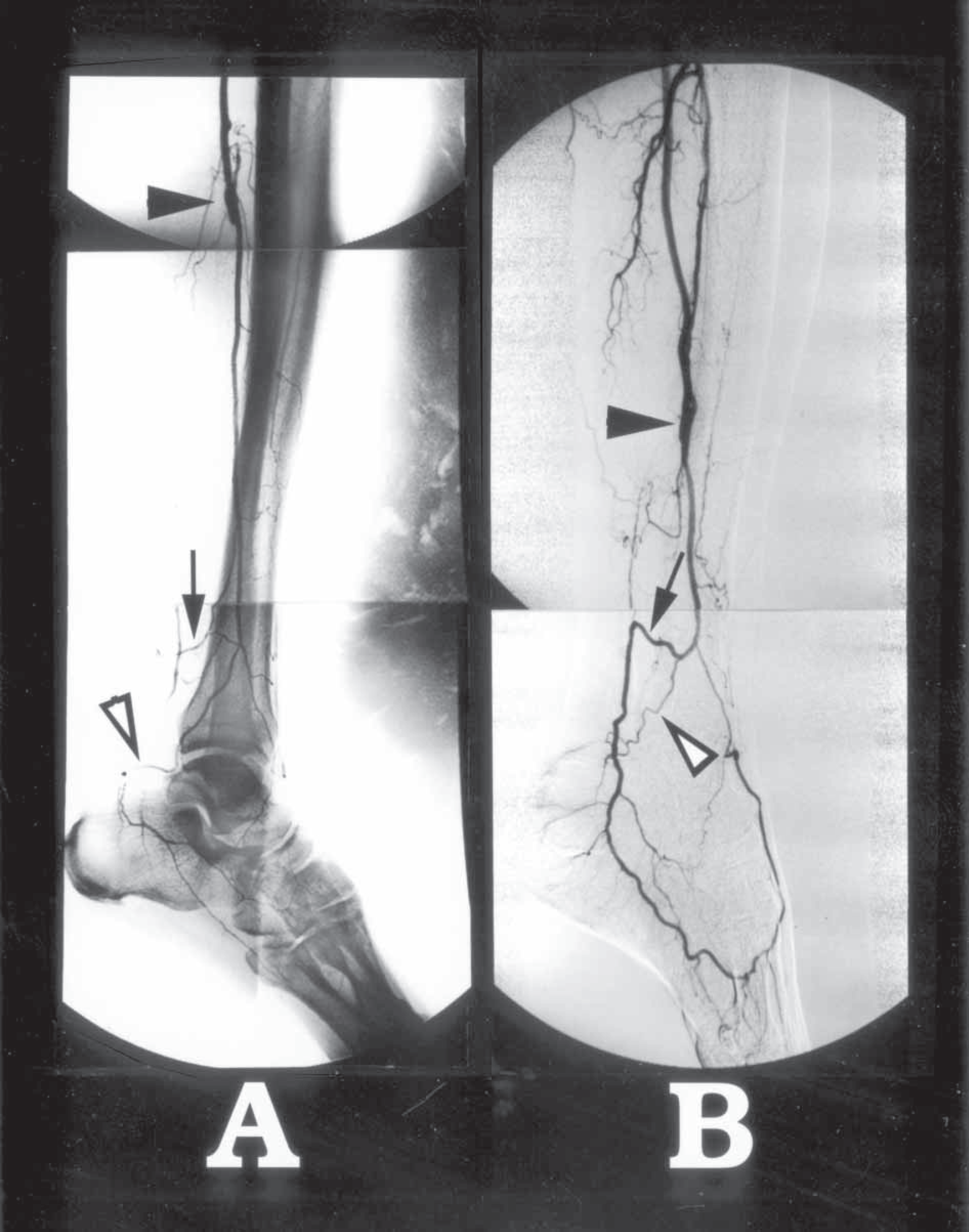
Angiography after peroneal artery reconstruction: (
Discussion
Tibioperoneal bypass surgery is frequently indicated for salvage of an ischemic limb. 11,12 When both the tibial and peroneal arteries are patent, posterior tibial artery reconstruction is preferred. 13,14 Tibial artery bypass is selected because of the greater density of muscular branches and the ease with which the vessels can be isolated and the anastomoses created. 15 However, the peroneal artery is sometimes less severely diseased and hence more suitable for bypass. 7 The success of peroneal artery reconstruction often determines the prognosis for the extremity. Therefore, technical improvements in peroneal artery reconstruction are of significant value.
Since Elkin and Kelly 16 first used fibulectomy to treat an arteriovenous fistula of the peroneal artery in 1945, the distal portion of the vessel has been approached through a lateral incision with segmental resection of the fibula. 1 –5 Most investigators have reported minimal morbidity following resection of the fibula. However, if bone resection is unnecessary for vascular isolation, it should not be performed. This may be of significant benefit in the elderly and in patients with osteoporosis. Moreover, eliminating the bone resection would simplify the approach to the peroneal artery. The peroneal artery is easily approached through a medial incision. Bone resection is unnecessary and the graft adopts a smooth anatomic path. Furthermore, the required graft length is shorter with the medial approach than with the lateral approach, and the saphenous vein harvest and anastomoses can be performed through a single skin incision. The tourniquet occlusion technique enables creation of the anastomoses in a bloodless field without interference from vascular clamps. Using these techniques, peroneal artery bypass surgery is as easy as posterior tibial bypass surgery.
In the 4 patients with occluded grafts, no technical errors related to the described procedures were identified. There was one early occlusion but the cause of graft failure was infection. Intimal hyperplasia at the anastomosis was not observed in the 3 late failures. Similar observations have been made in other patients who have undergone tibial bypass surgery at our institution. 17 Although clear evidence is not available at this time, minimizing arterial injury at the anastomoses appears to prevent late complications.
Peroneal bypass surgery for limb salvage in patients with critical ischemia is accepted by most vascular surgeons, although some remain skepticial. 12 –14 Most of our patients underwent surgery for critical limb ischemia. On the other hand, Raftery and colleagues 18 reported the hemodynamics of peroneal artery bypass to be equivalent to other tibial bypasses. Still, the indications for peroneal artery bypass for claudication are controversial. 19 This is in part due to the fact that there are few muscular branches from the peroneal artery. However, the perforators from the peroneal artery above the ankle connect directly or indirectly to the posterior tibial artery (Figure 2). Thus blood flow to the calf muscle is increased after peroneal artery bypass via the posterior tibial artery. Preoperative angiography frequently fails to demonstrate these connections because of low inflow. Consequently, the decision to revascularize the peroneal artery for claudication is not easily made before surgery. Patient selection is therefore critical. When the peroneal artery is the only patent artery in the calf and ischemic claudication is present, peroneal artery reconstruction is indicated even if blood flow to the calf via the peroneal artery is not demonstrated preoperatively. An increase in flow in the peroneal artery eventually augments the blood supply to the calf muscles. In our experience, all patients suffering from claudication were able to walk without pain after peroneal artery bypass. Peroneal artery bypass should therefore not be restricted only to limb salvage.