
Abstract
Two patients with neurofibromatosis presented with expanding masses at the left supraclavicular region. Computed tomography (CT) scans revealed vascular masses. The patients underwent surgery and ruptures of the left subclavian artery were found. Both patients were treated by ligation of subclavian artery.
Introduction
Neurofibromatosis type I, an autosomal dominant neurocutaneous disorder, is carried on chromosome 17 and involves the peripheral nerve sheath. Vascular complications, especially spontaneous rupture of a major artery, are rare. There are three reported cases of left subclavian aneurysms in the literature. The appropriate treatment for these complications involves surgery or an intraluminal stent graft.
Case Report
Case I
A 46-year-old woman with neurofibromatosis presented with an expanding mass, experienced at the left supraclavicular region for 5 days. A progressive weakness and numbness developed in her left hand and forearm. She also experienced pain in the left supraclavicular area. There was no prior history of trauma. A physical examination showed a tense tender left supraclavicular mass, 10 × 12 cm. There was a sensory deficit in the left hand and forearm, and the motor power was grade IV/V. The left radial pulse was decreased. A chest CT scan revealed a hematoma in the left supraclavicular region and a moderate left pleural effusion (Figure 1). Angiography revealed leakage from the left subclavian artery near the origin of the thyrocervical trunk (Figure 2).
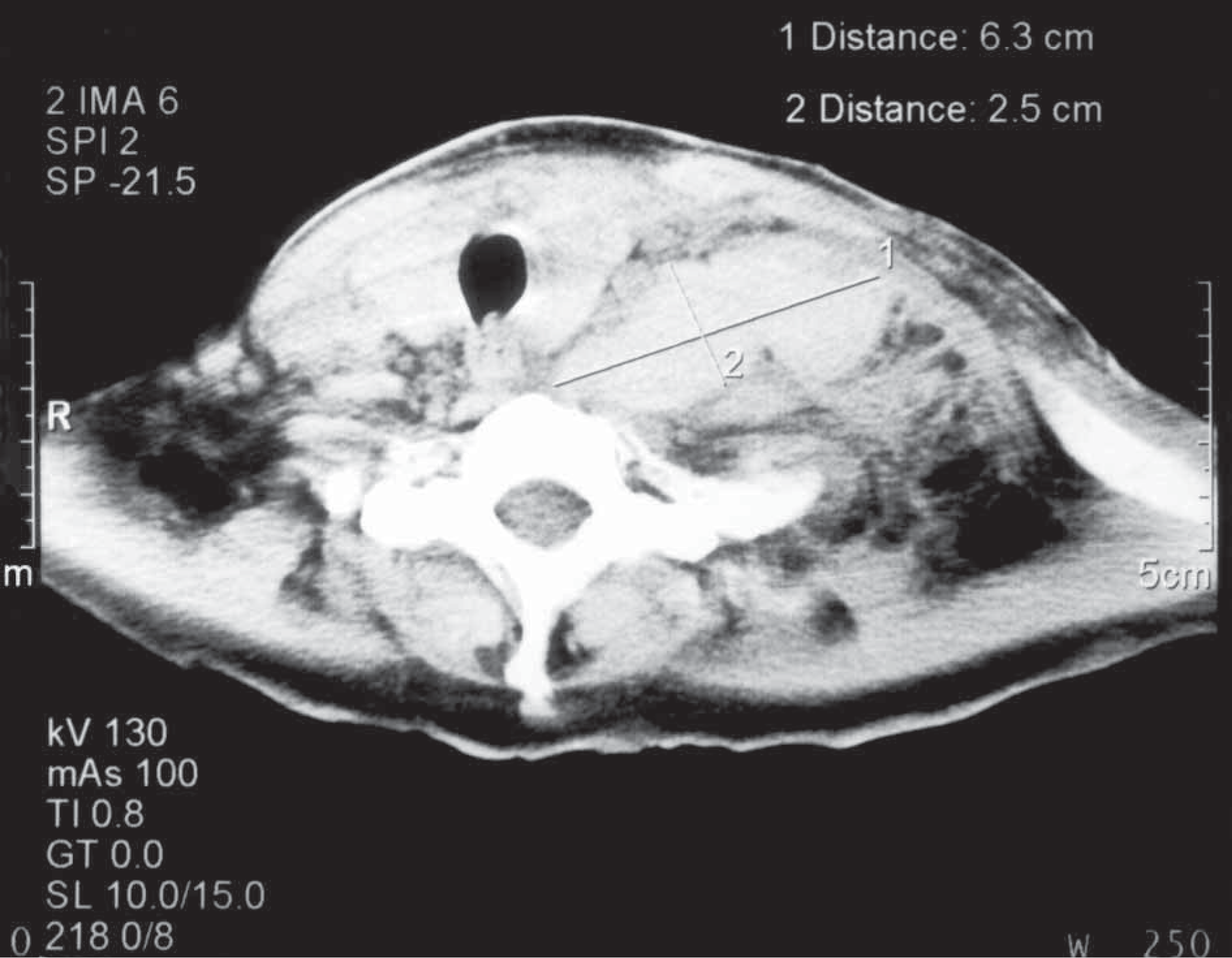
Computed tomography showing a hematoma at the left supraclavicular region.
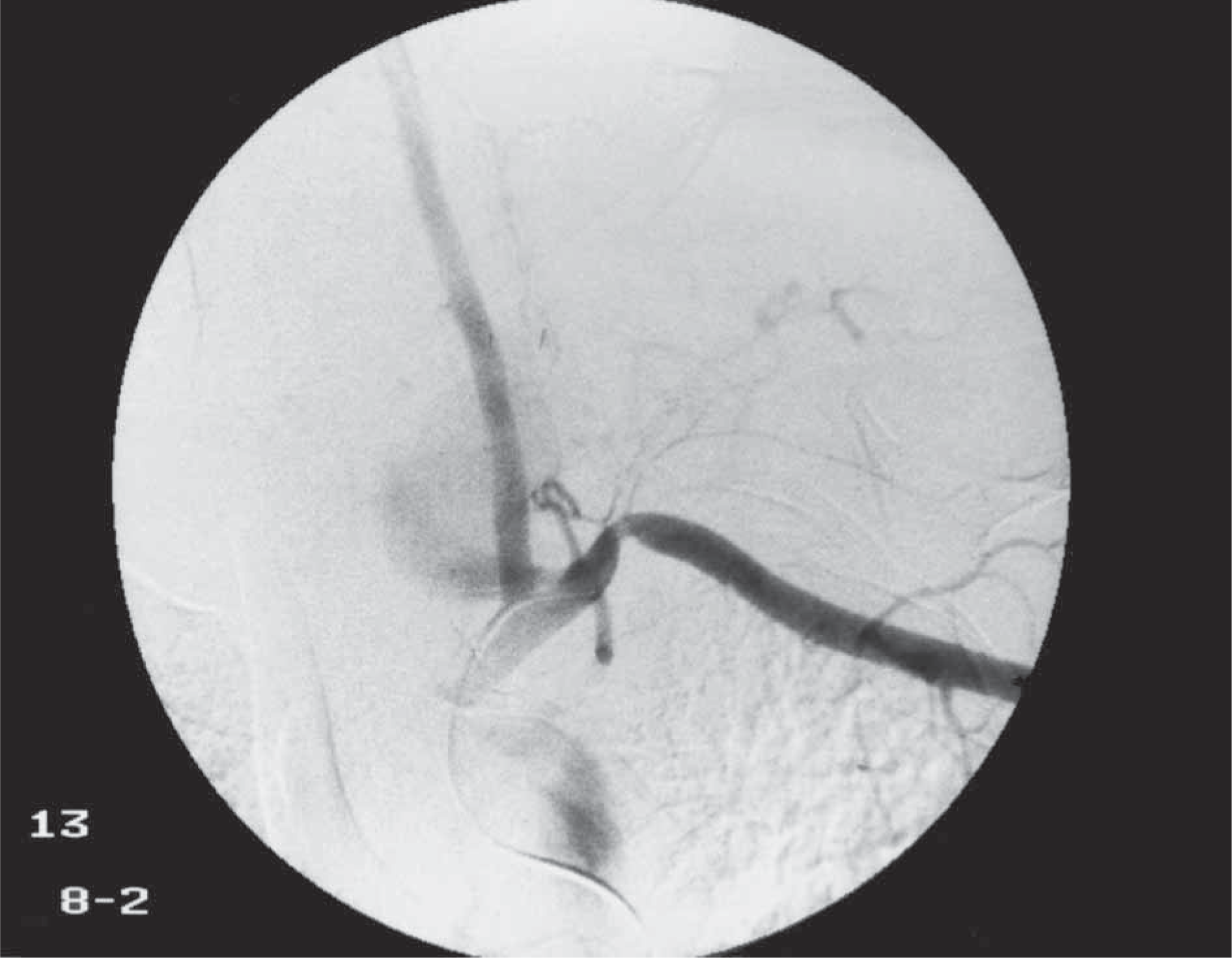
Angiography of the left subclavian artery demonstrated leakage of the contrast media near the origin of thyrocervical trunk.
The patient proceeded to surgery and a median sternotomy with a left supraclavicular extension was performed. Three hundred milliliters of blood were removed from the left pleural cavity. Bleeding at the subclavian artery was controlled proximally at the origin of the artery and the distal control was obtained at the third part of the left subclavian artery after resecting the clavicular shaft. The vertebral artery, thyrocervical trunk, left internal mammary arteries and the thoracic duct were individually ligated. Oxygen saturation measured at the left index finger was 99% and the estimated blood loss was 2,400 ml.
After the operation, the motor power of the left forearm was grade II/V which gradually improved to grade III/V. The sensory deficit remained unchanged. The patient was subsequently placed on a rehabilitation programme.
Case II
A 44-year-old man with neurofibromatosis, presented with an acute painful expanding mass experienced at the left supraclavicular region for 1 day. There was no history of trauma. A physical examination revealed a supraclavicular mass, 10 × 10 cm in diameter. Motor power in the left hand and forearm was grade IV/V with sensory deficit. A CT scan revealed a vascular mass at the left clavicular region and a left pleural effusion.
The patient suddenly developed hypotension and became unconscious. After resuscitation, an emergency operation was performed by a median sternotomy and a left supraclavicular extension. Cardiopulmonary bypass was commenced via the right atrium and the ascending aorta. The midshaft of the left clavicle was removed and there was more than 2,000 ml of clotted and nonclotted blood in the left pleural space. As the bleeding originated from the ruptured left subclavian artery, it was divided and ligated.
After the operation, the motor power and sensation of the left hand and forearm improved. The arterial section, when stained with hematoxylin and eosin, revealed a cellular proliferation of neurofibromatous tissue surrounding the adventitia of a normal small artery with infiltration into the hemorrhagic fibrofatty tissue (Figure 3). Some enlarged nerve bundles were also noted.
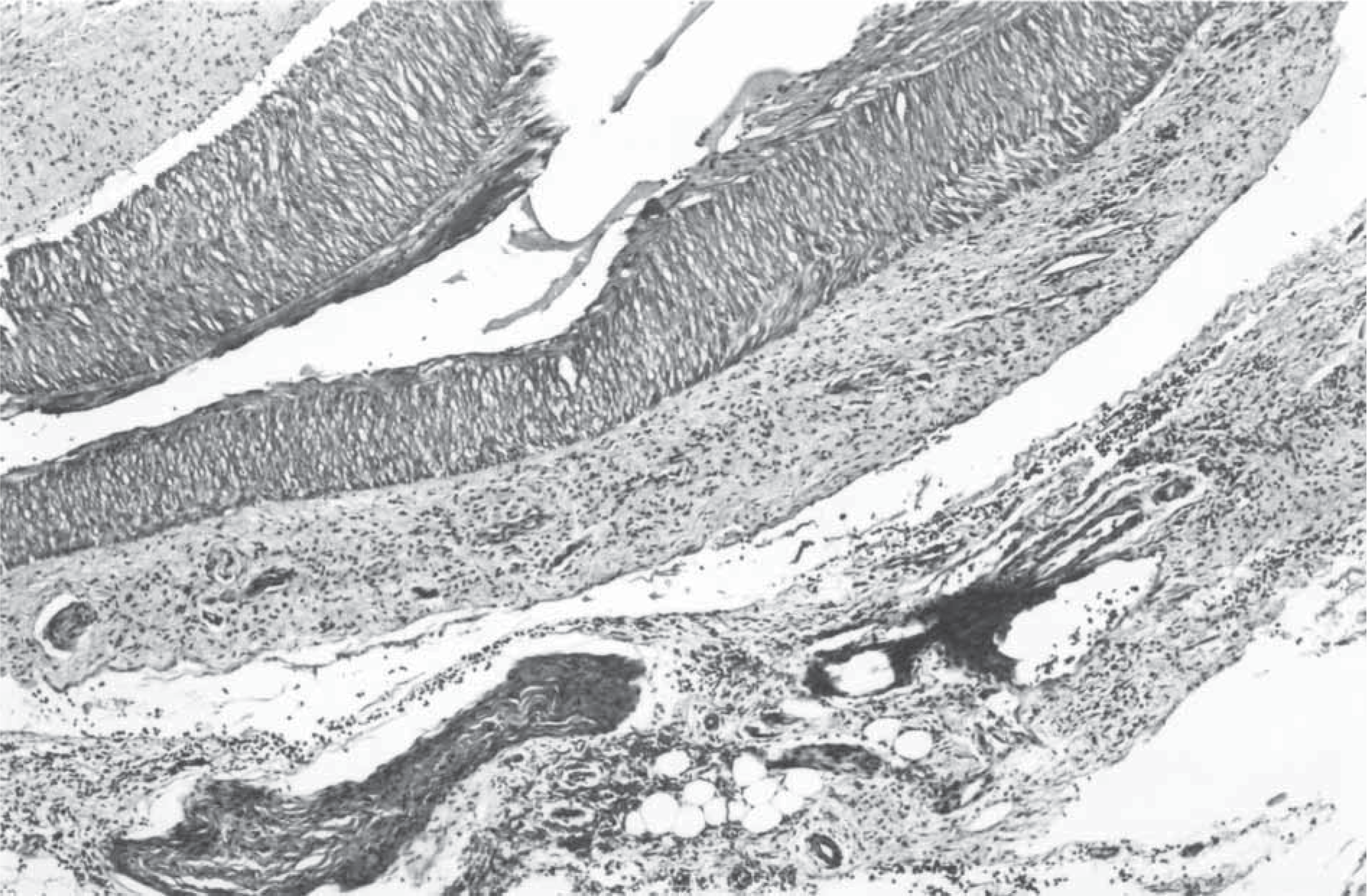
Photomicrograph of the arterial section revealed diffuse neurofibromatous tissue involvement around the small arteries and in the fibrofatty tissue (hematoxylin and eosin stain, original magnification × 40).
Discussion
Neurofibromatosis type I, von Recklinghausen, or peripheral neurofibromatosis is the most common form of neurofibromatosis with a prevalence of 1 in 4,500. The major defining features of the disease include Café au lait spots, freckling, peripheral neurofibromas and Lisch nodules. Minor disease features include macrocephaly, short stature, plexiform neurofibromas, CNS tumors, and intellectual handicap. 1 Vascular abnormalities such as stenoses, occlusions, aneurysms, arteriovenous malformations and fistulae are well recognized but uncommon. The most common abnormality is arterial stenosis, particularly at the proximal renal artery. While aneurysms are less common, there are reports of these in the left thyrocervical trunk, vertebral artery, left subclavian artery, lumbar artery, radial artery, coronary artery, and arc of Buhler. 2 –8
The pathology of vascular lesions was first described by Reubi in 1944, who divided them into three types: an intimal form (intimal proliferation occluding the vascular lumen), an aneurysmal form (fibrohyaline thickening of the intima with fragmentation of the muscularis and elastica), and a nodular form (spindle or epithelioid cells disturbing the integrity of the vessels wall). Salyer and Salyer proposed that the pathogenesis of all arterial lesions involves the proliferation of Schwann cells with secondary degenerative changes. 9 Greene et al described two basic categories of vascular lesions; one involving larger vessels with surrounding neurofibromatous or ganglioneuromatous tissue, and the other involving dysplasia of small vessel. 10 A ruptured left subclavian artery in the neurofibromatosis is uncommon and often fatal.
This is a report of two cases with a successful life saving operation involving the ligation of the artery was performed to control bleeding. There was a neurological complication in one patient. Vascular complications in the neurofibromatosis patient should be recognized, especially in the presence of a rapidly enlarging mass. In these situations, prompt investigations and subsequent operations should be undertaken.