
Abstract
We performed 167 femoropopliteal bypass surgeries in 151 patients (95 patients underwent above-knee bypass and 56 below-knee bypass) from December 1985 to December 2000 with the use of prosthetic graft or autologous vein graft. We compared primary patency rates between age, sex, graft material, distal anastomotic site and severity of ischemia, considering their survival rates to elucidate the long-term outcome of above-knee and below-knee femoropopliteal bypass. The 10 year patency rate for above-knee bypass was 47.4%, compared to 36.9% for below-knee (p < 0.01). Better results were found after bypass surgery for claudicants than for critical ischemia (p < 0.05). With regard to graft material and age categories, there were unexpectedly no statistical differences in either above-knee or below-knee anastomosis. The survival rate at 10 years in claudicants was 51.2%, compared to 15.9% with critical ischemia (p < 0.01). Mortality was much influenced by ischemic heart disease (p < 0.002) and the age of patient (p < 0.05). The results after above-knee bypass had comparable patency, whereas the results after below-knee bypass were disappointing. Below-knee arterial reconstruction for claudicants should be carefully considered and might be recommended only to patients with critical ischemia.
Introduction
Both operative indications and procedures to treat intermittent claudication caused by arteriosclerosis obliterans have been controversial. There are many options, however the criteria for conservative therapy, endovascular treatment, or surgical treatment have not yet been established. Some reports recommend conservative therapy 1,2 whilst others recommend surgical treatment. 3 –6 Even in the case of bypass surgery, the best choice of conduit for above-knee (AK) femoropopliteal (FP) bypass has not been established yet. This is due to some authors reporting results with the use of prosthetic graft being equivalent to the use of autologous vein graft, 7 –10 and because others advocated the use of autologous vein both for above and below knee (BK) arterial reconstruction. 11,12 Otherwise, for infrageniculate arterial bypass, the opinion that autologous vein is the best conduit is widely accepted. 13,14 However, patients with arteriosclerosis obliterans (ASO) can suffer from potential ischemic heart disease (IHD) concomitantly and they need to undergo some interventional coronary angioplasty and/or coronary bypass surgery. Their autologous saphenous vein might be implanted at cardiac surgery prior to lower limb surgery. In such cases we should consider an alternative conduit for below knee revascularization without appropriate autologous saphenous vein. Basically, we use prosthetic grafts for above knee bypass and use either saphenous veins or prosthetic grafts (Dacron or PTFE) for below knee bypass.
The purpose of this study was to review the results of primary above or below knee bypass surgery considering severity of ischemia, concomitant diseases and patient survival rates.
Patients and Methods
One hundred and sixty seven FP bypass surgeries performed on 151 patients from December 1985 to December 2000 at our institution were reviewed. AK bypass was reconstructed in 107 (64.1%) limbs and BK in 60 (35.9%) limbs. These patients were characterized by sex, age, risk factors, implanted graft materials and manifestation of lower limb ischemia. Severity of limb ischemia was divided into two categories: intermittent claudication and critical ischemia. Critical ischemia was defined as rest pain or gangrene. Furthermore, two age groups were defined, 70 years and older, the other less than 70 years, at time of surgery. Graft materials implanted were Dacron, PTFE and autogenous saphenous vein. In terms of bypass counduit numbers, Dacron graft was implanted in 142 (85.0%) limbs, PTFE graft in 7 (4.0%)limbs, and saphenous vein in 18 (11.0%) limbs (13 reversed vein, 5 “in situ”). Pre and postoperative ankle brachial pressure index (ABPI) was measured and arteriography was performed regularly. Ischemic heart disease was usually considered and routine cardiac ultrasound sonography and cardiac scintigraphy have been performed since the 1990's. Coronary angiography was considered necessary based on scintigram results. Postoperative antiplatelet drugs or coumarin potassium were given daily to all patients after bypass surgery.
Postoperative graft surveillance was studied at our outpatient clinic with ABPI and duplex scanning. Graft occlusion was diagnosed on the basis of ABPI decrease, duplex scanning findings or patient's symptoms.
Operative mortality and postoperative complications were considered when they occurred within 30 days of the operation. Primary patency was defined as uninterrupted patency of the graft without any intervention. Occluded grafts, which were not revasculized but replaced with new grafts, were considered as occluded. With regard to amputation, limited toe amputation was not considered a failure, however, at the ankle or above was considered limb loss.
The data was analyzed statistically using chi-square test and Student's t test for group comparison. Kaplan-Meier survival analysis was applied to calculate the cumulative graft patency and survival rates with long-rank test.
Results
The mean and median follow-up periods were 51.3 months and 47 months, respectively (range, 1 to 159 months). Twenty two patients were lost during the follow-up period. The mean ± SD age at operation of all the patients was 68.5 ± 7.78 years (range, 46 to 87). Additionally, the mean age of patients who underwent AK and BK femoropopliteal bypass surgeries was 68.9 and 67.6, respectively, and the mean age of the patients who had intermittent claudication and critical ischemia was 68.5 and 68.5, respectively. There were no statistical differences in terms of age. There were 135 (89.5%) men, and 16 (10.5%) women in the study. Of the 151 patients, 59 (35.3%) had diabetes mellitus (DM), 56 (33.5%) patients had ischemic heart disease (IHD), 106 (63.5%) had hypertension (HT) and 121 (72.5%) were smokers. The number of patients who had risk factors are summarized in Table 1. The number of patients who underwent AK bypass surgery was significantly more than those who underwent BK bypass surgery among DM patients (p < 0.05).
Patient Characteristics
DM = diabetes mellitus; IHD = ischemic heart disease; HT = hypertension.
There was a total of 61 graft occlusion cases during follow-up, of which 28 cases were AK bypass, and 33 BK bypass. Early graft failure, which occurred within 30 days of operation, counted 8 cases in the AK group and 3 in the BK group. In the AK group, 7 of 8 cases were implanted with a Dacron graft, and 1 case with a vein graft. In the BK group, 1 of the 3 cases was Dacron graft and 2 vein graft. Four early graft occlusion cases in the AK group were conservatively observed and 2 underwent immediate thrombectomy, with the other 2 undergoing late bypass operation. In BK cases, revisional bypass surgery was done for 1 case and conservative therapy for 2 cases. Only 1 case required subsequent amputation in BK cases despite early alternative revisional surgery because of progression of an infected foot ulcer. All these cases suffered from severe diabetes mellitus.
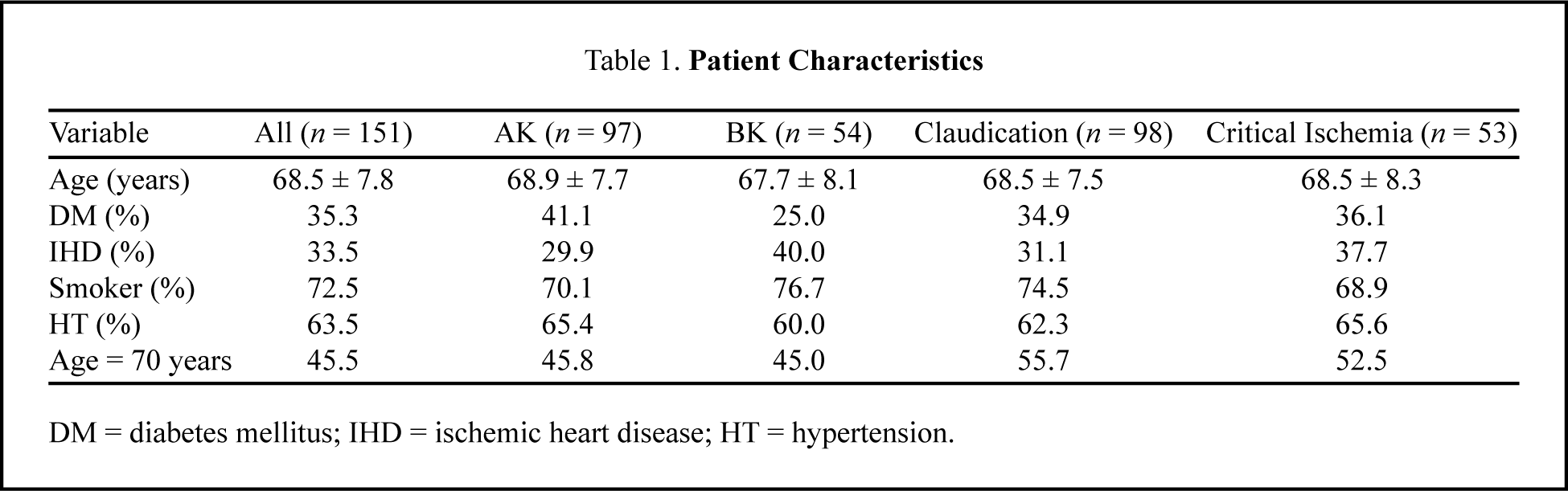
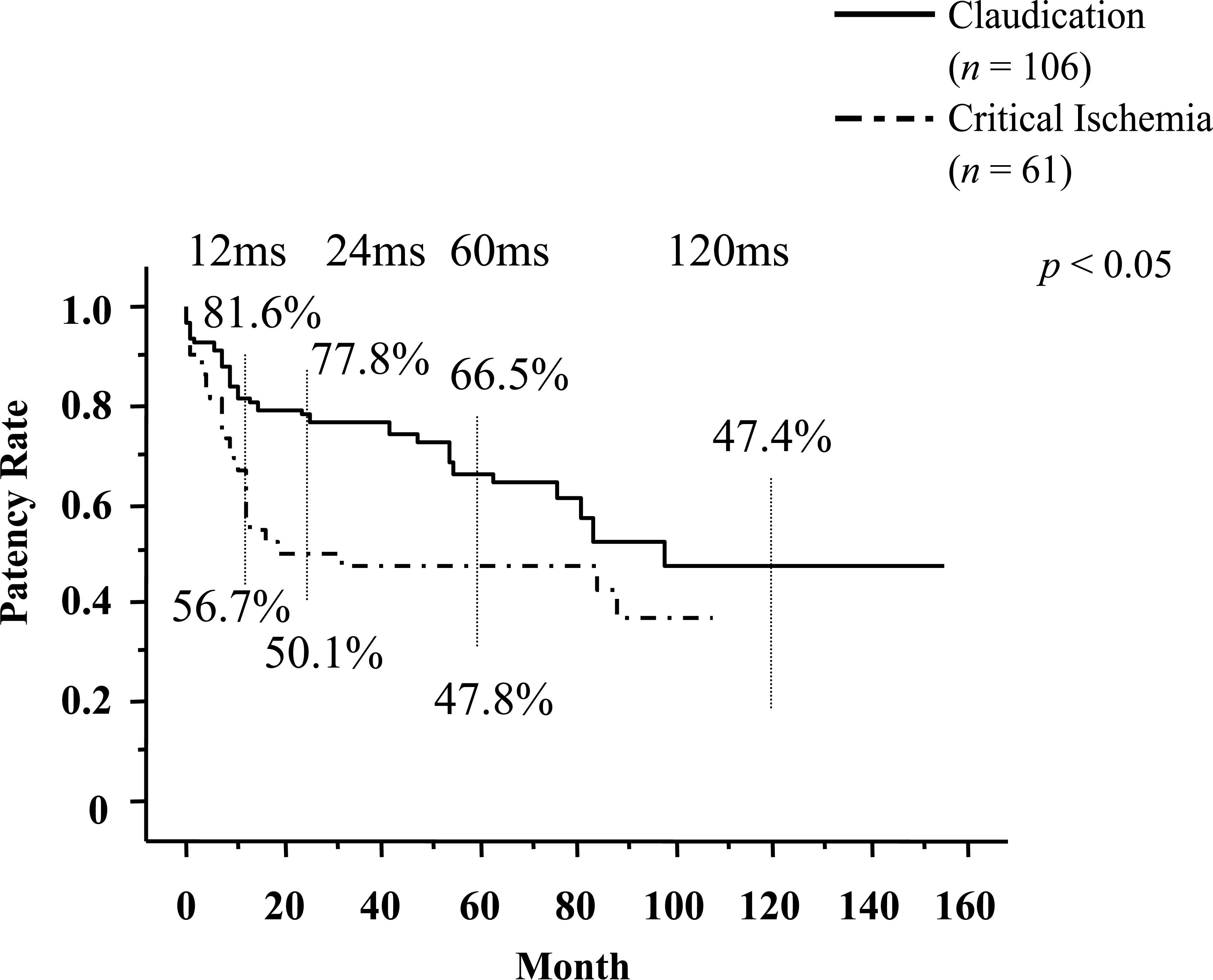
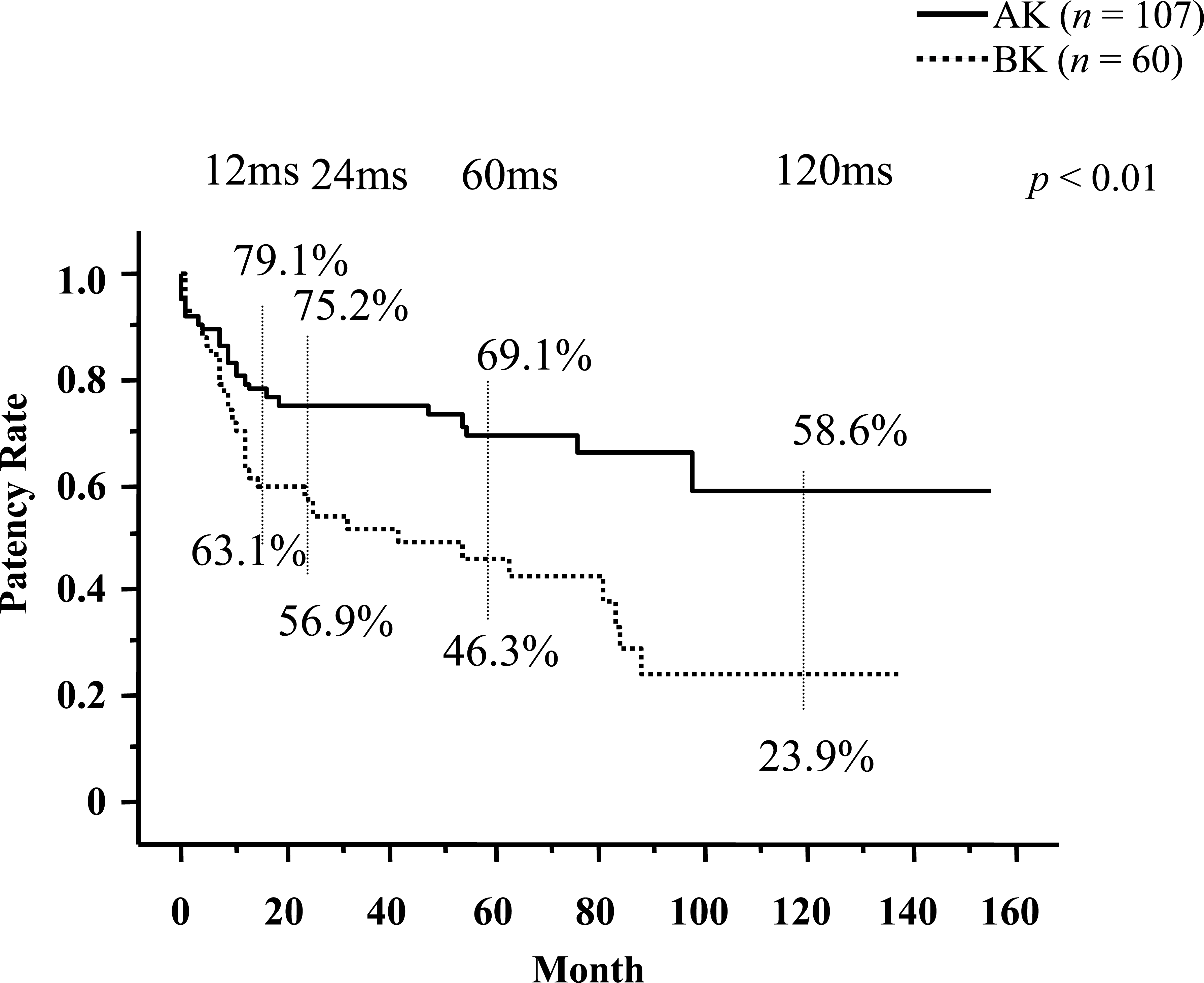
The patency rates at 1, 5 and 10 years in claudicants were 81.6%, 66.5% and 47.4%, respectively. This compares with 56.7% and 47.8% and 36.9%, respectively, in critical ischemia cases (Figure 1). The rates at 1, 5 and 10 years in AK were 79.1%, 69.1% and 58.6%, compared to 63.1%, 46.3% and 23.9%, respectively, in BK (Figure 2). Comparison of the patency rates between claudicants and critical ischemic patients, and also between AK and BK bypass, were statistically significant (p < 0.05, p < 0.01, respectively). As for graft materials, the patency rates at 1, 5 and 10 years using prosthetic graft for AK were 81.3%, 69.3% and 57.6%, respectively. The rates for BK were 73.7%, 50.6% and 26.1%, respectively. For vein graft, the patency rates at 1, 5 and 10 years for AK were 83.3%, 66.7% and 66.7%, respectively, and 67.5%, 56.3% and 56.3%, respectively, for BK (Table 2). There was no significant difference between the prosthetic graft and vein graft. There were a total of four operative deaths; three underwent AK bypass and one BK bypass. Three of these patients had life-threatening leg ischemia and were already in poor condition on admission. One patient had claudication and cause of death was uncertain. The survival rates at 1, 5 and 10 years in claudicants were 91.1%, 77.2% and 51.2%, respectively, compared to 79.2%, 53.9% and 15.9%, respectively, in patients with critical ischemia (Figure 3). The rates at 1, 5 and 10 years, characterized by distal anastomotic site, were 87.1%, 60.0% and 39.0%, respectively, in AK and 86.3%, 59.5% and 35.9%, respectively, in BK (Figure 4). Obviously, patients under 70 survived longer than patients 70 years old and over (Figure 5). Statistically significant differences were detected both in severity of ischemia and age categories (p < 0.01, p < 0.05, respectively), however, no difference was detected in the survival rates between those who underwent AK and BK anastomosis. Furthermore, only IHD affected mortality of the patients among these risk factors (Figure 6) (p < 0.002).
Cumulative primary patency for both claudication and critical ischemia groups, calculated by Kaplan-Meier method. Significant difference was recognized.
Cumulative primary patency for both AK and BK groups. There was significant difference between these groups.
Cumulative survival rate for both claudication and critical ischemia groups, calculated by Kaplan-Meier method. Significant difference was recognized.
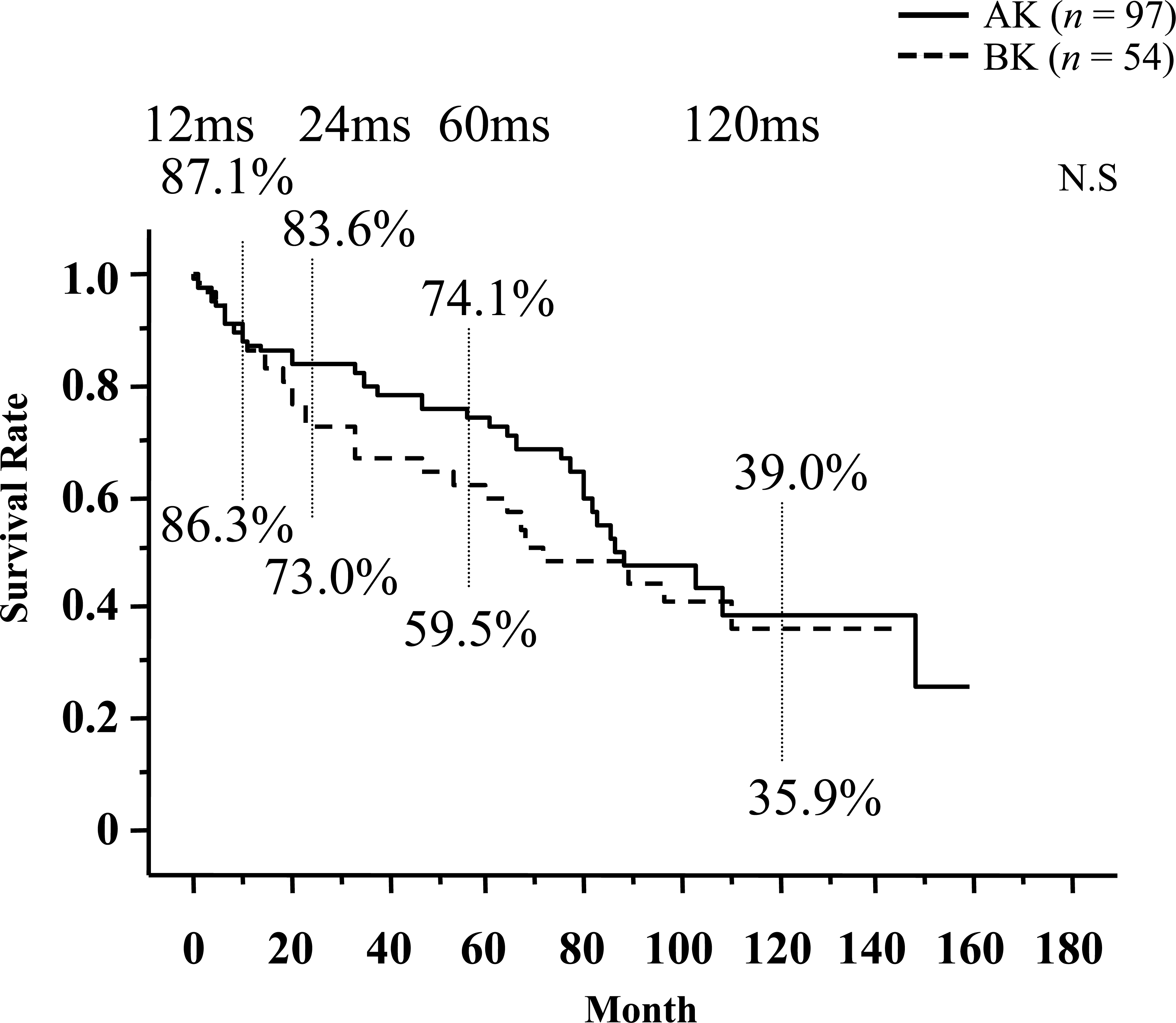
Cumulative survival rate for both AK and BK groups. There was significant difference between these groups.
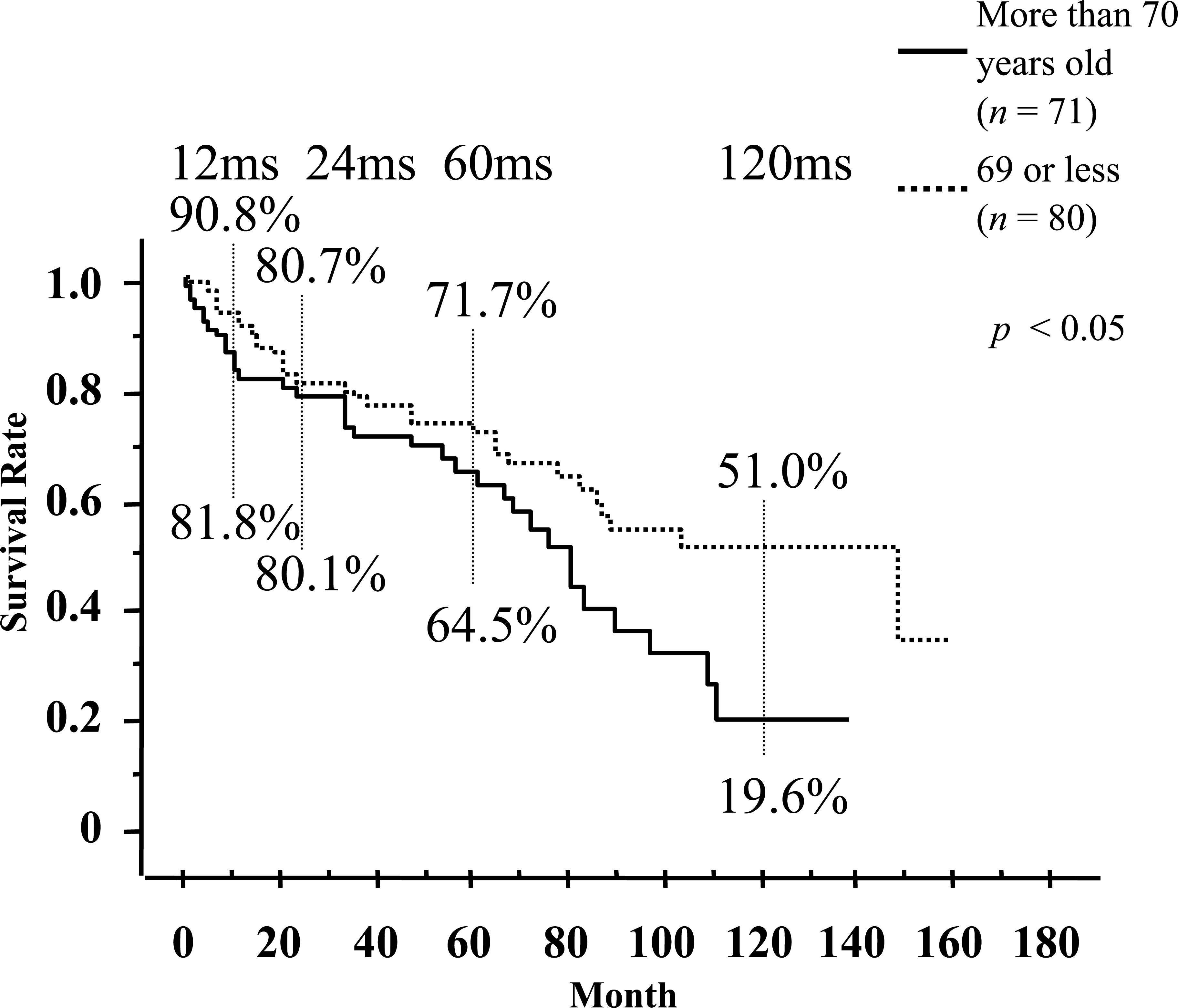
Cumulative survival rate for age category groups, calculated by Kaplan-Meier method. Significant difference was recognized between older than 70 years and 69 or less group.

Cumulative survival rate for the patients with IHD and without IHD. Significant difference was recognized between these groups.
Graft Materials Implanted at Bypass Surgery
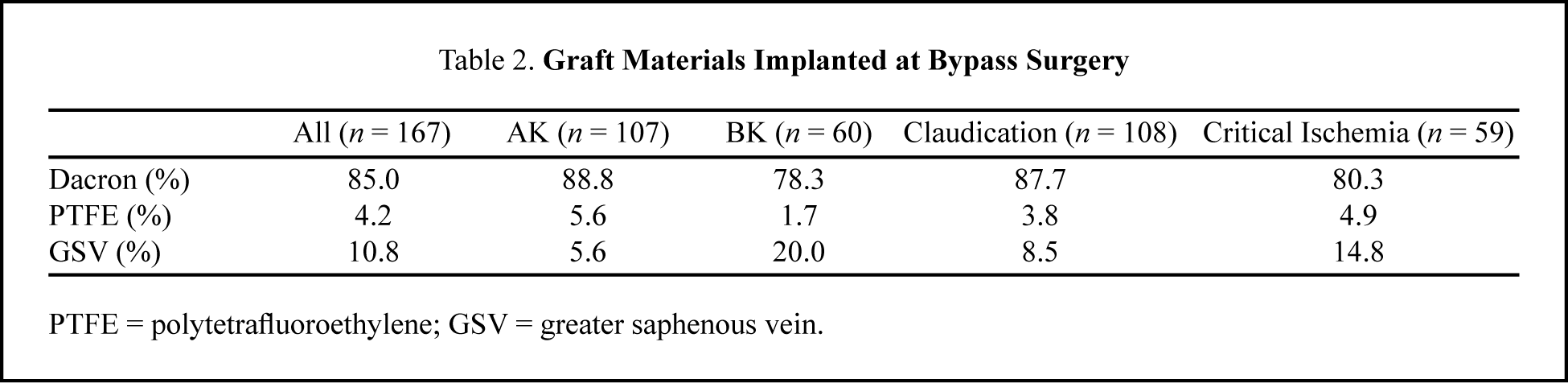
PTFE = polytetrafluoroethylene; GSV = greater saphenous vein.
Discussion
The indications for femoropopliteal bypass in patients with intermittent claudication are controversial and universal acceptance has not been established. In the western world, especially in the US, conservative therapy may be the first choice and reconstructive surgery is not recommended 2,15 because claudication does not mean critical ischemia resulting in limb loss. Unless symptoms improve with appropriate medication and/or exercise, patients find limitations in their activities. Daily life could be much improved after successful bypass surgery. However, our study reveals that most patients with lower limb peripheral arterial disease simultaneously had other vascular diseases, such as coronary artery disease and cerebral vascular disease. Therefore, bypass surgery for intermittent claudication is not recommended without appropriate estimation of the patient's general condition. From this point of view, the present data is reasonable in that only one operative death (uncertain reason) after reconstructive surgery for intermittent claudication and only 3 death cases for severe critical ischemia occurred. IHD is the most common cause of fatal event among patients with peripheral arteriosclerosis, 16 and our report also reveals IHD to be one of the most significant risk factors which greatly influences the mortality rate with femoropopliteal occlusive disease. The reason for only one operative death after surgery for claudicants to date, we think, was that cardiac condition was estimated routinely by means of ultrasonography and/or scintigraphy. If necessary, interventional radiology or coronary bypass surgery was performed prior to bypass surgery. 17 Fifteen patients underwent cardiac revascularization prior to FP bypass surgery. DM is a well recognized risk factor for death and for graft failure. 16,18 It was surprising that DM influenced neither the mortality nor the graft patency of the patients who underwent FP bypass surgery, despite all patients who needed revisional BK bypass being diagnosed as having diabetes mellitus with poor run-off. It was probable that the combination of DM and poor run-off might progress peripheral arteriosclerosis and graft failure.
What is the best conduit for AK or BK bypass surgery? According to our study, no statistical differences in patency rates were recognized among graft materials in either AK or BK bypass surgery. These results were surprising as it was thought that greater saphenous vein (GSV) graft must be the preferred material to other prosthetic grafts for BK revascularization. Dacron graft was not worse than the GSV conduit, unexpectedly. Our better patency rates, especially with regard to BK bypass, were thought to be due to the lack of kinking and compressibility of the Dacron graft, the avoidance of clamps with the use of tourniquet, and to the policy of making a wide distal anastomotic site first (more than 2 cm). 19,20 Despite obtaining this preferential result, currently we choose prosthetic graft for above 2nd portion of popliteal artery and choose autogenous GSV for distal BK system at first. One reason is that, even if coronary bypass grafting is mandatory prior to the FP bypass surgery, we do use not GSV graft, but arterial graft, e.g. radial artery, internal thoracic artery, for coronary revascularization in recent times. Another reason is that distal bypass in the future could be difficult after GSV has already used for AK bypass surgery.
In conclusion, AK bypass surgery should be offered only to the patients with disabling claudication and critical ischemia who have their quality of life much limited, though AK bypass surgery could be advocated as a safe and durable operation based on our study. However, BK bypass should be carefully considered for the claudicant and might be recommended for limb salvage procedures.