
Abstract
Multifocal sclerosing hemangioma of the lung is a rare entity. While solitary pulmonary lesions by themselves are uncommon and few reports have been described, multifocal bilateral lesions are rare and limited instances have been cited in indexed medical literature. We herewith describe a case of multiple sclerosing hemangiomas of the lung, in a patient who also had a vascular malformation over the calf.
Introduction
Liebow and Hubbell first described the lesion sclerosing hemangioma of the lung in 1956. 1 The lesion has unusual histological features and presents a diagnostic challenge to the pathologist. Considerable controversy surrounds the exact nature of the tumor and its classification as to whether it represents a hamartoma or a neoplastic process. While numerous reports in the literature have reported series of these unusual lesions, the finding of multiple bilateral lesions is rare and merits reporting. We report one such case seen recently at our center.
A 17-year-old male was referred to us from another hospital for multiple coin shadows in the lung. He had a history of a swelling over the calf excised about six months ago. The pathology report from the referring hospital confirmed the excised lesion to be a sarcoma with a prominent vascularity. A routine chest X-Ray performed on the first follow-up six months later showed multiple nodular shadows in the right lung. With a presumptive diagnosis of sarcoma, clinicoradiologically he was diagnosed to have multiple pulmonary metastases and was referred to our hospital for further management. A review of the pathology slides of the original lesion revealed a vascular malformation. Since it was not sure whether all the slides had been submitted and evaluated, we presumed this patient to have a malignancy. We therefore treated the condition as pulmonary metastasis from a sarcoma. The patient was asymptomatic and no clinical abnormality was noted on general physical examination. The local site of the excision was normal on clinical examination. Computed tomography (CT) scan performed by us confirmed the presence of multiple lesions in the lung (Figure 1). In view of the young age, good general condition, and excellent pulmonary functions, a metastatectomy was planned. The patient underwent a standard right posterolateral thoracotomy. On exploration multiple nodules were detected in the right lung with at least 10 of them distinctly palpable. Three nodules were detected in the upper lobe, two in the middle lobe and five in the lower lobe. The lesions were nodular, firm on palpation, between 1–2 centimeters in size and diffusely spread over the pulmonary parenchyma.
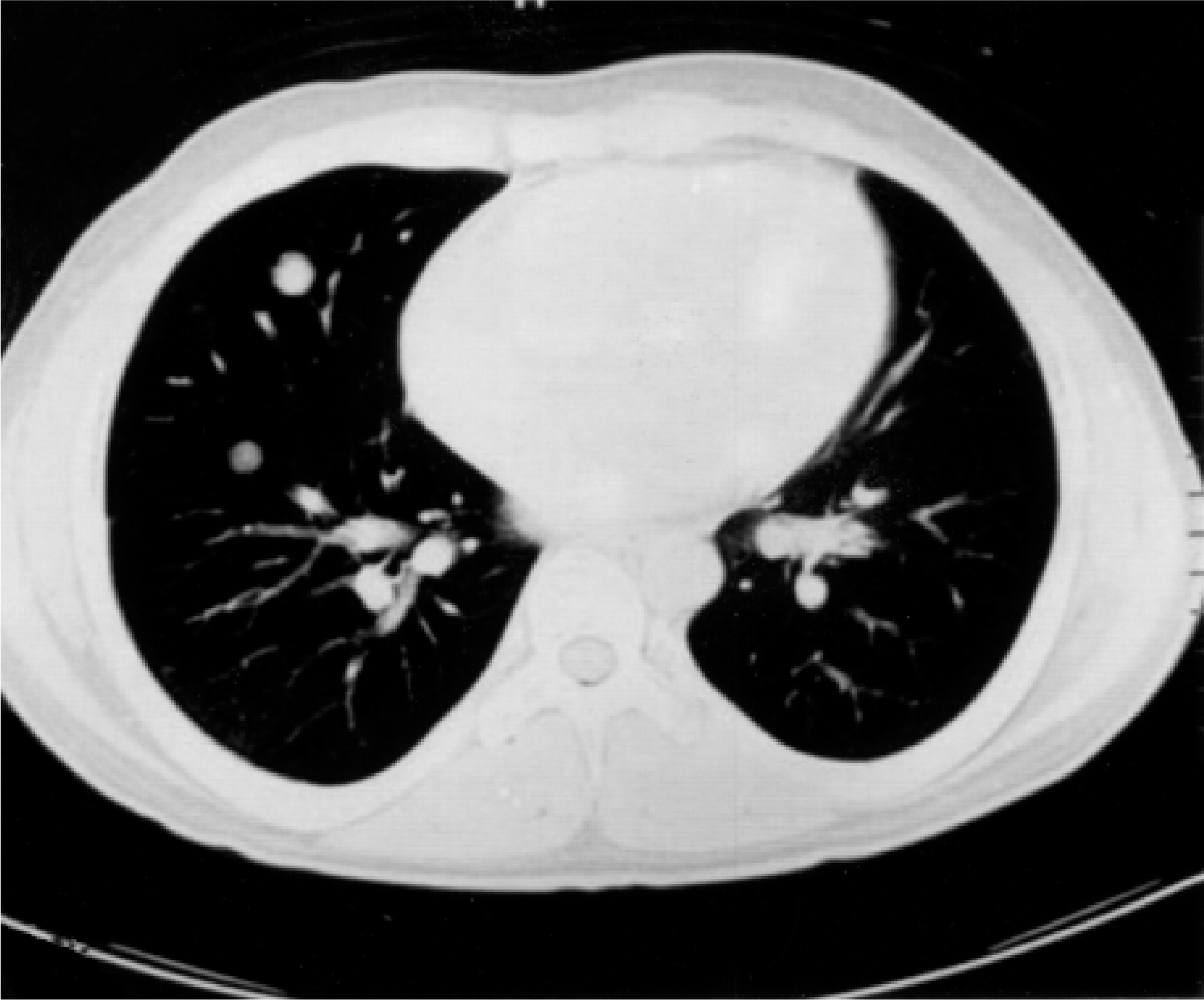
CT scan showing nodules bilaterally.
A wedge resection of the lesions in the lower lobe was done (Figure 2) and a frozen section for the same was carried out. Frozen section showed the lesion to be a sclerosing hemangioma and in view of multiple lesions present, involving all the three lobes and diffusely spread, further wedge resection of these lesions was abandoned. Removal of all the lesions would have amounted to a significant loss of functioning lung parenchyma. The patient had a smooth postoperative recovery and was discharged four days later.
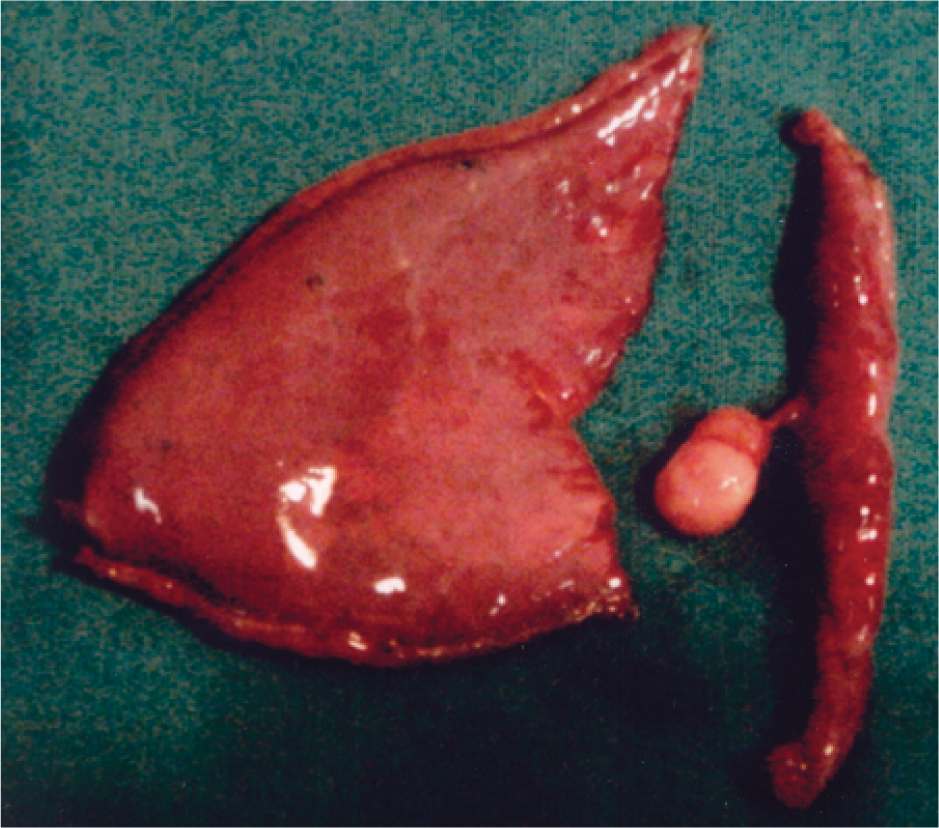
Clinical photograph of a resected hemangioma.
We therefore concluded that malignancy was not present. The finding in this case of multiple sclerosing hemangiomas was purely incidental and accidental. This may probably be the first recorded instance of these lesions co-existing with a vascular malformation elsewhere in the body.
Discussion
Sclerosing hemangioma of the lung is an unusual benign tumor first described by Liebow and Hubbell in 1956. 2 They described 7 lung tumors, which they named sclerosing hemangiomas, lesions which are very often confused with pulmonary histiocytomas. 3 Liebow suggested this term because of the numerous lakes and hemorrhagic areas that characterize this lesion. Various alternative terms have been suggested including post inflammatory pseudotumor, fibroxanthoma, papillary pneumocytoma, and histiocytoma. 4 Clinically, sclerosing hemangiomas of the lung have a propensity to present as an asymptomatic solitary lung nodule in young female patients (80%) more often than not as incidental findings on chest X-Ray. 4 These lesions are commonly detected at between 15 and 83 years of age with most occurring in the 5th decade of life. For reasons not very clear a high proportion of the cases have been seen in the Orient. Symptoms if at all present are cough, chest pain, recurrent cold and hemoptysis. 4 Macroscopically, sclerosing hemangiomas are benign tumors often evidenced as round to oval masses, which are well circumscribed with an average size of 2.8 centimeters and a range of 0.4–8.0 cm in diameter. The majority of the lesions are less than 5 cm: in our case most of these lesions were about 2 cm in diameter. The lesions are well surrounded by the pulmonary parenchyma but are not encapsulated. 2 The lesions from the pulmonary parenchyma can be easily shelled out and this helps differentiate them from well-differentiated adenocarcinomas, which also can be easily enucleated. 2,4
The lesions may on occasion involve the pleura. 2 The lesions have a yellow, red tan or gray appearance on cut section and a varying amount of fatty change. Fresh or old hemorrhage may also be present. Some tumors may have a rubbery or a granular cut surface. The surrounding lung tissue at times may show discoloration but may otherwise be normal. 4 Sclerosing hemangiomas are well defined and circumscribed lesions within the pulmonary parenchyma composed of round cells with bland nuclei and intermixed with papillary and tubular structures lined with cuboidal epithelium. 5
The tumor differentiated to type 2 pneumocytes in various areas. 6 Differential diagnoses of similar lesions in the lung have been suggested and includes a variety of benign and malignant lesions such as: inflammatory l pseudotumor, benign clear cell tumor, carcinoid, epitheloid hemangioendothelioma, histiocytoma, bronchioalveolar carcinoma, and metastatic tumors of the thyroid and kidney. 4
The papillary nature of sclerosing hemangiomas demands that it be distinguished from adenocarcinomas of the lung, particularly from well-differentiated adenocarcinomas. Adenocarcionoma cells show a greater cytologic atypia and frequent mitoses: a feature missing from sclerosing hemangiomas. Metastatic papillary lesions from the kidney and thyroid may occasionally pose a diagnostic difficulty. 4 The histogenesis of this lesion has been a subject of speculation and debate. The question of whether sclerosing hemangiomas are a neoplastic or hamartomatous process has still not been resolved. However the bulk of the available evidence suggests that pulmonary sclerosing hemangiomas are an epithelial neoplastic process, and have a potential for pneumocytic, Clara cell and bronchiolar differentiation. This finding is further supported by the fact that rare cases are multifocal and have occasionally been shown to be metastasizing. However Spencer and Nambu argued for a hamartomatous origin on the basis of a variety of epithelial and mesenchymal tissues that may be present in this lesion. 3 These lesions may also arise due to a congenital weakness of the blood vessels and in that case multiple vascular lesions and malformations should be the rule rather than the exception. 7 Approximately 150 cases of pulmonary sclerosing hemangiomas have been described individually or as a series of cases. 2 As in the present case, rare multiple lesions have been described and at times bilateral lesions have also been reported. 3,5,7,8 Some authors have reported multifocal lesions as in our case. Lesions with spread to the regional lymph nodes have also been periodically described. 3 They may be locally invasive and may infiltrate into surrounding structures in the mediastinum. 4 On thoracotomy, wedge resection of these lesions or a lobectomy has been the standard treatment. 2,4 No cases of recurrence have been cited. 2
The present case is an unusual finding in light of the general clinical pattern of presentation of pulmonary sclerosing hemangiomas. The likelihood of multiple sclerosing hemangiomas although unusual, should be borne in mind when evaluating any patient with multiple coin shadows in the lung. The diagnosis should be made after thorough clinical evaluation of the patient and after ruling out other obvious causes of such radiological findings.