
Abstract
To evaluate the invasiveness of a minimal access approach for simple congenital heart defects, and determine whether it can be regarded as a standard operation, 83 patients with an atrial septal defect and 73 with a ventricular septal defect underwent repair through a minimal skin incision and lower partial median sternotomy. There were no operative deaths, severe intraoperative complications, or conversion to full sternotomy. The clinical course of 106 patients was compared with that of 21 treated using a full sternotomy by the same surgeon; there were no significant differences, except in the operative time for ASD patients. The clinical courses of 2 minimal access subgroups (50 patients operated on by residents and 106 treated by the staff surgeon were compared; operative time, bypass time, ventricular fibrillation time (ASD repair), and cardiac arrest time (VSD repair) were significantly shorter in those operated on by the staff surgeon, but there was no difference in clinical course. The minimal access approach produced good cosmetic results, its invasiveness was similar to that of a full sternotomy, and it may be considered a standard operation for pediatric patients with septal defects.
Introduction
With recent advances in minimally invasive cardiac surgery (MICS), it has been introduced even for pediatric patients. 1 –10 Patients and their parents are coming to expect smaller incisions and the accelerated recovery that these operations seem to provide. Previously, pediatric surgeons had several ways of accessing the heart through smaller incisions, often relying on femoral artery cannulation to achieve cardiopulmonary bypass (CPB). 1,2 The complexity of such approaches precluded widespread adoption. In contrast, a limited skin incision and partial sternotomy represent a very simple method for repair of congenital heart defects. 4,5 Owing to the flexibility of children's tissues, the partially divided sternum is easily retracted, providing direct visualization, and special instruments are seldom required. However, it is unclear whether this approach is really less invasive than a full median sternotomy, or whether it is reasonable to regard it as a standard operative technique. 7 –9 To help clarify these points, we conducted a retrospective study on patients operated on by a partial lower sternotomy at our institution.
Patients and Methods
Between August 1997 and October 2001, 156 children under the age of 18 years underwent elective closure of an atrial septal defect (ASD; n = 83) or ventricular septal defect (VSD; n = 73) through a limited skin incision and partial lower sternotomy. There were 63 boys and 93 girls. They ranged in age from 3 months to 17 years (mean age, 50 ± 44 months); body weights ranged from 4.3 to 50.2 kg (mean, 15.1 ± 10.1 kg). The diagnosis was made by preoperative echocardiography (Table 1). The ASDs were repaired by direct closure in 81 cases and by patch closure in 2. All VSDs were repaired by patch closure.
Patient Characteristics
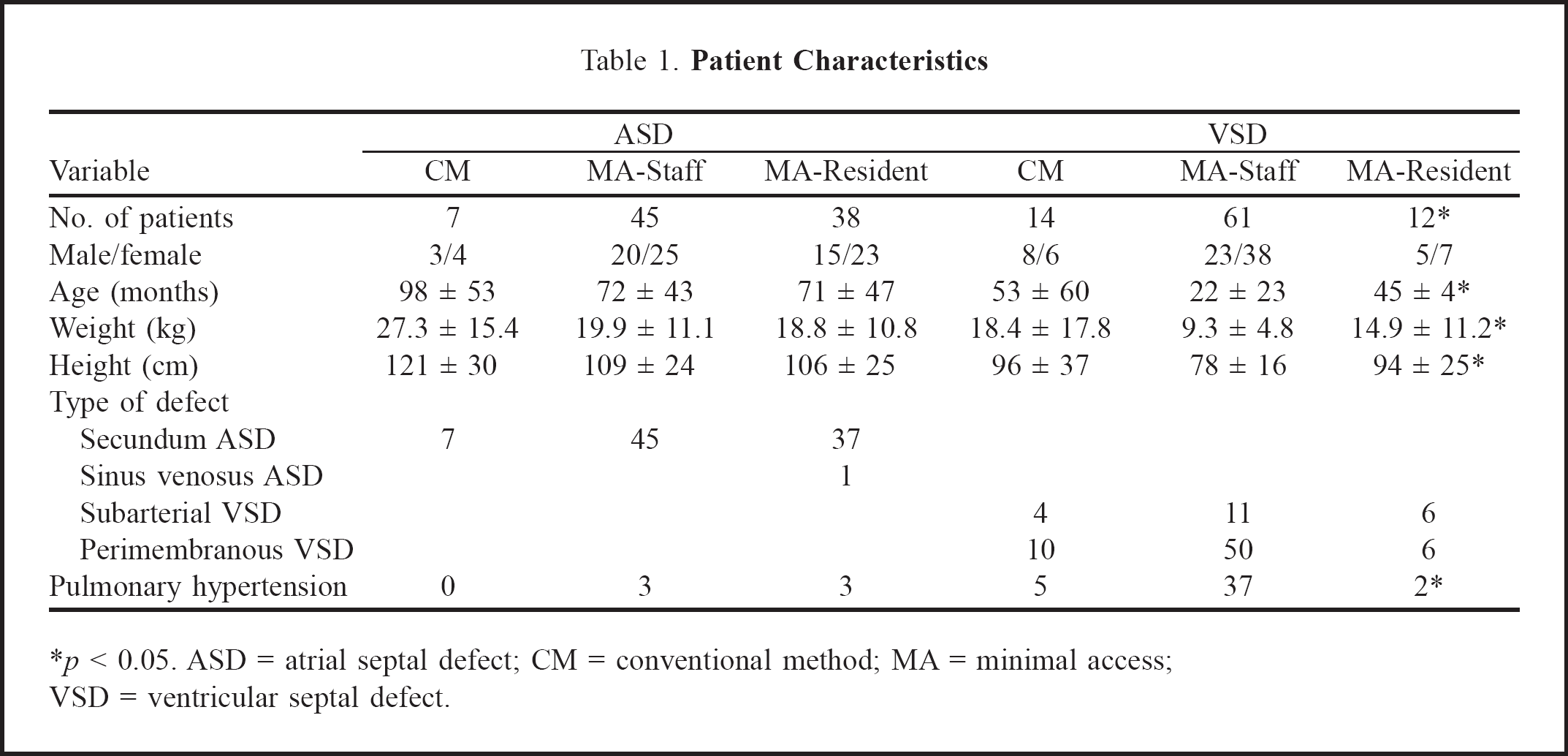
*p < 0.05. ASD = atrial septal defect; CM = conventional method; MA = minimal access; VSD = ventricular septal defect.
All patients were placed in the supine position, and a roll was used to elevate the inferior portion of the chest to improve exposure. The length of the skin incision was decided by the ratio of the incision (cm) to the patient's height (m), to obtain a ratio of 6.0. The superior extent of the skin incision was restricted to 1 cm above the nipple level. Skin flaps were raised to mobilize the incision. The sternum was partially divided up to the level of the manubrium. A standard pediatric sternal retractor was used to spread the partial sternotomy. No instruments were used for cephalad retraction. The thymus was partially resected, and the pericardium was opened. Cannulation pursestring sutures were placed on the ascending aorta, the atrial-inferior vena caval junction, and the superior vena cava or right atrial appendage. After heparinization, aortic cannulation was performed with the root of the ascending aorta carefully retracted. The inferior vena cava was drained with a straight venous cannula, and the superior vena cava was intubated directly with a right-angled cannula or with a straight cannula through the atrial appendage. After CPB was established, the venae cavae were snared in preparation for total CPB. The aorta was clamped through the incision with a standard crossclamp. Ventricular fibrillation was performed mechanically in ASD cases, and cardioplegia was administered through the aortic root in VSD cases. Moderate to mild hypothermia (28°C–32°C) was used for CPB. Direct or patch closure of an ASD was carried out through an atriotomy. Patch closure of a VSD was performed using continuous suture with a Dacron patch. Subarterial VSDs were repaired through incision of the pulmonary artery, and perimembranous VSD through an atriotomy. The crossclamp was removed after air was eliminated from the left heart, and removal of air was continued through the aortic root. The patient was rewarmed, CPB was terminated, and the pericardium was partially coapted. A mediastinal drain and a pericardial drain were inserted, and the sternotomy was closed with nonabsorbable sutures. Subcutaneous tissue was approximated, and the skin was closed using an intracutaneous running suture.
To evaluate the invasiveness of this method, intraoperative and postoperative clinical results were compared with those of a conventionally treated control group for the following variables: operative time, bypass time, ventricular fibrillation time or cardiac arrest time, and postoperative hospital stay, drainage, maximum white blood cell counts, and maximum C reactive protein levels. Forty-five ASD patients and 61 VSD patients who underwent total repair via a partial sternotomy performed by a single staff surgeon were selected as the minimal access (MA) group. The control group comprised 7 ASD and 14 VSD patients who underwent total repair via the conventional method (CM) of a full sternotomy by the same surgeon. To determine whether the minimal access method can reasonably be considered as a standard operation, the 156 MICS patients were divided into the staff surgeon group (45 ASD and 61 VSD) and the resident surgeon group (38 ASD and 12 VSD). The two groups were compared with regard to clinical course and the ratio of incision length (cm) to height (m).
All data are presented as mean ± standard deviation. Patient characteristics and postoperative clinical course were compared using the Student t test for continuous variables and the chi-squared or Fisher's exact test for categoric variables. A value of p less than 0.05 was considered statistically significant. Stat-View version 4.5 software (Abacus Concepts, Berkeley, CA, USA) was used for statistical analysis.
Results
There were no operative deaths in this series; no severe intraoperative complications with regard to exposure, cannulation, or bleeding; and no need to convert to conventional full sternotomy. A transient air embolism occurred in one VSD patient in the staff group; the patient had recovered completely by the time of discharge. The length of the skin incision varied between 3.9 and 12 cm, according to the size of the patient. The ratio of mean skin incision (cm) to mean height (m) was 6.3 ± 1.0, and the cosmetic results were superior in the minimal access patients (Figure 1).

The length and location of the skin incisions is shown in a 10-month-old infant 1 month after closure of a ventricular septal defect. The coin is a Japanese 1-yen coin which is 2 cm in diameter.
Patient characteristics of the CM and MA groups are shown in Table 1. There were no significant differences between ASD patients in the two groups. Among VSD patients, the age and weight of the MA patients were significantly lower. The number of patients with pulmonary hypertension was greater in the MA group. Table 1 also shows the patient characteristics in the staff and resident subgroups. For ASD patients, there were no significant differences between the groups. For VSD patients, the age, weight, and height of the patients in the resident group were significantly greater than those in the staff group. The number of patients with pulmonary hypertension was smaller in the resident group.
Table 2 compares the clinical course of patients in the CM and MA groups. Among ASD patients, operative time was significantly shorter for the MA group than the CM group, and it was also shorter for VSD patients in the MA group. Bypass time and ventricular fibrillation or cardiac arrest times did not vary significantly between groups. There were no significant differences in the postoperative clinical course for MA and CM patients, although postoperative hospital stay tended to be shorter in the MA group.
Comparison of The Conventional and Minimal Access Operations By a Staff Surgeon
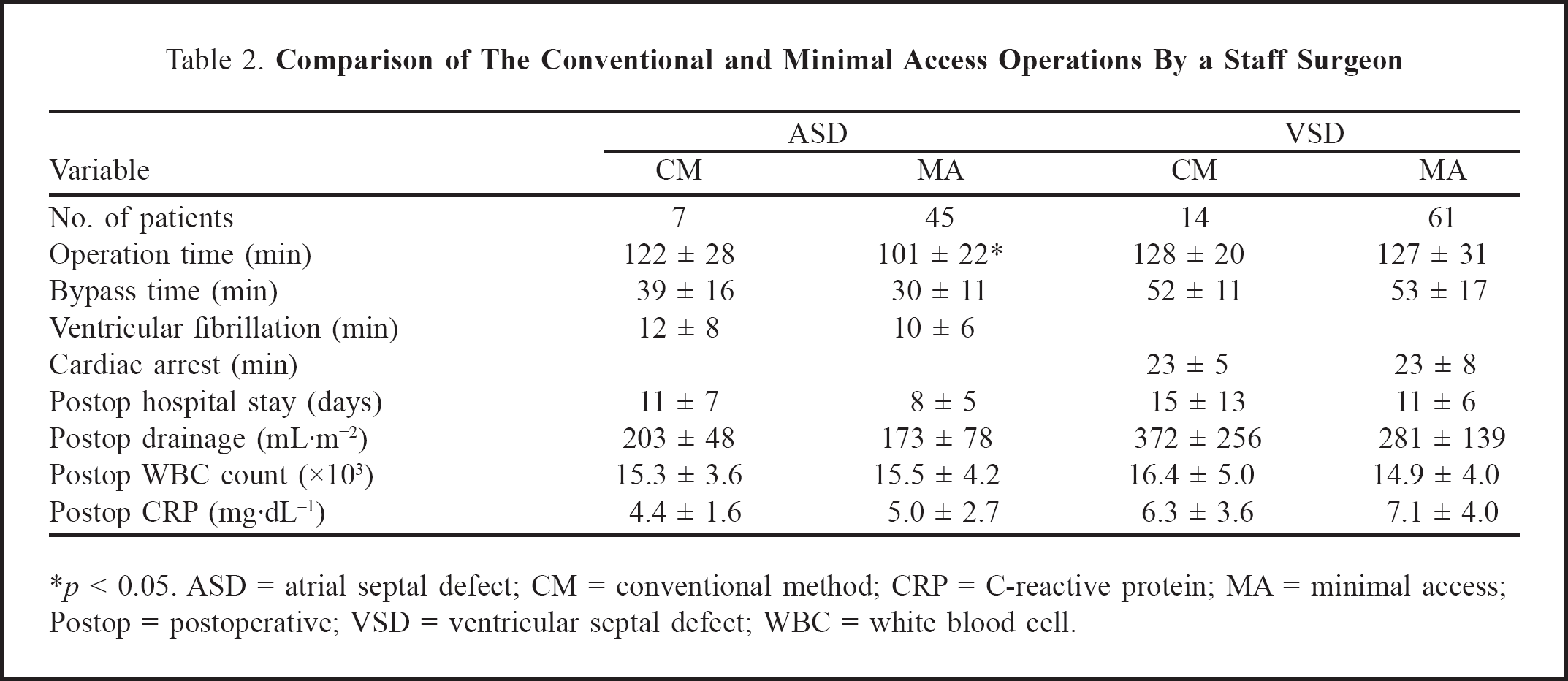
*p < 0.05. ASD = atrial septal defect; CM = conventional method; CRP = C-reactive protein; MA = minimal access; Postop = postoperative; VSD = ventricular septal defect; WBC = white blood cell.
The clinical course of patients in the staff group is compared with that of the resident group in Table 3. Mean operative time, bypass time, ventricular fibrillation time (ASD cases), and cardiac arrest time (VSD cases) for patients in the staff group were significantly shorter than for those in the resident group. There was no significant difference in other clinical course variables, except for postoperative C reactive protein in the ASD group and length of hospital stay in the VSD group. The ratio of incision (cm) to height (m) was nearly the same in both groups.
Comparison of Staff vs. Resident Surgeons
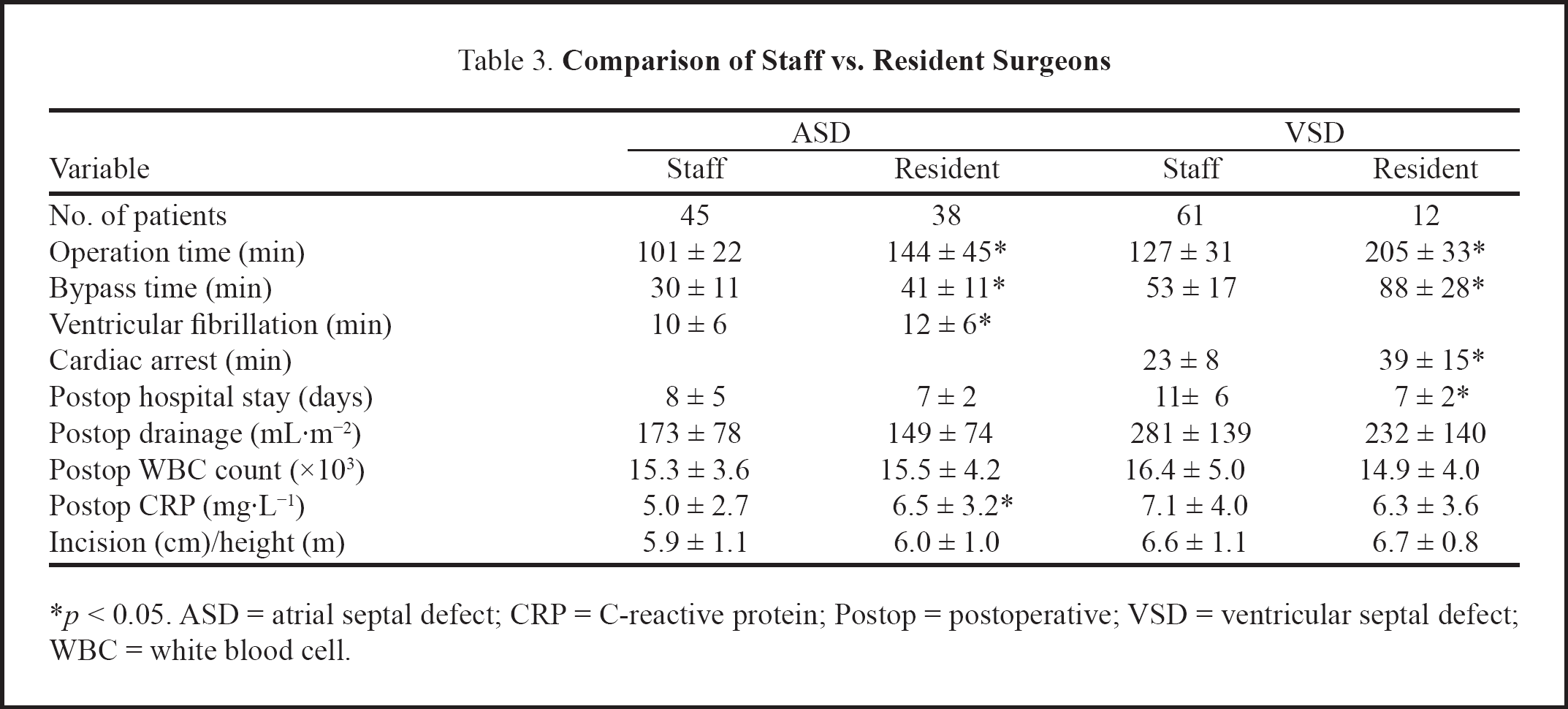
*p < 0.05. ASD = atrial septal defect; CRP = C-reactive protein; Postop = postoperative; VSD = ventricular septal defect; WBC = white blood cell.
Discussion
Early studies on different minimally invasive approaches for pediatric cardiac surgery showed that transatrial closure of ASDs and VSDs could be performed without sternotomy or with a limited sternotomy. 4 –10 For female patients, anterolateral thoracotomy with a submammary skin incision was adopted to produce cosmetic advantages over a median sternotomy. 2,11,12 However, phrenic nerve injury was noted following ASD closure through an anterior right thoracotomy, and pectoral muscle and breast maldevelopment was reported after a transverse inframammary incision, along with paresthesia around the breast tissue. 13,14 The parasternal approach with peripheral cannulation provides reproducible exposure of cardiac structures without violating chest wall integrity, and it reduces pain. 15 However, resultant chest wall deformity and lung herniation have prompted some centers to abandon this approach. 16,17 Although the addition of videoscopic assistance and percutaneous transthoracic aortic crossclamping permits adequate exposure through an even smaller thoracotomy, this approach has not been adopted widely because of the difficulty and complexity of relying on femoral cannulation to achieve CPB. 1,2 The difficulty of defibrillation and air removal from the ventricles is also a serious drawback.
On the other hand, there are several advantages with the lower partial sternotomy. 4 –10 The skin incision is much shorter than the conventional sternotomy, and sternal elevation and retraction provide adequate exposure of the heart and great vessels. The incision is easily and rapidly extended to a full sternotomy should technical problems be encountered or if exposure is inadequate. We chose the lower partial sternotomy rather than the transxyphoid approach which compromises exposure of the ascending aorta, impairs crossclamping, cardioplegia, and air removal, and often requires peripheral cannulation. As there were no operative deaths, no severe intraoperative complications regarding exposure, cannulation, or bleeding, and no need to convert to a full sternotomy, we concluded that this approach can be safely performed for all children and infants who need a transatrial reconstruction procedure.
The cosmetic result achieved with this approach is good, but some reports have expressed concern about the surgical results. 18 To evaluate the invasiveness of this method, the clinical results were compared with those of the conventional full sternotomy performed by the same surgeon. The minimal approach led to accurate ASD and VSD repair without increased morbidity, but there was no evidence that MICS confers an advantage over the conventional approach. Other factors, such as cytokine levels and systemic inflammatory response, must be examined before the less invasive approach can be considered to be superior.
Another important factor is the greater technical difficulty of MICS. Almost all patients who underwent a minimal access approach had a simple cardiac anomaly, and some were operated on by residents with limited experience. To determine whether this method can be regarded as a standard operation that even residents can perform, the results of staff and resident surgeons were compared; however, the differences in the two patient groups makes this comparison difficult to interpret. Nevertheless, the results indicate that MICS can be performed safely by residents, in appropriate cases.
The conclusions that can be drawn from this retrospective study are limited in that the patient population was small, especially in the control group, the patients were not randomized, and the decision as to which surgeon performed the operation was left to the staff surgeon. As a result, some different patient characteristics were recognized. A further limitation of this study is that the potential advantage of pain reduction due to MICS is more difficult to assess in pediatric patients. 18 However, it was concluded that pediatric transatrial operations with a limited skin incision and partial sternotomy can be performed safely without compromising exposure. The patients and their parents were pleased with the good cosmetic results. As there were no procedure-related disadvantages when residents applied this technique on appropriate patients, we believe this limited skin incision and partial sternotomy can become a standard approach for simple congenital heart defects.