
Abstract
We report a 4-year-old girl who underwent replacement of a bioprosthetic valve in the tricuspid position due to rare bioprosthetic dysfunction. The bioprosthetic valve showed marked tricuspid insufficiency as well as stenosis caused by the adhesion of the preserved native valve leaflets to the undersurface of the implanted bioprosthesis.
Introduction
Excellent long-term results for bioprosthetic valves in the tricuspid position have been reported. Kawachi reported that freedom from structural tissue failure rate in tricuspid bioprostheses was as high as 94% at 10 years 1 and also demonstrated the superiority of bioprostheses over mechanical prostheses in the tricuspid position in both adults and a younger population. 2 Guerra also reported an acceptable long-term performance for tricuspid bioprostheses. 3 However, despite the reports of excellent long-term outcomes, we encountered a case of early deterioration of a tricuspid bioprosthesis, due to the adhesion of preserved native valve tissue to the bioprosthesis.
Case Report
The patient was a 4-year-old girl who was referred to Kitasato University Hospital with right heart failure due to bioprosthetic valve dysfunction in the tricuspid valve position. She previously underwent a tricuspid replacement with a Carpentier-Edwards bioprosthesis (23 mm) at the age of 2 years and 10 months due to tricuspid insufficiency following the repair of tetralogy of Fallot, at which time the native valve tissue was preserved. At admission, examinations showed hepatomegaly despite medication for heart failure and chest X-Ray showed a cardiomegaly with 70% cardiothoracic ratio. Echocardiography revealed massive tricuspid regurgitation at the center of the valve, which was also shown by the right ventricular angiography, and a markedly enlarged right atrium and right ventricle were noted (Figure 1). The right atrial pressure was 22 mm Hg with a pressure gradient across the bioprosthesis of 10 mm Hg.
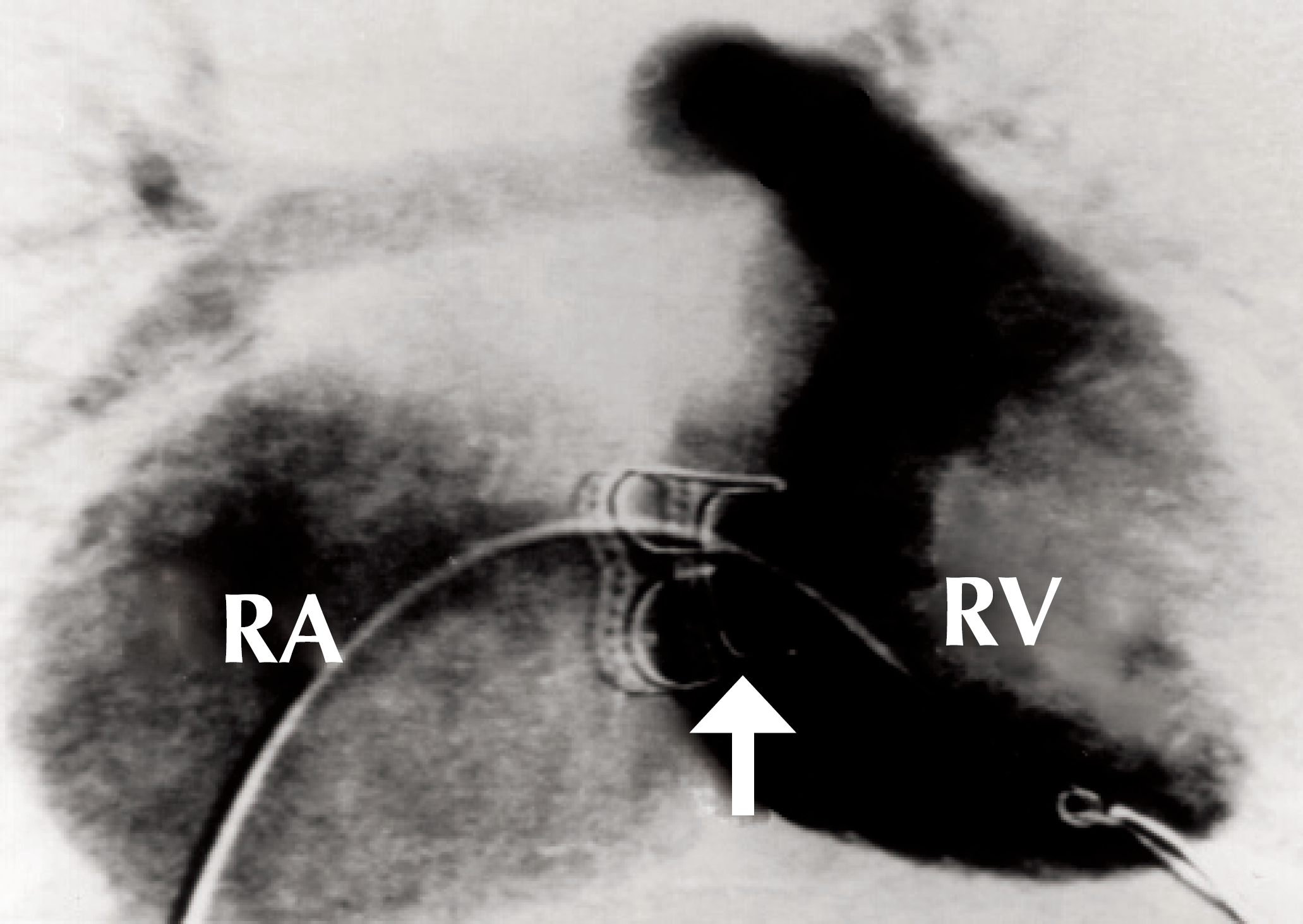
Right ventriculography revealed massive tricuspid valve regurgitation from the center of the bioprosthesis and the enlarged right atrium and right ventricle. The arrow shows the Carpentier-Edwards bovine pericardial prosthesis which was implanted in the tricuspid position while preserving the native tricuspid leaflets. RA = right atrium, RV = right ventricle.
Under cardiopulmonary bypass and cardioplegic cardiac arrest, the right atrium was opened. Since we initially intended to repair the previously preserved native valve and re-use it, we carefully inspected both the bioprosthesis and the native valve leaflets. Finally, we found that the tricuspid bioprosthesis was fixed in an open position and the valve leaflets were severely adhered to the undersurface of the tricuspid bioprosthesis when the native valve leaflets were peeled from the undersurface of the bioprosthesis. Thus, we considered that the adhesion of the native tissue to the bioprosthesis limited the movement of the bioprosthetic leaflets and resulted in structural failure (Figure 2). The bioprosthesis was carefully removed from the annulus. We abandoned re-using the preserved native valve, which seemed to hardly function as a tricuspid valve. A 25 mm Mosaic bioprosthesis (Medtronic, Minneapolis, MN, USA) was implanted after the native leaflets were excised. The excised native valve leaflets were carefully inspected and the bioprosthesis was examined by soft tissue roentgen photography, which showed no signs of calcification.
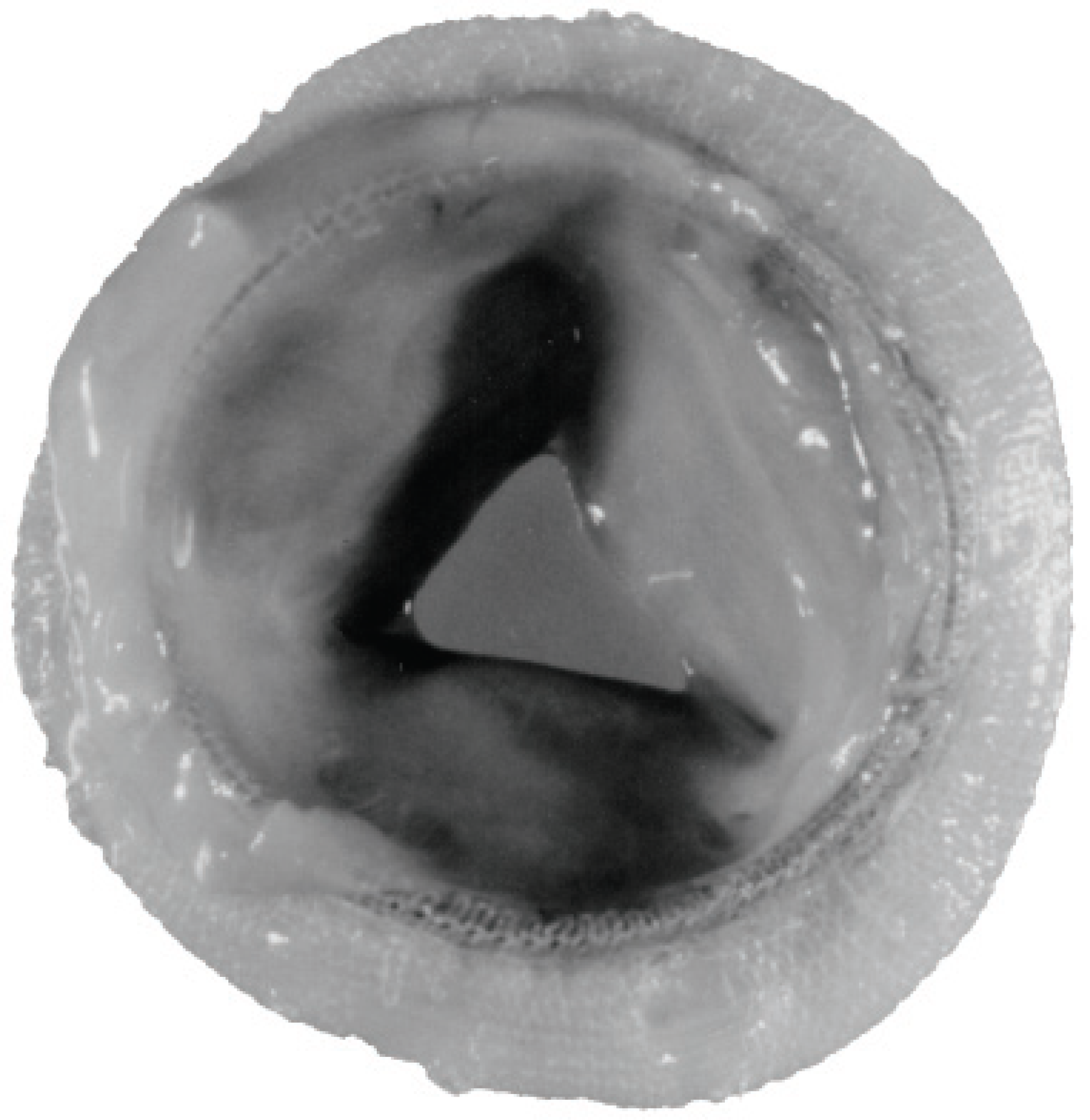
The extracted bioprosthesis. The valve leaflets were fixed open due to severe adhesion of native valve leaflets to the undersurface of the prosthesis. Since native leaflets were peeled from the bioprosthesis in trying to re-use them during surgery, they were not seen in this specimen.
The right atrial pressure was 5 mm Hg on the first postoperative day. The patient's postoperative course was uneventful and she was discharged from hospital on the seventh postoperative day. The patient is now active and is receiving furosemide at 1 mg·kg−1·day−1. The administration of Coumadin was ceased after the completion of a 3-month regime. At one year postoperatively, echocardiography showed no signs of valve dysfunction.
Discussion
Long-term follow-up studies have reported excellent results for bioprostheses in the tricuspid position in terms of survival rates, freedom from valve related complications such as hemorrhage, thromboembolism, structural valve failure and re-operations. 1 –5 Moreover, the results were better for bioprostheses than for mechanical valves in the tricuspid position. 2,5 Although the early deterioration of the tricuspid bioprosthesis is very rare, 1 –5 in our patient deterioration of the bioprosthetic valve function was speculated to be due to the adhesion of the preserved native valve tissue to the bioprosthesis.
Some surgeons like to preserve the native valve tissue to circumvent injury to the conduction tissue, to strengthen the annulus for anchoring the stitches and to preserve right ventricular function. However, the native tricuspid leaflets may result in adhesion to the bioprosthesis when they are preserved and left unfolded in the tricuspid replacement, because the native tricuspid valve leaflets tend to be so thin and smooth that they may come into close contact with the undersurface of the bioprosthesis during a whole cardiac cycle. Such adhesive native leaflets may then limit the movement of the bioprosthetic valve and cause insufficiency and stenosis of the bioprosthesis. Kitamura and colleagues 6 and Nemoto and colleagues 7 reported a series of adult cases in which the preserved native tricuspid valve leaflets were severely adhered to the implanted bioprosthesis and restricted the valve motion. Involved bioprostheses were replaced from 4 to 10 years after implantation. Therefore, we suggest that it is important for native tricuspid valve leaflets to be carefully folded when they are preserved in tricuspid valve replacement.