
Abstract
Significant venous hypercarbia has been reported in septic shock and circulatory failure. Cardiopulmonary bypass also impairs systemic and pulmonary blood perfusion. The objective of this study was to determine the clinical significance of the increased venous-arterial CO2 tension gradient resulting from venous hypercarbia after cardiopulmonary bypass. On arrival in the intensive care unit, venous and arterial CO2 tensions were measured in the radial and pulmonary arteries in 140 consecutive patients who had undergone coronary (n = 79), valve (n = 34), aortic (n = 20), and other (n = 7) surgery under cardiopulmonary bypass. The mean venous-arterial CO2 tension gradient was 5.0 ± 3.3 mm Hg (range, 7.7 to 15.7 mm Hg). By linear regression analysis, the factors that significantly correlated with venous-arterial CO2 tension gradient were bypass duration, aortic crossclamp time, initial arterial lactate level, transpulmonary arteriovenous lactate difference, arterial bicarbonate level, base excess, cardiac index, mixed venous O2 saturation, O2 delivery, O2 consumption, and the peak value of creatine kinase. The venous-arterial CO2 tension gradient may reflect impaired perfusion and anaerobic metabolism induced by cardiopulmonary bypass and could be a simple and useful indicator for patient management after surgery under cardiopulmonary bypass.
Introduction
It has been reported that venous hypercarbia and increases in the venous-arterial CO2 tension gradient (Pv-aCO2) may develop during circulatory arrest, traumatic shock, and severe sepsis associated with circulatory failure. 1 –5 Increases in venous CO2 tension (PvCO2) in these conditions appear to be related to critical reductions in systemic and pulmonary blood flow. Cardiopulmonary bypass (CPB) provides similar systemic and pulmonary conditions, which may be described as a “sepsis-like” syndrome. 6 The adverse effects of CPB, such as vasoconstriction, capillary permeability, and leukocytosis are attributed to altered arterial blood flow and exposure to foreign surfaces. Therefore, we speculated that Pv-aCO2 increases due to venous hypercarbia after CPB. We measured Pv-aCO2 and investigated its correlation with perioperative factors to determine its clinical significance in the postoperative management of patients undergoing surgery with CPB.
Patients and Methods
This study included 140 consecutive patients, 103 men and 37 women, with a mean age of 66 ± 9 years, undergoing surgery under CPB in Kasugai Municipal Hospital. The operations performed were: coronary bypass in 79 patients (bypass alone in 66, and bypass with valve surgery in 13), valve in 34 (mitral in 14, aortic in 15, and both in 1), and thoracic aortic surgery in 20 (ascending in 13, arch in 3, and descending in 4), and others (n = 7), including 33 emergency operations. In 17 patients undergoing aortic surgery, deep-hypothermic circulatory arrest with a minimum rectal temperature of 23.2°C ± 1.7°C and antegrade selective cerebral perfusion were applied. Other operations were performed under moderate hypothermic CPB with a minimum rectal temperature of 34.0°C ± 1.4°C. Anesthesia was induced with fentanyl (10 15 μg·kg−1) and midazolam, and maintained with a continuous infusion of propofol (3 4 mg·kg−1·h−1) and midazolam (0.05 0.1 mg·kg−1·h−1) in all patients. Muscle relaxation was achieved by intermittent administration of pancuronium. The following intraoperative variables were recorded to determine their correlation with Pv-aCO2: aortic crossclamp time, duration of CPB, and lowest rectal temperature.
Pulmonary artery pressure, right atrial pressure, mixed venous O2 saturation (SvO2), and cardiac index (CI) were monitored in every patient with a Swan-Ganz continuous cardiac output thermodilution catheter (744HF75; Baxter Healthcare, Irvine, CA, USA). To monitor arterial pressure, a catheter was placed in the radial artery. On arrival in the intensive care unit, baseline measurements of hemodynamic status were obtained and blood samples were drawn simultaneously from the arterial catheter and the distal port of the Swan-Ganz catheter. Blood gas analysis was performed at 37°C in a blood gas analyzer (ABL510; Radiometer, Copenhagen, Denmark). Based on the arterial (PaCO2) and mixed venous (PvCO2) CO2 tensions, Pv-aCO2 was calculated using the formula: Pv-aCO2 = PvCO2 − PaCO2. Postoperative variables were recorded to determine their correlation with Pv-aCO2. Immediate postoperative variables comprised: arterial pH, HCO3, base excess, PaO2/FiO2, alveolar arterial O2 difference [A-aDO2 = FiO2 − 713 − PaCO2/0.8 − PaO2], SvO2, CI, O2-delivery index [DO2I = CI − CaO2 − 10], O2 consumption index [VO2I = CI(CaO2 − CvO2) − 10], and O2-extraction rate [O2ER = VO2I/DO2I], where CaO2 is the arterial O2 content and CvO2 is the mixed venous O2 content. Lactate measurement was also performed at 37°C in an enzyme-electrode analyzer (EML105, Radiometer, Copenhagen, Denmark). Based on the arterial and mixed venous lactate levels (La and Lv, respectively), the transpulmonary arteriovenous difference (% La-v) was calculated using the formula: % La-v = 100(La-Lv)/Lv. Further postoperative variables were: peak plasma creatine kinase activity in routine serial 12-h measurements, and duration of intubation for mechanical ventilation.
All data are expressed as mean ± standard deviation. Statistical correlation of variables with Pv-aCO2 were assessed by linear regression analysis. A p value of less than 0.05 was considered to be statistically significant.
Results
The mean Pv-aCO2 was 5.0 ± 3.3 mm Hg (range, 7.7 to 15.7 mm Hg) immediately after surgery with CPB. A physiologically normal value of Pv-aCO2, up to 1 kPa or 7 mm Hg, was observed in 112 patients (80%). The Pv-aCO2 showed a positive correlation with aortic crossclamp time and duration of CPB (Table 1, Figure 1). In arterial blood gas analysis immediately postoperatively (Table 1, Figure 1), Pv-aCO2 correlated inversely with arterial bicarbonate level and base excess, although there was no correlation with the arterial pH. The Pv-aCO2 showed an inverse correlation with SvO2 and CI. Respiratory parameters such as PaO2/FiO2 and A-aDO2 did not show any correlation with Pv-aCO2. With regard to tissue O2 metabolism, both DO2I and VO2I correlated inversely with Pv-aCO2. The Pv-aCO2 correlated positively with the initial arterial lactate level and inversely with % La-v. Postoperative Pv-aCO2 values showed a positive correlation with peak plasma creatine kinase activity (Table 1, Figure 1). Three patients had difficulty in weaning from CPB and 2 did not survive the surgery; these numbers were too small to find any correlation of Pv-aCO2 with CPB weaning or mortality.
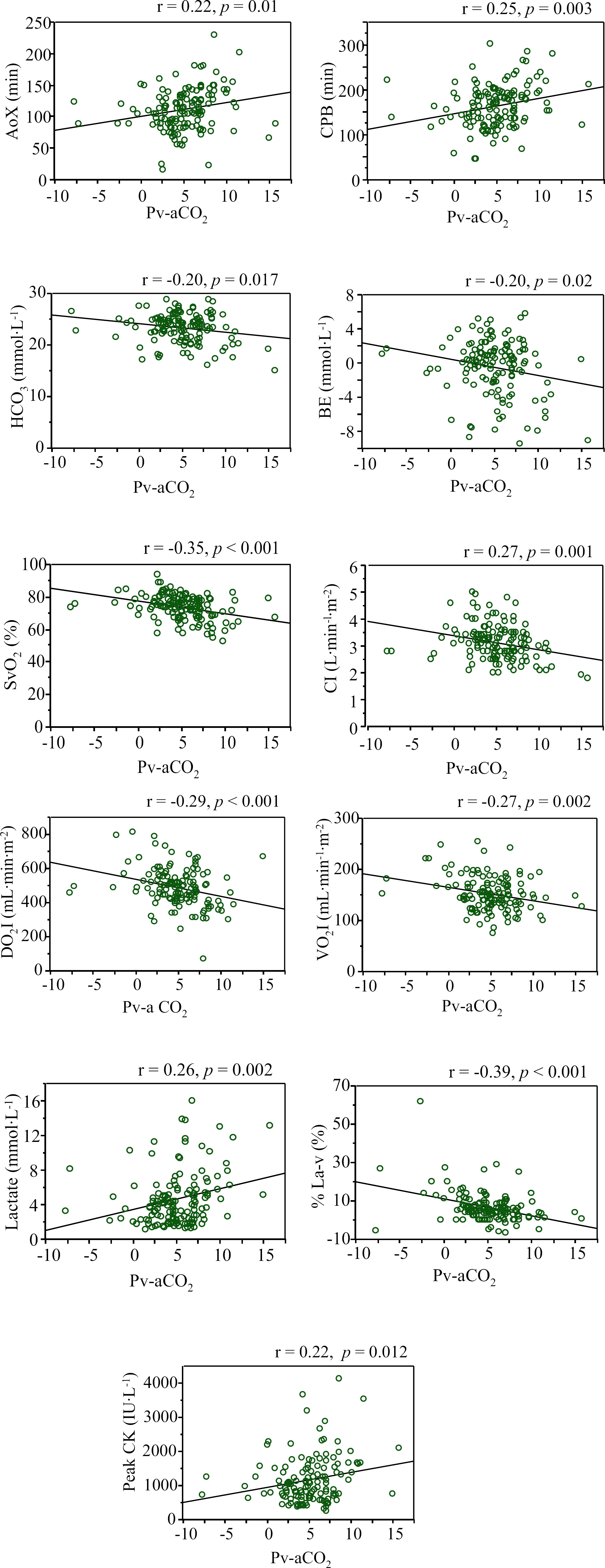
Correlation of the perioperative parameters with the venous-arterial CO2 tension gradient (Pv-aCO2). AoX = aortic crossclamp time, CPB = cardiopulmonary bypass time, BE = base excess, SvO2 = mixed venous oxygen saturation, CI = cardiac index, DO2I = oxygen delivery index, VO2I = oxygen consumption index, % La-v = transpulmonary arteriovenous difference of lactate levels, CK = creatine kinase.
Linear Regression Analysis of Venous-Arterial CO2 Tension Gradient and Perioperative Variables
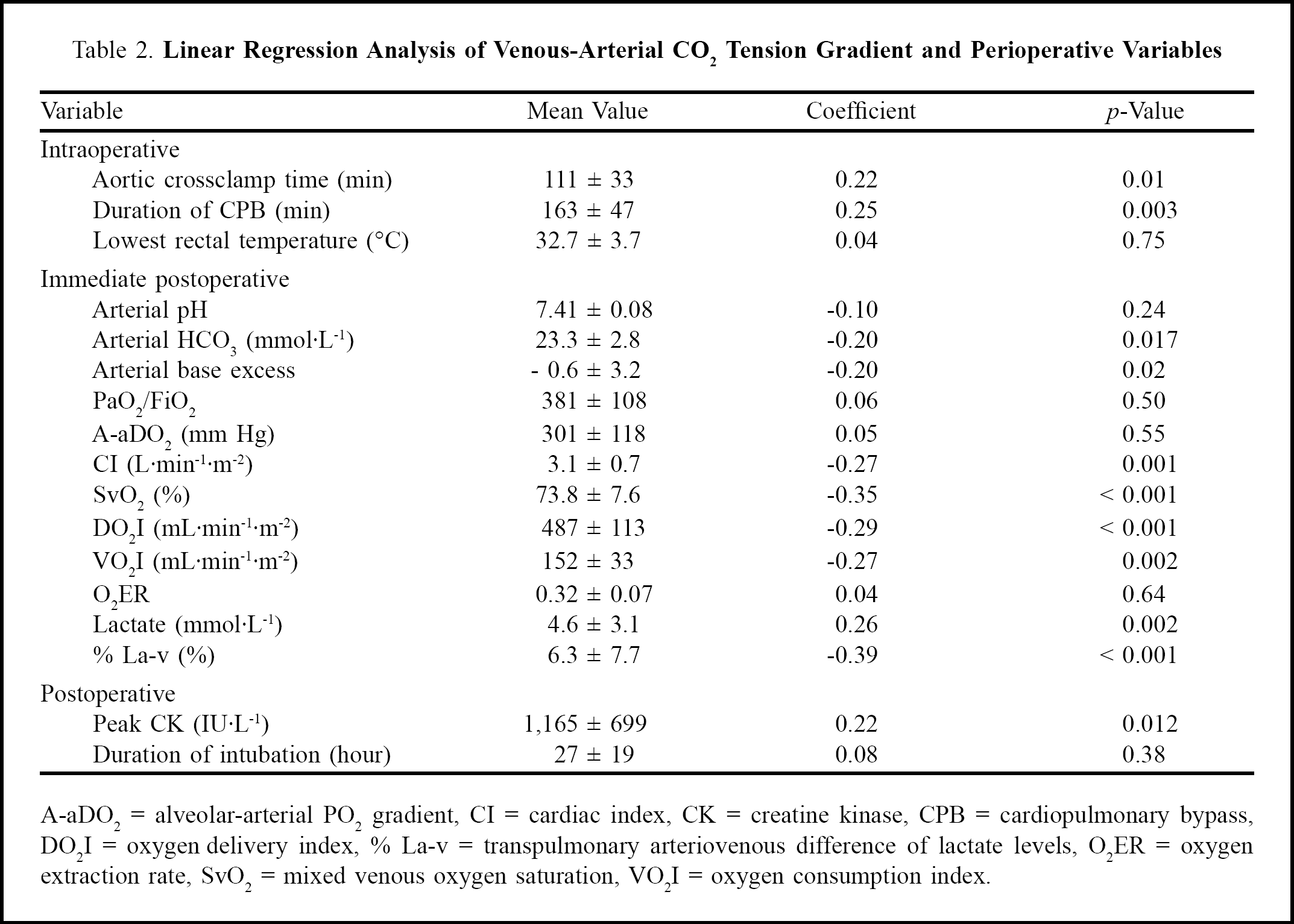
A-aDO2 = alveolar-arterial PO2 gradient, CI = cardiac index, CK = creatine kinase, CPB = cardiopulmonary bypass, DO2I = oxygen delivery index, % La-v = transpulmonary arteriovenous difference of lactate levels, O2ER = oxygen extraction rate, SvO2 = mixed venous oxygen saturation, VO2I = oxygen consumption index.
Discussion
The first main finding of our study was that Pv-aCO2 increased in most patients undergoing cardiovascular surgery with CPB. Increased Pv-aCO2 has been observed during other low blood flow states such as circulatory collapse, septic shock, traumatic shock, hemorrhagic shock, and cardiac tamponade. 1 –5 There was one report of increased Pv-aCO2 after CPB; however, it included only 10 patients. 7 Our study enrolling 140 patients provides more accurate and detailed data with regard to Pv-aCO2 after CPB.
Under normal conditions, 80% of CO2 exchange in the lung is mediated by carbonic anhydrase-catalyzed dehydration of HCO3. 8 Therefore, most CO2 produced in the tissues is transported as HCO3. 9 The development of venous hypercarbia after CPB seems to be related to critical reductions in systemic and pulmonary blood flow during CPB and cardiac arrest, resulting in impaired CO2 elimination and exchange. It has been reported in animal models that a 3-fold increase in Pv-aCO2 is associated with a 50% reduction in cardiac output. 10 A previous report also demonstrated that increasing CI or systemic blood flow by fluid resuscitation and blood transfusion resulted in a reduction of Pv-aCO2 in critically ill patients. 5 During anaerobic metabolism at low systemic and peripheral perfusion, CO2 is increasingly produced from both the buffering of acids, such as lactic acid, by HCO3 and from anaerobic decarboxylation. In addition, the buffering capacity of blood is impaired, resulting in a decrease in the relative amount of CO2 transported as HCO3, and thus a further increase in Pv-aCO2. Low pulmonary blood flow unbalances the ventilation/perfusion ratio of the lung and reduces pulmonary CO2extraction associated with venous respiratory acidosis. 3 Both metabolic and respiratory acidosis associated with decreased HCO3, by which CO2 is transported from the tissues, may cause an increase of Pv-aCO2. This mechanism is supported by our finding that decreased HCO3 was closely related to increased Pv-aCO2.
The second main finding of our study was that the degree of increased Pv-aCO2 was closely associated with the invasiveness of the surgery under CPB. Longer CPB time and aortic crossclamp time correlated positively with Pv-aCO2. Increased Pv-aCO2 was also closely related to decreased CI, SvO2, arterial HCO3, and base excess, as were an increased lactate level and a higher peak plasma creatine kinase level, all of which may be the results of more invasive surgery. Furthermore, higher DO2I and VO2I, indicating the “hypermetabolic” state after invasive CPB, were closely related to decreased Pv-aCO2. 6 Increased Pv-aCO2 may reflect impaired perfusion and anaerobic metabolism induced by CPB.
This study also revealed interestingly that Pv-aCO2 correlated inversely with the initial transpulmonary arteriovenous lactate difference (% La-v) which indicates the severity of lung injury caused by surgery. We have reported that severe hypoxia of the lungs is closely associated with increased % La-v. 11 Especially with CPB, lower temperature and reduced pulmonary blood flow induces more lung damage. The pathophysiological mechanism of the increased Pv-aCO2 described above explains the close correlation between Pv-aCO2 and % La-v. However, there was no relationship between Pv-aCO2 and the initial PaO2/FiO2 in the intensive care unit, A-aDO2, or the duration of intubation for mechanical ventilation. Further studies are needed to reveal the clinical significance of the relationship between Pv-aCO2 and % La-v.
One of the limitations of our study is that we did not investigate the correlation of Pv-aCO2 with clinical morbidity and mortality. We should have included not only laboratory parameters but also clinical parameters to reveal the clinical significance of Pv-aCO2 in detail. The second limitation is that the correlation coefficient is actually rather weak. This weakness could be due to the wide range of measured Pv-aCO2. Another limitation is that we did not investigate the possible effect of arteriovenous shunting in the peripheral tissues with impaired perfusion after CPB. When shunting occurs, inadequate tissue O2 delivery is exacerbated, associated with an increase in plasma lactate and a fall in Pv-aCO2. We did not find any data to elucidate the precise mechanism of the increased Pv-aCO2 after CPB. However, as the Pv-aCO2 value may reflect impaired perfusion and anaerobic metabolism induced by CPB, it could be a simple and useful indicator, in parallel with the above factors, of the invasiveness of CPB surgery for postoperative patient management.