
Abstract
A 35-year-old woman was found on echocardiography to have a pseudoaneurysm of the mitral-aortic intervalvular fibrosa, residual ventricular septal defect, and aortic regurgitation. She had undergone surgical closure of a ventricular septal defect at age 7 and was found to have residual shunt several years later. She had been followed nonsurgically and had symptoms of cardiac failure during her 2 pregnancies. The pseudoaneurysm and the septal defect were successfully repaired.
Introduction
Pseudoaneurysm of the mitral-aortic intervalvular fibrosa is rare but may occur as a complication of cardiac surgery, endocarditis, or chest trauma. We report the successful treatment of a patient with this lesion in association with residual ventricular septal defect (VSD) and moderate aortic regurgitation.
Case Report
A 35-year-old woman had undergone surgical repair of a VSD when she was 7 years old and was found to have residual shunt several years later. She was followed nonsurgically and had no signs of cardiac failure except during her 2 pregnancies at age 25 and 29. These episodes were treated with diuretics. She was eventually referred to us with cardiomegaly and a tendency towards lung congestion. Echocardiography revealed residual left-to-right shunt, aortic regurgitation, and a small lesion in the mitral-aortic intervalvular fibrosa presenting as a pseudoaneurysm that communicated directly with the left ventricle and expanded during systole (Figures 1 and 2). A left ventriculogram confirmed systolic expansion of the pseudoaneurysm (Figure 3) and a perimembranous residual VSD with a shunt fraction of 2.5.
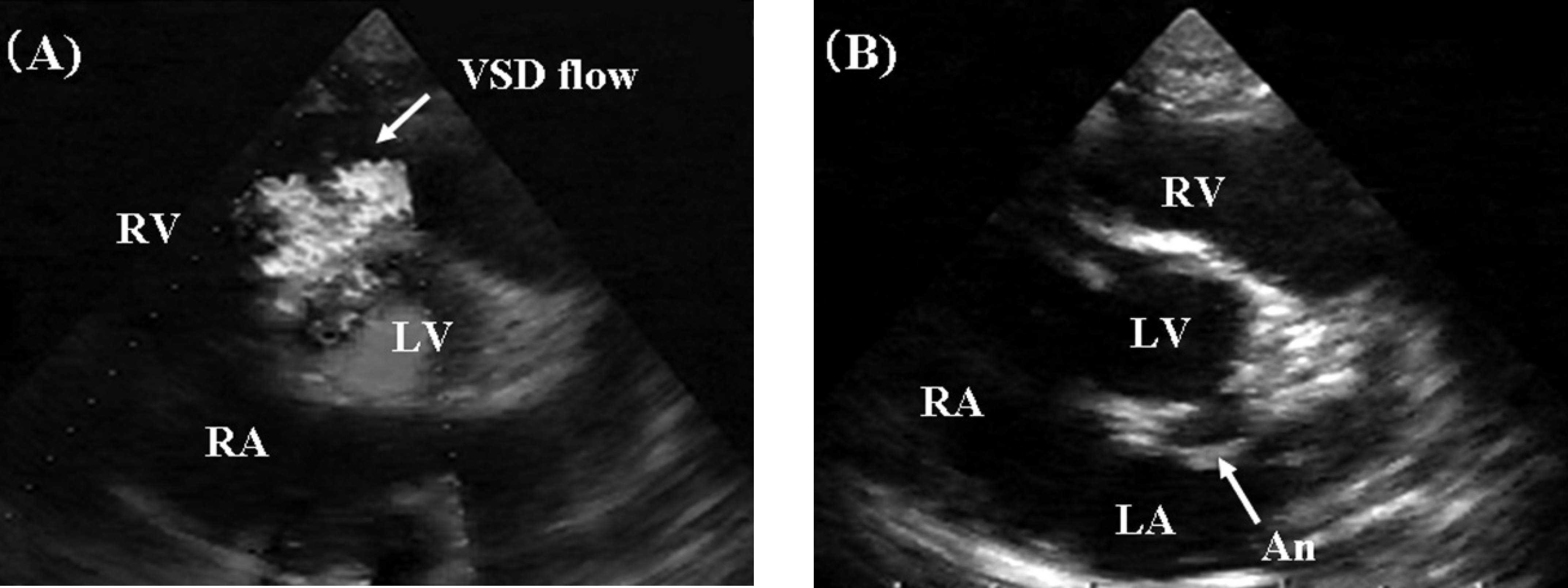
Transthoracic echocardiogram in the short-axis view showing a residual ventricular septal defect in the perimembranous portion with pouch formation
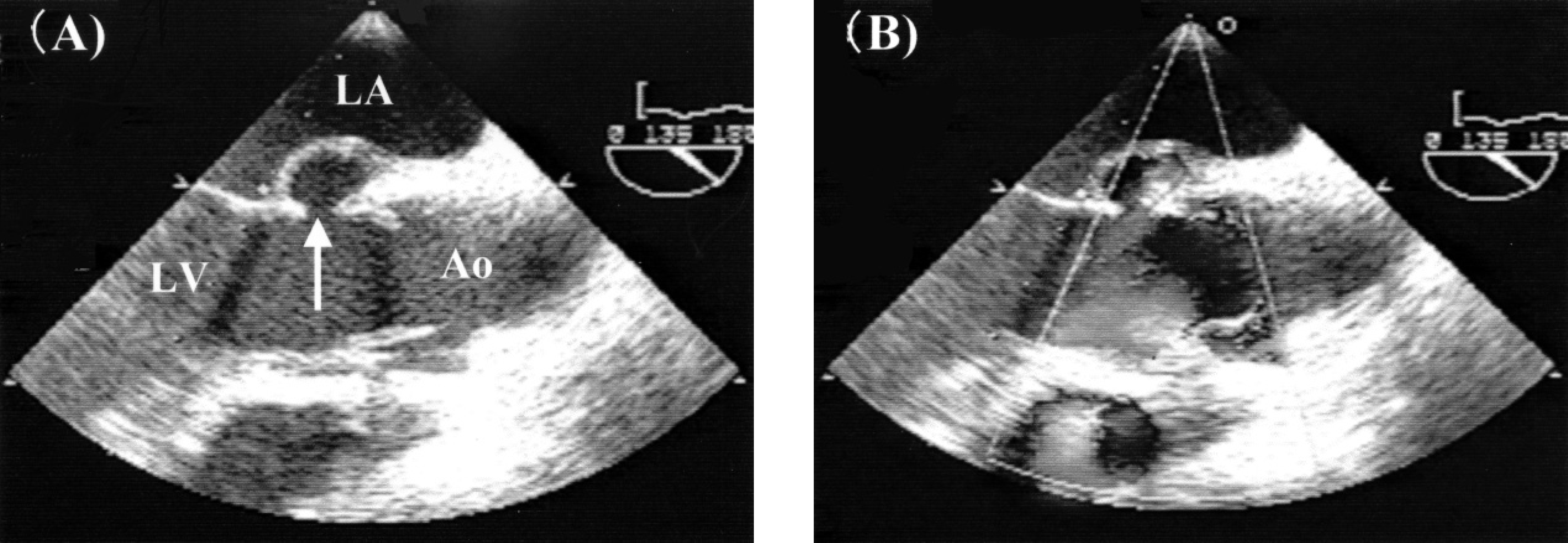
Transesophageal echocardiogram showing a mitral-aortic intervalvular pseudoaneurysm protruding into the left atrium

Left ventriculogram showing expansion of the pseudoaneurysm (arrows) during systole. Ao = aorta, RV = right ventricle, LV = left ventricle, An = pseudoaneurysm.
Surgical repair was performed under cardioplegia and bicaval cannulation. A right atrial incision was made. The VSD was confirmed to be perimembranous and was covered by an aneurysmal pouch and the tricuspid septal leaflet. It appeared to have arisen from a muscle tear caused by the stitches inserted during the previous VSD closure. The mitral-aortic intervalvular lesion was visualized through the VSD and was about 5 mm in diameter (Figure 4). Both defects were closed using Dacron patches with continuous sutures. The ascending aorta was opened, and the slightly lowered left coronary and noncoronary cusps of the aortic valve were suspended.
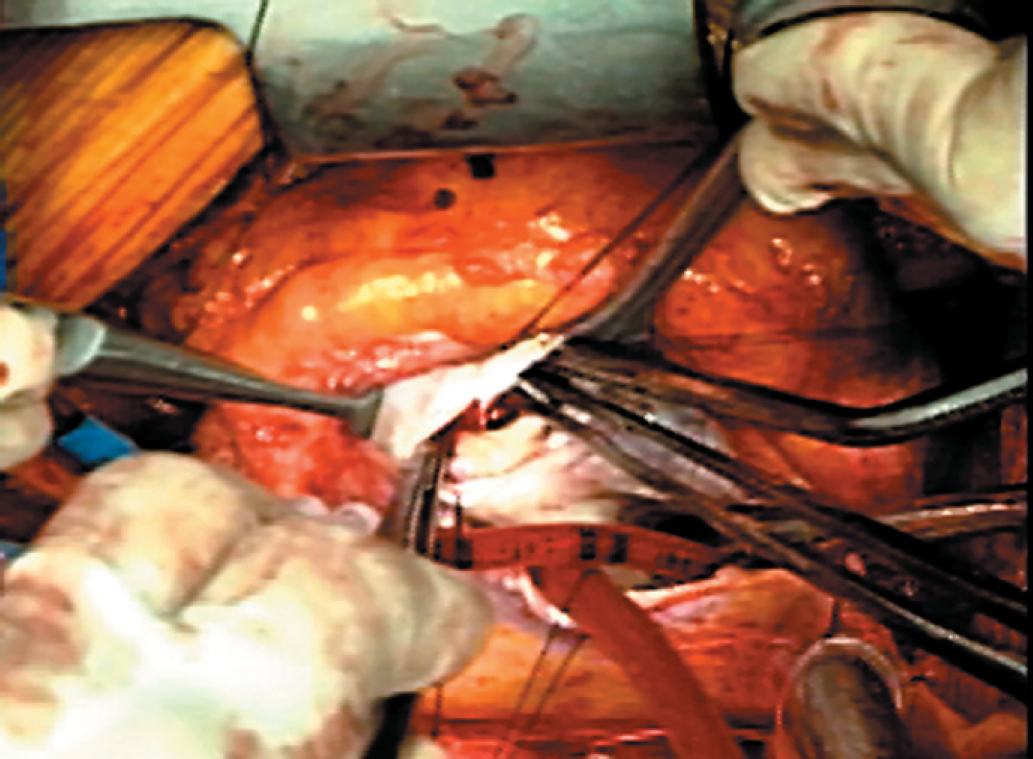
Intraoperative view of the mitral-aortic intervalvular lesion (arrow). RA = right atrium, RV = right ventricle, TV = tricuspid valve.
The postoperative course was uneventful. Echocardiography showed trivial aortic regurgitation, no residual shunt, and reduced left ventricular size. The patient was discharged on the 11th postoperative day.
Discussion
A lesion in the aortic-mitral annulus can cause aneurysm of the mitral valve or the left ventricular outflow tract and may be a complication of aortic or mitral valve surgery, aortic valve endocarditis, or chest trauma. 1 –3 Subvalvular left ventricular aneurysm can be congenital or secondary to weakness in the ventricular wall in the region of the atrioventricular groove. 4 Aneurysms of such lesions have been described as pseudo- or false aneurysms: consisting of no endocardial elements. These pseudoaneurysms are thought to arise as a result of perforation of the mitral-aortic intervalvular fibrosa and subsequently expand during systole. They have been reported to cause coronary artery compression resulting in coronary ischemia, and rupture can cause acute mitral regurgitation or cardiac tamponade, followed by acute cardiac failure or sudden death, resulting in a true surgical emergency. 5 –7 Pseudoaneurysms should be surgically treated as soon as possible after diagnosis.
Our patient had no history of endocarditis, chest trauma, or aortic or mitral valve surgery. Although the etiology could not be established definitively, it is possible that the mitral-aortic intervalvular fibrosa was injured by forceps or a needle during the previous VSD closure, as the lesion was just behind the VSD. Another possibility is that the pseudoaneurysm was congenital, however there was no record of its existence from the previous operation.
As the mitral-aortic intervalvular fibrosa was in close approximation with the perimembranous VSD, surgical closure of this type of VSD had to be performed with great care. In this case, preoperative transesophageal echocardiography was very effective for visualizing this region and for making a definitive diagnosis. Transthoracic echocardiography should also be considered as an essential component of postoperative follow-up in patients with perimembranous VSD.