
Abstract
The effect of the ultra-short-acting beta blocker, landiolol, on ischemic preconditioning was examined in isolated rabbit hearts. Ischemic preconditioned hearts received 2 episodes of 5 min each of global ischemia and reperfusion. The left anterior descending coronary artery was occluded for 1 hour and reperfused for 1 hour. Left ventricular end-systolic and end-diastolic pressures and infarct size were measured. Seven control hearts had no drug infused. Four groups of 6 hearts each were pretreated with 1 or 3 μM of landiolol or a combination of 1 or 3 μM landiolol and ischemic preconditioning. A further group of 6 hearts had ischemic preconditioning without landiolol. Ischemic preconditioning significantly reduced left ventricular end-diastolic pressure and infarct size compared to the controls. Landiolol alone did not change left ventricular end-diastolic pressure or infarct size, but landiolol 3 μM and ischemic preconditioning decreased left ventricular end-diastolic pressure more than preconditioning alone. These data suggest that pre-ischemic landiolol infusion may enhance the cardioprotective effect of ischemic preconditioning.
Introduction
Ischemic preconditioning (IPC) enhances tolerance to subsequent ischemic injury. 1,2 Ischemic preconditioning results in changes such as reduction of infarct size, preservation of ionic homeostasis, and a decrease in ventricular arrhythmias after ischemia-reperfusion. Several researchers, including ourselves, have proposed subcellular mechanisms for the IPC response, including the mitochondrial adenosine triphosphate-sensitive potassium channel, nitric oxide, protein kinase C, opioid receptors, and β-adrenergic receptors. 3 –7 Sandhu and colleagues 8 reported that β-receptor stimulation before ischemia reduced infarct size and mimicked IPC effects. An increase in cyclic adenosine monophosphate, a key mediator of the β-receptor signaling pathway, is essential for the IPC response. Moreover, we have recently shown that IPC fails to protect after myocardial infarction, but the adenylate cyclase agonist forskolin restores the protective effects of IPC. 9 This accumulated evidence indicates that β-receptors are involved in the IPC mechanism.
Recent experiments have shown beneficial effects of blocking β1-adrenergic receptors in ischemia-reperfusion injury. 10 However, we found that β2-receptors play a pivotal role in the IPC protective response. 11 This suggests that β1 blockade might enhance the cardioprotective effect of IPC, whereas activation of β2 receptors is associated with the cardioprotective effect of IPC. To assess the role of β1 blockade in IPC, we used a specific β1 blocker, landiolol. Landiolol (ONO-1101) is an ultra-short-acting beta blocker with a shorter half-life (4 min) and higher affinity for β1 receptors (255-fold > β2 receptors) than other ultra-short-acting beta blockers. 12 However, the precise effect of β1 blockade during the IPC response is unknown. The purpose of this study was to determine the effect of landiolol on IPC in isolated perfused rabbit hearts.
Materials and Methods
All animals received humane care in compliance with the “Guide for the Care and Use of Laboratory Animals” prepared by the Institute of Laboratory Animal Resources, Commission on Life Sciences, National Research Council, and published by the National Academy Press, revised 1996. Thirty-seven adult male New Zealand rabbits, weighing 6–7 kg, were anesthetized with sodium pentobarbital (30 mg·kg−1) and anticoagulated with sodium heparin (200 U·kg−1) via an ear vein. Once the corneal reflex was abolished, the rabbits were placed in the supine position and the chest was entered through a bilateral thoracotomy. The heart was rapidly excised and placed in an ice-bath (4°C) of Krebs-Henseleit solution (Na+ 135 mM, K+ 4.7 mM, Ca2+ 1.7 mM, PO4 − 1.1 mM, Mg2+ 1.2 mM, HCO3 − 25 mM, glucose 11.5 mM, pyruvate 4.9 mM, fumarate 5.4 mM). The aorta was cannulated, and the heart was suspended within a heated glass chamber. The aorta was perfused with oxygenated (95% O2 + 5% CO2) Krebs-Henseleit solution at 37°C and 75 mm Hg root pressure, and the pulmonary artery was incised. The heart was allowed to equilibrate for 30 min while the left atrium was excised and a water-filled balloon was placed through the mitral valve into the left ventricle. The initial left ventricular end-diastolic pressure (LVEDP) was set at 5–10 mm Hg by water inflation, and the volume remained constant throughout the experiment. Left ventricular end-systolic pressure (LVESP) and LVEDP were measured from the balloon tracing. The heart was paced at 150 beats·min−1 with an asynchronous pacemaker. Ischemia was induced by ligating the left anterior descending coronary artery (LAD) close to its origin with 3/0 silk suture. After 1 hour of ischemia, reperfusion was achieved by releasing the ligature and briefly massaging the LAD with a moistened cotton swab. After 1 hour of reperfusion, the heart was removed from the perfusion apparatus, religated, and 3 mL of 0.4% disodium indigotin-disulfonate (Daiichi Pharmaceutical Co., Ltd., Tokyo, Japan) was infused through the aortic cannula. The right ventricle was excised, and the left ventricle was sectioned horizontally at 2-mm intervals into 5 or 6 slices. The slices were incubated with triphenyltetrazolium chloride (Sigma Chemical Co., St. Louis, MO, USA) at 37°C, pH 7.4, for 15 min. The unstained area was scanned (SigmaScan Pro; SPSS, Inc., Chicago, IL, USA) and the infarcted area was labeled. The infarcted area (IA) was expressed as a percentage of the total area at risk. The overall infarcted area was computed as a weighted average of the slices by weight.
The experimental protocol is shown in Figure 1. Seven hearts served as a control group without any treatment prior to LAD ischemia and reperfusion. In another 6 hearts, IPC was accomplished with two 5-min episodes of complete aortic occlusion followed by 5 min of reperfusion prior to LAD ischemia. Four groups of 6 hearts each were pretreated with 1 or 3 μM of landiolol (Ono Pharmaceutical Co., Ltd., Osaka, Japan) or a combination of 1 or 3 μM of landiolol and IPC prior to LAD ischemia. To evaluate the effect of landiolol on cardiac pressure, LVEDP and LVESP were measured 5 min after 1 μM (n = 6) and 3 μM (n = 6) of landiolol infusion.
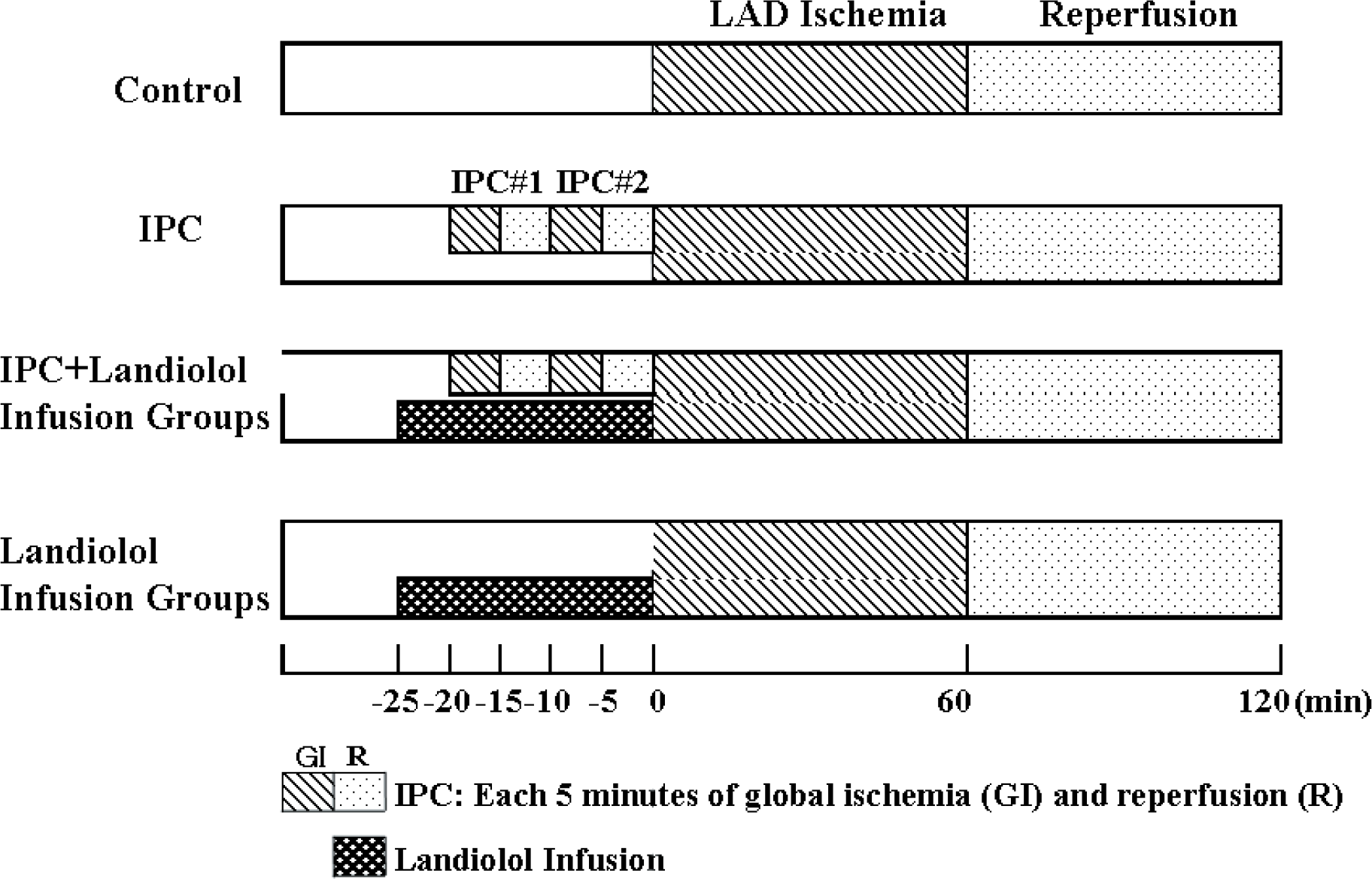
Experimental protocol: landiolol was infused during pretreatment and ischemic preconditioning (IPC), but not during regional ischemia or reperfusion, landiolol was infused from −25 to 0 min and IPC consisting of 2 cycles of 5-min global ischemia and reperfusion, regional ischemia of the left anterior descending coronary artery (LAD) occurred from 0 to 60 min, and reperfusion from 60 to 120 min.
All results are expressed as mean ± standard error. LVEDP and LVESP data were analyzed using two-way repeated measures analysis of variance. Infarct size was analyzed using one-way analysis of variance. The effect of landiolol was analyzed using the paired two-tailed t test. Statistical analyses were performed using GraphPad Prism version 4 (GraphPad Software Inc., San Diego, CA, USA). A p-value < 0.05 was considered significant.
Results
Infusion of landiolol per se tended to decrease LVESP but it did not reduce LVEDP compared to the pretreatment value (Table 1). Changes in LVEDP during the experiment are shown in Figure 2. Baseline LVEDP was preserved during pretreatment and LAD ischemia in all groups. Ischemic preconditioning reduced LVEDP compared to controls (p = 0.06). Landiolol 3 μM + IPC reduced LVEDP after reperfusion compared to IPC alone (p = 0.03) or controls (p < 0.01). Landiolol 3 μM + IPC also reduced LVEDP compared to landiolol 3 μM (p = 0.01), landiolol 1 μM (p < 0.01), and landiolol 1 μM + IPC (p < 0.01). Landiolol 1 μM + IPC did not reduce LVEDP compared to IPC alone (p = 0.19), landiolol 1 μM (p = 0.35), or controls (p = 0.70). Landiolol 1 μM did not affect LVEDP compared to controls (p = 0.14) or IPC alone (p = 0.68). Changes in LVESP during the experiment are shown in Figure 3. Regional LAD ischemia decreased LVESP in all groups, and it did not recover to the pretreatment value in any group. None of the treatments had a significant effect on LVESP: IPC vs. controls, p = 0.35; landiolol 3 μM + IPC vs. IPC, p = 0.33; landiolol 3 μM + IPC vs. controls, p = 0.95; landiolol 3 μM + IPC vs. landiolol 3 μM, p = 0.62; landiolol 3 μM + IPC vs. landiolol 1 μM or 1 μM landiolol + IPC, p = 0.83. Infusion of 1 μM of landiolol before ischemia with IPC did not change LVESP vs. IPC (p = 0.47), landiolol 1 μM (p = 0.95), or controls (p = 0.88). Landiolol 1 μM alone did not change LVESP compared to controls (p = 0.74) or IPC (p = 0.45).
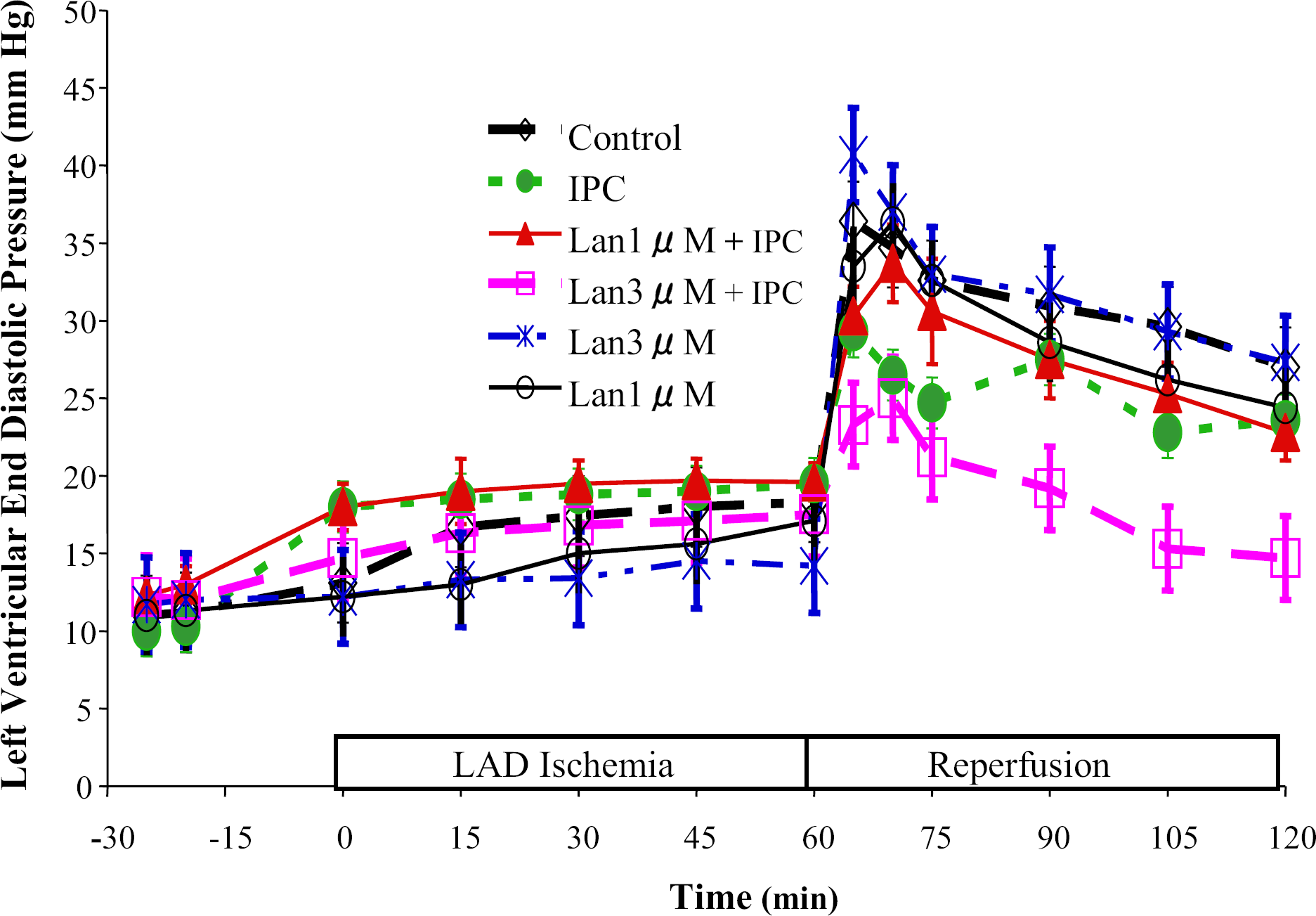
Time-course of changes in left ventricular end-diastolic pressure, left ventricular end diastolic pressure in the Lan3μM + IPC group was significantly lower than the other groups. IPC = ischemic preconditioning, Lan1μM = pretreatment with 1 μM of landiolol, Lan3μM = pretreatment with 3 μM of landiolol.
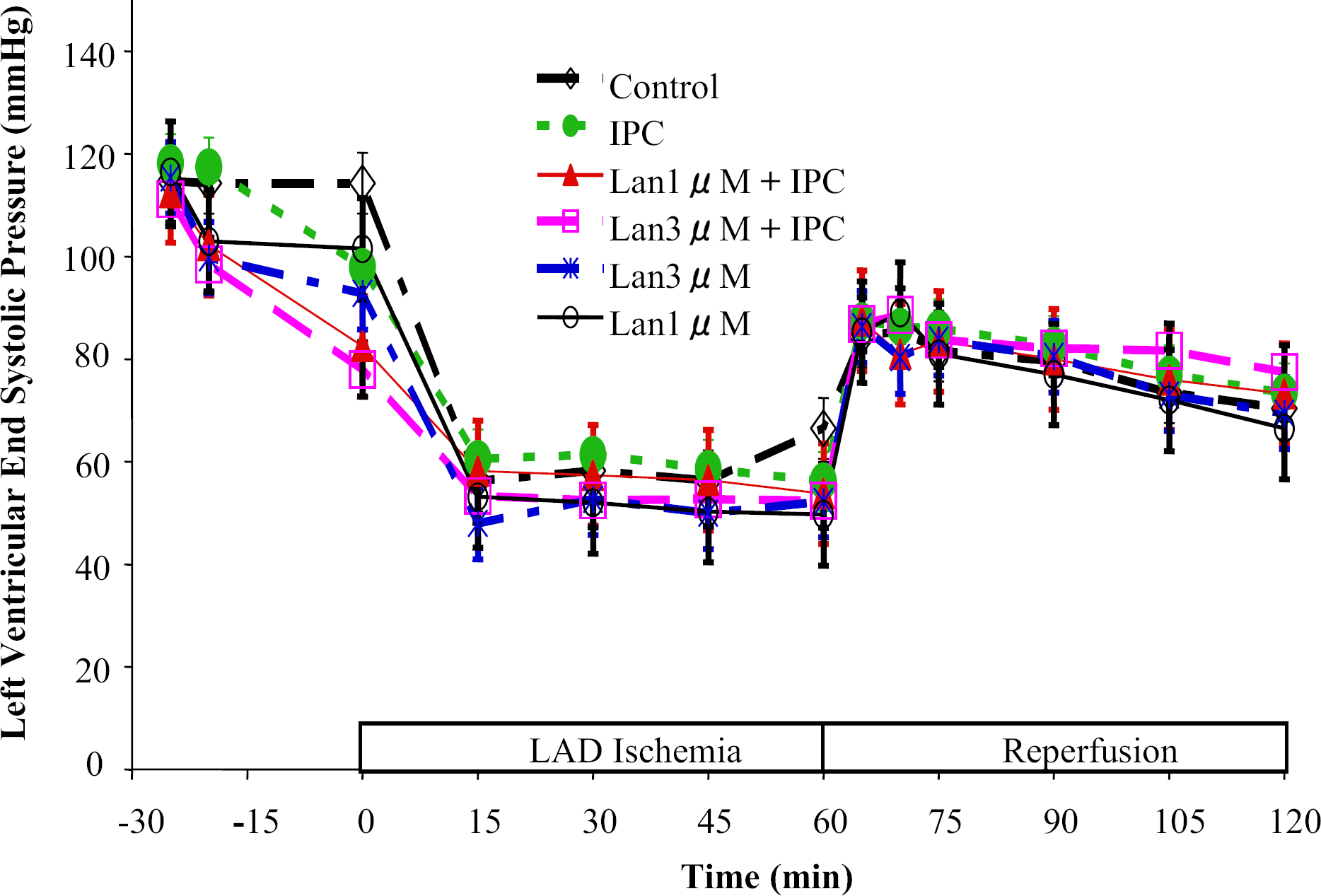
Time-course of changes in left ventricular end-systolic pressure during the experiment, there were no significant difference between the groups. Abbreviations as in Figure 2.
Beta-blocking Activity Of Landiolol
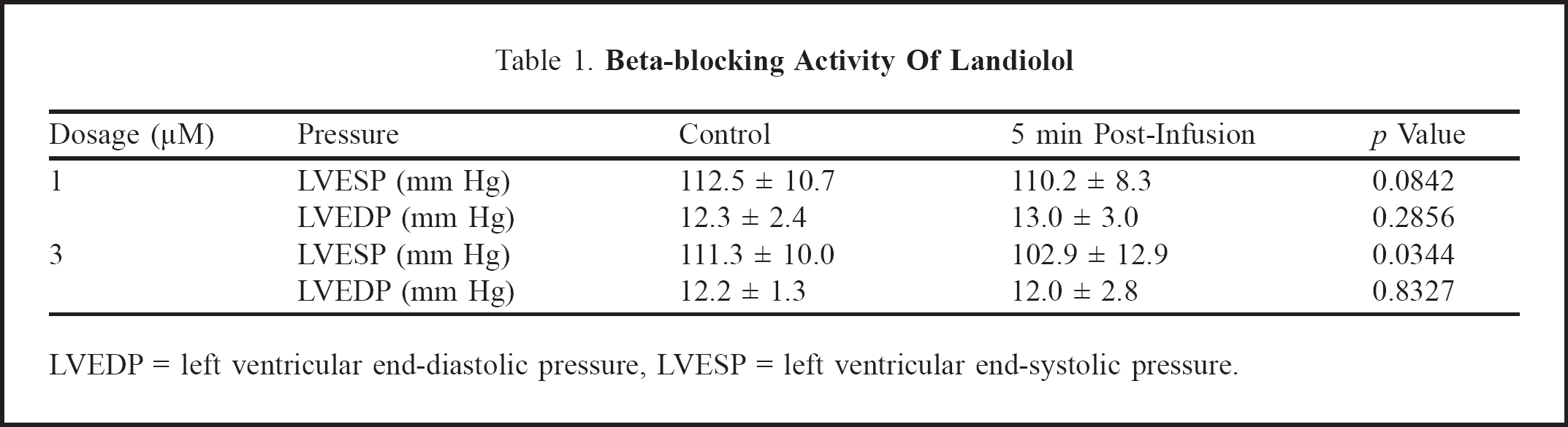
LVEDP = left ventricular end-diastolic pressure, LVESP = left ventricular end-systolic pressure.
Infarct size is shown in Figure 4. Control hearts had an IA of 48% ± 4%. Ischemic preconditioning reduced IA to 25% ± 3% (p < 0.01 vs. controls). Landiolol 3 μM + IPC and 1 μM + IPC also reduced IA to 17% ± 3% and 22% ± 3%, respectively (p < 0.01 vs. controls for both doses). No significant difference in IA was observed between IPC and landiolol 3 μM + IPC (p = 0.11). Landiolol 3 μM alone did not reduce IA (p = 0.8093 vs. controls). Landiolol 3 μM + IPC reduced IA compared to 3 μM (p < 0.01) and 1 μM alone (p < 0.01). No significant difference was found between 1 and 3 μM of landiolol.
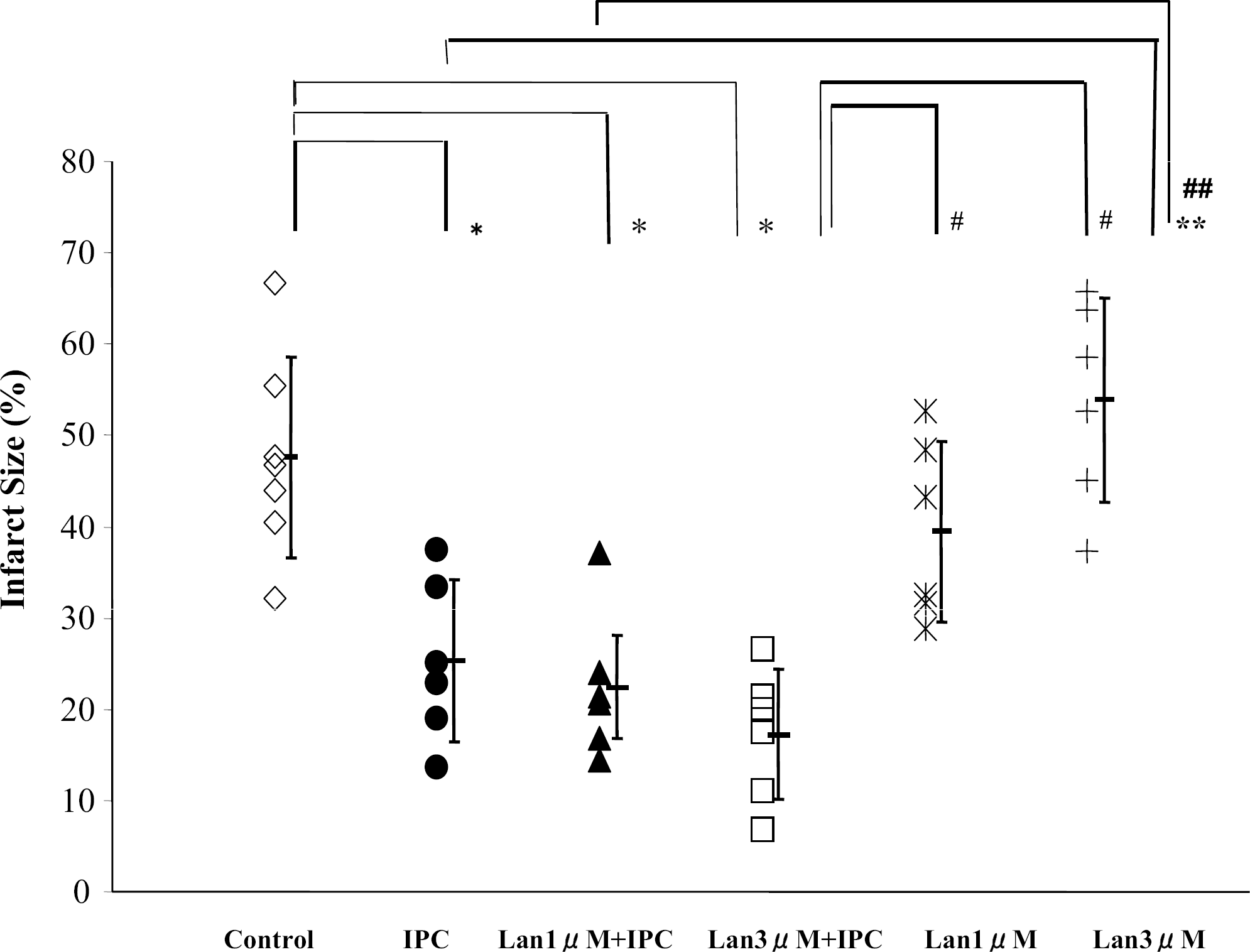
Left ventricular infarct size (% of area at risk), significant differences versus control, IPC, IPC + Lan1μM, Lan3μM, and IPC + Lan3μM are designated by *, **, ##, and #, respectively. Abbreviations as in Figure 2.
Discussion
These results demonstrate that pre-ischemia infusion of landiolol enhances the cardioprotective effect of IPC after reperfusion. Ischemic preconditioning reduces infarct size and arrhythmic events, and improves left ventricular function. Recent reports suggest that β-adrenergic receptor stimulation is involved in the mechanism of IPC. During short periods of ischemia, IPC causes release of catecholamines, resulting in increased catecholamine concentration in the myocardium. In agreement with these results, this study demonstrated that IPC reduced LVEDP and infarct size. Pre-ischemic β-adrenergic stimulation by isoproterenol administration also reduces infarct size. 7 Lochner and colleagues 13 demonstrated that IPC increases cyclic adenosine monophosphate concentration, a downstream effect of β-receptor stimulation during the short period of preconditioning, suggesting a mechanism for the IPC-mediated effects. Adenylate cyclase activity is also increased in preconditioned hearts. 14 This accumulated evidence suggests that β-receptor activation during IPC activates the β-adrenergic signaling pathway, and promotes the cardioprotective effect after reperfusion.
Landiolol is a highly cardioselective agent with a 255-fold higher affinity for β1-adrenergic receptors than β2-receptors. 15 In comparison with other beta blockers, esmolol, widely used as an ultra-short-acting beta blocker, has a 33-fold greater affinity for β1-receptors than β2-receptors, while propranolol, a non-selective beta blocker, possesses a 0.68-fold greater affinity for β1-receptors. It is known that the β1-receptors are 60%–80% of the total β-receptors in myocardium. The 2 types of receptor have different systems to regulate downstream signaling. 16 For example, β1-receptor stimulation induces apoptotic effects through Gs proteins, while β2-receptor stimulation shows anti-apoptotic effects due to the dual coupling systems through Gs and Gi proteins. The dual coupling system is thought to contribute to cell survival in various types of injury including ischemia. Although further studies are needed to investigate to what extent the β2-receptor signaling pathway is activated in this model, it is possible that landiolol specifically blocks β1-receptors, leading to enhanced or selective activation of the β2-receptor signaling pathway.
We have previously shown that IPC fails to provide cardioprotective effects in hearts in which β2-receptor expression is decreased after myocardial infarction, and that gene transfer of β2-receptors enhances the cardioprotective effects of IPC, resulting in preservation of left ventricular pressure after reperfusion. 9,11 In addition, the adenylate cyclase agonist forskolin restores the refractory effect of IPC in the heart after myocardial infarction. The present results, therefore, imply that pre-ischemic infusion of landiolol in combination with IPC may allow IPC to activate β2-receptor signaling in the absence of β1-receptor signaling pathways. Acute myocardial ischemia rapidly induces catecholamine release from nerve terminals. Ischemic preconditioning caused by repetitive and reversible ischemic stress protects myocardium from subsequent prolonged ischemia. However, there may not be an increase in catecholamines without IPC, which may explain why landiolol infusion alone failed to show cardioprotective effects after reperfusion. In addition, because landiolol has only a 4-min half-life in plasma, our results are not related to the direct effect of landiolol on LVEDP at 1 hour after reperfusion. 12 It is generally accepted that IPC exhibits a cardioprotective effect after repetitive and/or more than 5 min of ischemia, and that this effect continues for 2–3 hour after reperfusion. 17 Therefore, a pre-ischemic infusion of landiolol is likely to enhance the cardioprotective effect of IPC, resulting in inhibition of the increase in LVEDP during reperfusion.
Landiolol may have its own cardioprotective effects against ischemia-reperfusion injury. Yasuda and colleagues 18 reported that landiolol has the potential to enhance post-ischemic cardiac function after warm cardioplegic arrest in isolated rat heart. Kurosawa and colleagues 10 demonstrated that infusion of landiolol for 10 min before global ischemia preserved left ventricular pressure after reperfusion. As we saw no protective effect of landiolol alone, our results are not in accordance with previous reports. We chose the concentrations of landiolol in this study based on previous experiments using esmolol. Although these dosages showed some β-blocking activity (Table 1), they may not be sufficient to exert a cardioprotective effect in this experimental protocol. Thus, the difference in drug effects between this study and others may be due to the experimental protocol and species.
It is known that beta blockers, including landiolol, have direct effects on the myocardial membrane, antiperoxidative activity, antiradical actions, sarcoplasmic reticular function, and cardiac gene expression, independent of β-blocking activity. We previously found that pre-ischemic treatment with the nitric oxide donor nipradilol exhibits cardioprotection mainly due to the antioxidative effects of this agent. 4 In addition, the nonselective beta blocker propranolol inhibits the activity of reduced nicotinamide adenine dinucleotide oxidase, the effect of which is to slow mitochondrial respiration, thereby preserving adenosine triphosphate stores. 19 It is unclear to what extent the cardioprotective effect of landiolol is due to additional effects such as those with nipradilol and propranolol, and thus further investigation is needed.
Recent studies have advanced the development of potent cardioprotective agents as an alternative to IPC. As repeated short periods of ischemia are needed to accomplish IPC, it is not relevant to all patients with serious ischemic heart disease and complications of other organs. However, IPC activates several signaling pathways simultaneously, and consequently provides a greater cardioprotective effect than currently available pharmacological agents. In this context, clarifying the mechanism responsible for IPC will contribute to the development of the ideal cardioprotective agent for preconditioning. It was concluded from these results that infusion of landiolol in combination with IPC reduced LVEDP after ischemia-reperfusion, but did not significantly affect LVESP or infarct size. This suggests that landiolol enhanced the cardioprotective effect of IPC. The mechanism by which landiolol exerts these effects may be through selective regulation of adrenergic receptor-mediated signals in response to IPC.
Footnotes
Acknowledgments
We thank R. Clements, PhD, for helpful advice and editing of the manuscript. Landiolol was kindly provided by Ono Pharmaceutical Company, Osaka, Japan.