
Abstract
Between September 1989 and June 2004, 148 consecutive patients underwent ascending aortic replacement for aneurysm or dissection. There were 130 males (88%) and 18 females (12%). Their mean age was 46.20 ± 13.36 years. Fifty-seven patients (39%) were treated for type 1 and type 2 aortic dissection, and 91 (61%) for ascending aortic aneurysm. The Bentall procedure was performed in 81 patients (55%), the Cabrol procedure in 7 (5%), separate ascending aortic replacement and aortic valve replacement or repair was carried out in 24 (16%), and ascending aortic replacement only in 36 (24%). Hospital mortality was 4.05% (6 deaths). On univariate analysis, left ventricular ejection fraction ≤ 30%, emergency surgery, contained rupture, concomitant coronary artery bypass grafting, and age ≥ 65 years were risk factors for early mortality. However, on multivariate analysis, ejection fraction ≤ 30% and contained rupture were the only factors significantly associated with early mortality. The long-term survival rates were 87.2% ± 3.7% at 5 years, 78.0% ± 5.6% at 10 years, and 60.9% ± 9.9% at 15 years. Ascending aortic resection for aneurysm or dissection can be performed with low mortality and morbidity.
Introduction
Despite numerous advances over the last 35 years, aneurysms and dissections of the ascending aorta remain a major challenge for cardiac surgeons. Many pathological conditions that involve dilatation of the aorta with aortic regurgitation require replacement of the aortic valve and ascending aorta, either separately or as aortic root replacement with re-implantation of the coronary ostia into the graft. Since the first description of root replacement by Bentall and De Bono 1 in 1968, there have been many modifications of this technique, and other methods have evolved. 2,3 Several studies have reported favorable early results of various techniques with hospital mortality between 2% and 13%. 2,4,5 Recent advances in diagnosis and surgical techniques have significantly improved the early and late results. 4,6 We present our experience of ascending aortic replacement for aneurysm and dissection over the last 15 years.
Patients and Methods
Between September 1989 and June 2004, 148 patients underwent ascending aortic replacement for aneurysm or dissection. The data of all patients undergoing surgery for ascending aortic pathology was collected prospectively. The mean age of these patients was 46 ± 13 years (range, 11 to 82 years), and 130 (88%) were men. Preoperative characteristics are shown in Table 1. The causes of the aneurysms were determined by reviewing the clinical findings and pathologic examination of the aortic biopsy. In 60 patients (41%), the cause was myxomatous degeneration. Of the 57 (39%) patients with type 1 aortic dissection, 16 (28%) had acute dissection. Other etiopathological causes included post-stenotic dilatation of the ascending aorta in 20 patients (14%), atherosclerosis in 10 (7%), and pseudoaneurysm in one (1%). Surgical procedures are listed in Table 2. In patients with aortic aneurysm, a ratio of measured-to-expected size of the aorta above 1.5 was the indication for replacement of the aorta. In cases of Marfan syndrome and bicuspid aortic valve, a lower ratio was chosen as an indication for surgery, as reported by others. 7 Thirty-two (22%) patients had features of Marfan syndrome, non-Marfan myxomatous disorder was present in 28 (19%). The DeBakey classification of aortic dissection was used in this study. Prolonged ventilation was defined as ventilation > 48 hours. Renal dysfunction was defined as serum creatinine > 2.0 mg · dL−1 or if the patient required dialysis. Emergency surgery was surgery performed as soon as the diagnosis was made. Urgent surgery was that undertaken within 24 hours of admission. Smoking was defined as current or past regular cigarette use. Of 6 patients who had concomitant coronary artery bypass grafting (CABG), 4 were redo CABG cases. Associated hemiarch replacement was carried out in 2 patients, and mitral valve surgery in 5.
Characteristics of 148 Patients Undergoing Ascending Aortic Replacement
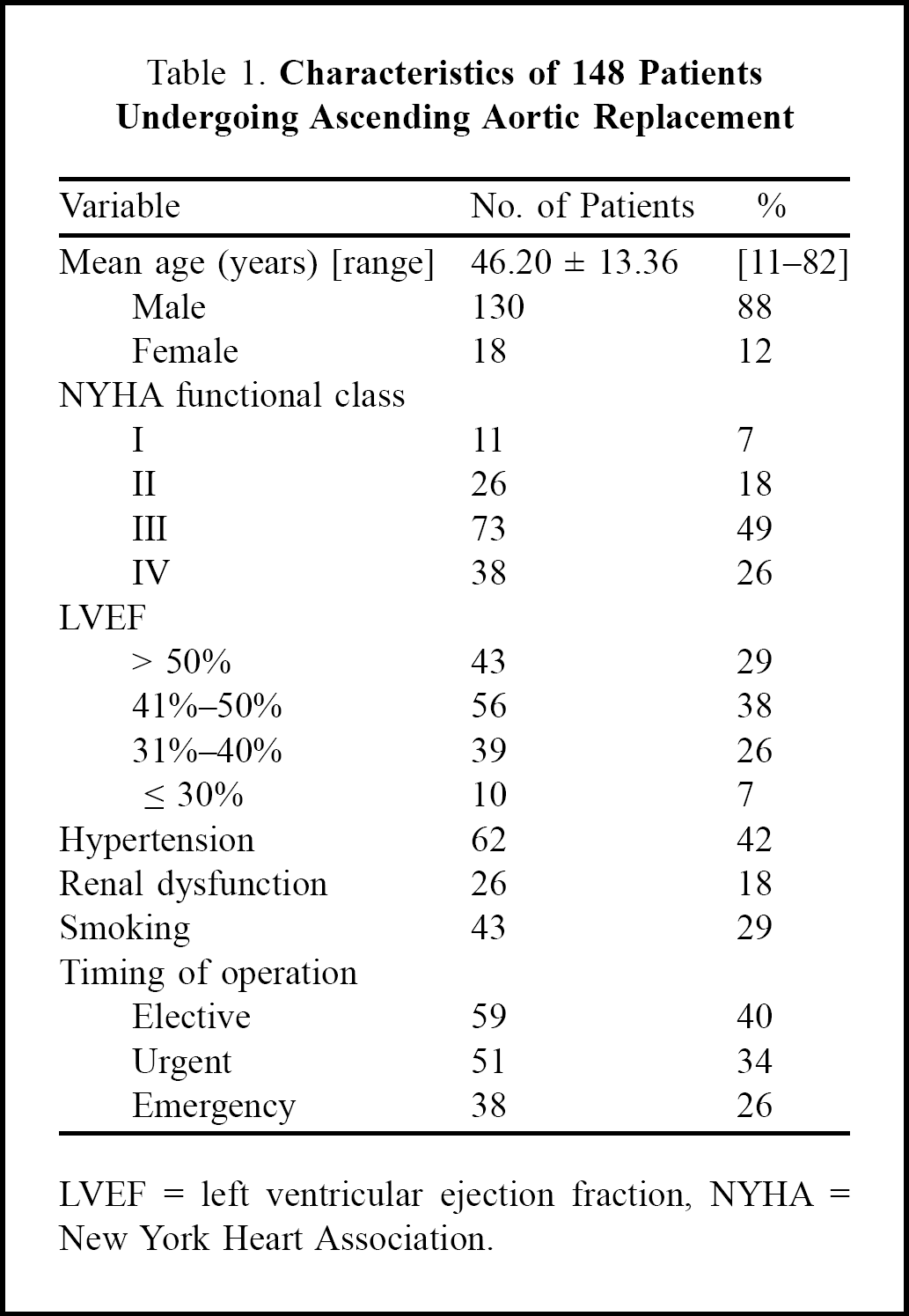
LVEF = left ventricular ejection fraction, NYHA = New York Heart Association.
Surgical Procedures in 148 Patients
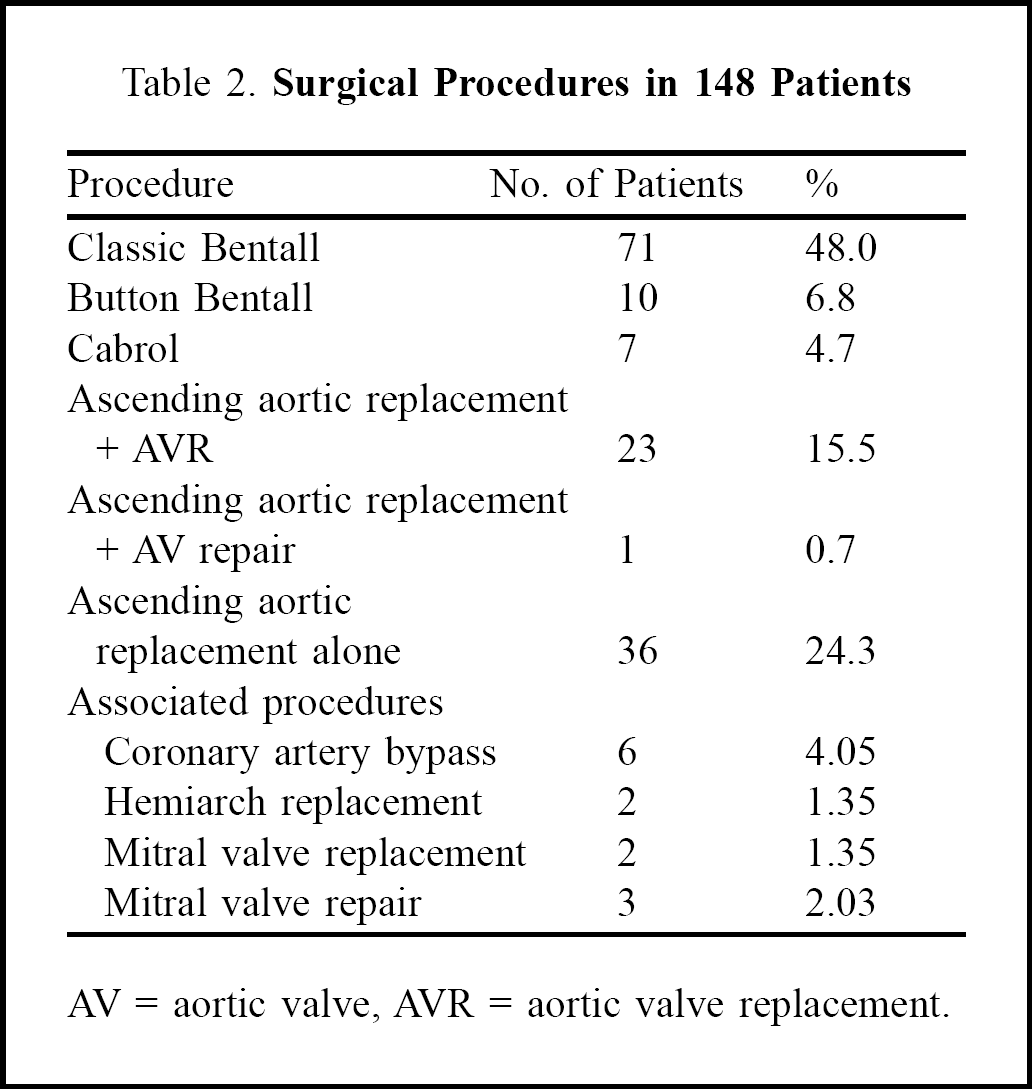
AV = aortic valve, AVR = aortic valve replacement.
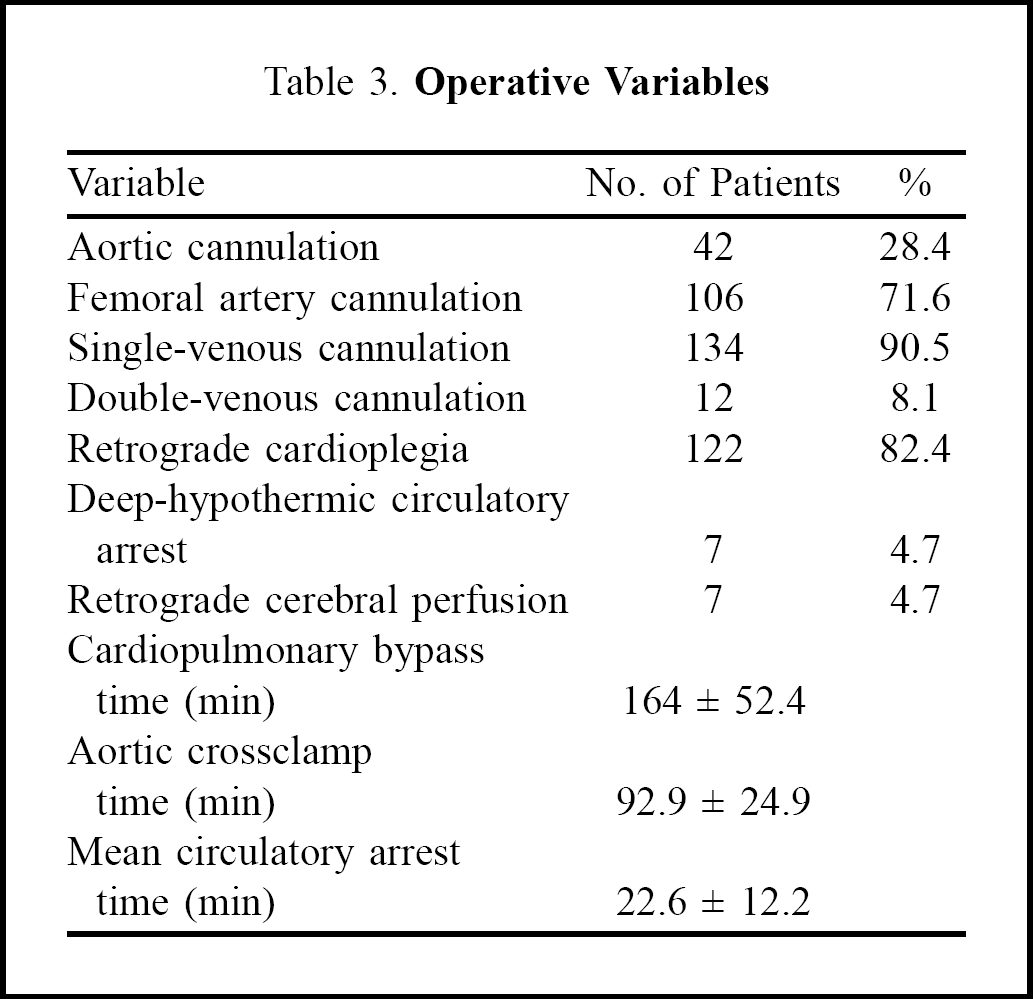
Aortic root replacement was performed by the classic or modified Bentall technique or by the Cabrol technique. 1 –3 Cardiopulmonary bypass was instituted with femoral-atrial or aortic-atrial cannulation. Bicaval-atrial cannulation was used in patients who required concomitant mitral valve surgery. In patients with dissection, arterial cannulation was always via the femoral artery. Moderate systemic hypothermia was used in those who had distal anastomosis during aortic crossclamping. Patients having open distal anastomosis were cooled to 16°C with deep-hypothermic circulatory arrest. Retrograde cerebral perfusion was used during hypothermic circulatory arrest. The left ventricle was vented through the right superior pulmonary vein in all cases. Myocardial protection was achieved with antegrade and retrograde cold blood cardioplegia. The operative variables are shown in Table 3. Direct coronary implantation was performed when the coronary ostia were lifted well above the annulus. When the coronary ostia were close to the annulus, they were mobilized as buttons and implanted into the graft. The Cabrol technique was applied in some early cases, using separate 6-mm conduits to implant the coronary ostia into the conduit. In cases of dissection, the conduit was cannulated after distal anastomosis, and cardiopulmonary bypass was re-instituted through this cannula. A composite graft with a Bjork-Shiley valve (Shiley, Inc., Irvine, CA, USA) was used in 17 (11%) patients, and a Carbomedics bileaflet valve (Carbomedics Inc, Austin, TX, USA) in 5 (3%) in the early period of the study. More recently, we used a composite Dacron graft with a St. Jude bileaflet valve (St. Jude Medical, Inc., St. Paul, MN, USA) in 89 (60%) patients. Gelatin-resorcinol-formaldehyde glue (GRF-glue; Fii, Saint-Just-Malmont, France) was used in 48 (84%) of the 57 patients with dissection to restore continuity between the separated layers of the aorta. The anastomosis was buttressed with Teflon strips to reinforce the fragile suture line. BioGlue, although expensive, is preferred by many surgeons because GRF glue can lead to adhesions and pseudoaneurysm formation. The patients were followed up at regular intervals in the outpatient clinic and by telephone contact. Follow-up ranged from 4 to 172 months, with a mean follow-up of 8.5 ± 2.6 years.
Operative Variables
Statistical analysis was carried out using SPSS version 10.0 software (SPSS, Inc., Chicago, IL, USA). The chi-squared test was used to calculate the probability value for the comparison of dichotomous variables. Fisher's exact test (2-sided) was used when the number in any cell was less than 5. Stepwise logistic regression was employed for multivariate analysis. The Kaplan-Meier survival curve was plotted. A p value < 0.05 was considered significant. Results are expressed as the mean ± standard deviation, except for estimated survival rates which are presented with the standard error.
Results
The overall hospital mortality was 4.05%. Causes of death were low cardiac output in 2 patients, multi-organ failure in 2, bleeding in 1, and stroke in 1. Two of the 91 patients with aneurysms died (2.20%), and 4 (7.02%) of the 57 patients with dissection died (p = 0.205). All 4 patients with dissection who died had acute dissection with low cardiac output preoperatively, requiring inotropics and ventilation, and they underwent emergency surgery. Two of them had diffuse coronary artery disease and required concomitant CABG; postoperatively, they had low cardiac output despite high-dose inotropic support, and died of myocardial failure. One 72-year-old man with dissection and a ruptured aneurysm required cardiopulmonary resuscitation and multiple blood transfusions when taken for emergency surgery. The aorta was very fragile, and he died of bleeding. Two patients died of multi-organ failure following septicemia. One patient was in a coma and did not recover. He had an atherosclerotic type 2 dissecting aneurysm. On univariate analysis, age ≥ 65 years, left ventricular ejection fraction ≤ 30, emergency surgery, concomitant CABG, and contained rupture were significantly associated with early death (Table 4). On multivariate logistic regression, ejection fraction ≤ 30% and contained rupture were the only factors associated with early mortality (Table 5).
Univariate Analysis of Preoperative and Operative Variables Associated with Hospital Mortality
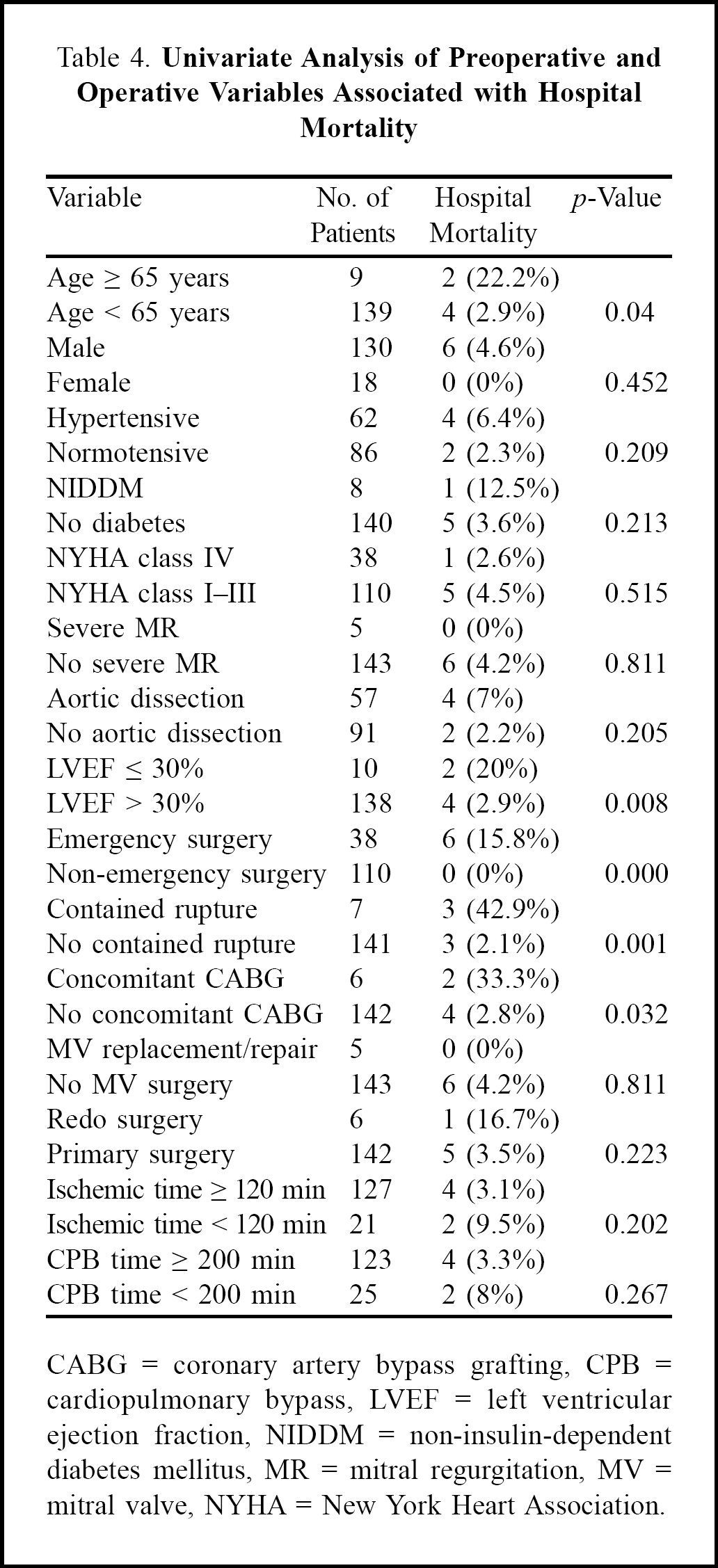
CABG = coronary artery bypass grafting, CPB = cardiopulmonary bypass, LVEF = left ventricular ejection fraction, NIDDM = non-insulin-dependent diabetes mellitus, MR = mitral regurgitation, MV = mitral valve, NYHA = New York Heart Association.
Multivariate Analysis of Factors Associated with Hospital Mortality
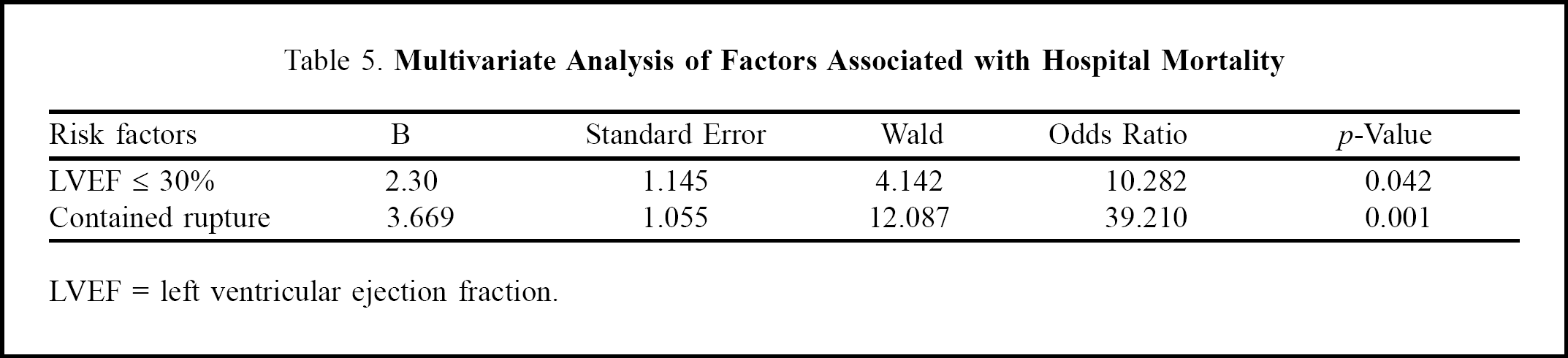
LVEF = left ventricular ejection fraction.
Postoperative morbidity is shown in Table 6. The 2 patients who had a transient neurological deficit recovered fully within a few hours. Of the 6 patients requiring prolonged ventilation, 2 needed a tracheostomy, and one had a mini-tracheostomy because he was unable to cough out secretions. Three patients developed renal dysfunction postoperatively, and one required dialysis; two others who required hemofiltration because of acute tubular necrosis made a full recovery. The median intensive care stay was 2 days (range, 1–4 days), and median hospital stay was 8 days (range, 6–15 days).
Postoperative Complications
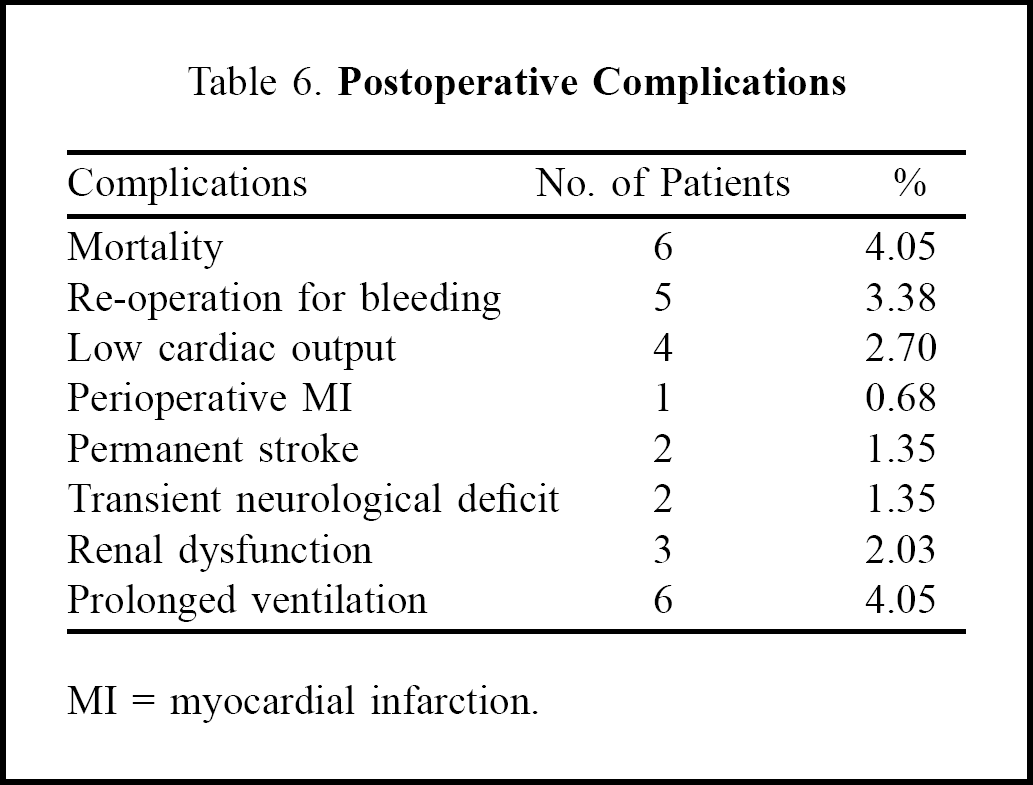
MI = myocardial infarction.
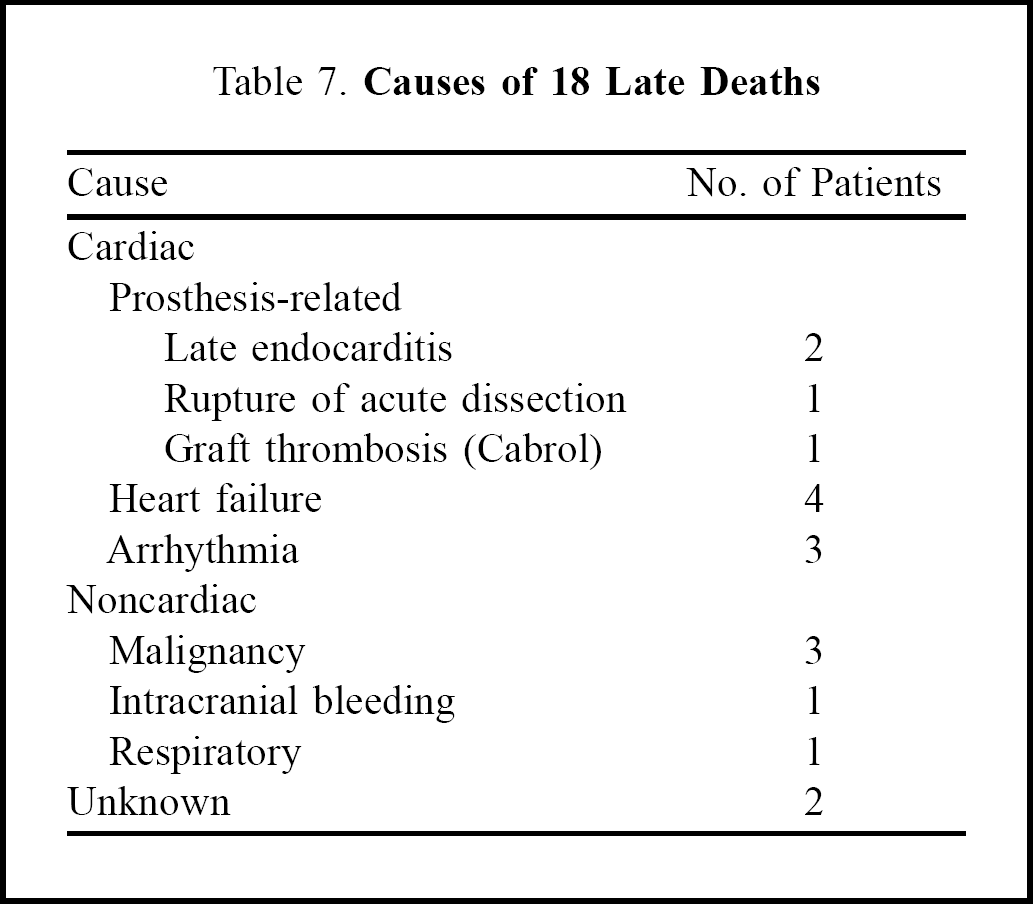
Of the 142 hospital survivors, 126 (89%) were followed up. The long-term survival rates were 87.2% ± 3.7% at 5 years, 78.0% ± 5.6% at 10 years, and 60.9% ± 9.9% at 15 years (Figure 1). Eighteen patients died during follow-up. The causes of late mortality are shown in Table 7. One patient who had a Cabrol procedure was re-admitted 2 years later with acute anterior wall myocardial infarction. On coronary angiography, the left limb of the graft (to the left ostium) was found to be occluded. He died before he could be taken up for surgery. Six patients had surgical re-interventions: 2 had aortic valve replacement, 3 underwent surgery for abdominal aortic aneurysm, and 1 developed pseudoaneurysm of the composite graft requiring a second graft replacement. Two patients who developed thoracoabdominal aortic aneurysm during follow-up refused surgery. One patient suffered thrombosis of a Bjork-Shiley valve and had thrombolytic therapy.
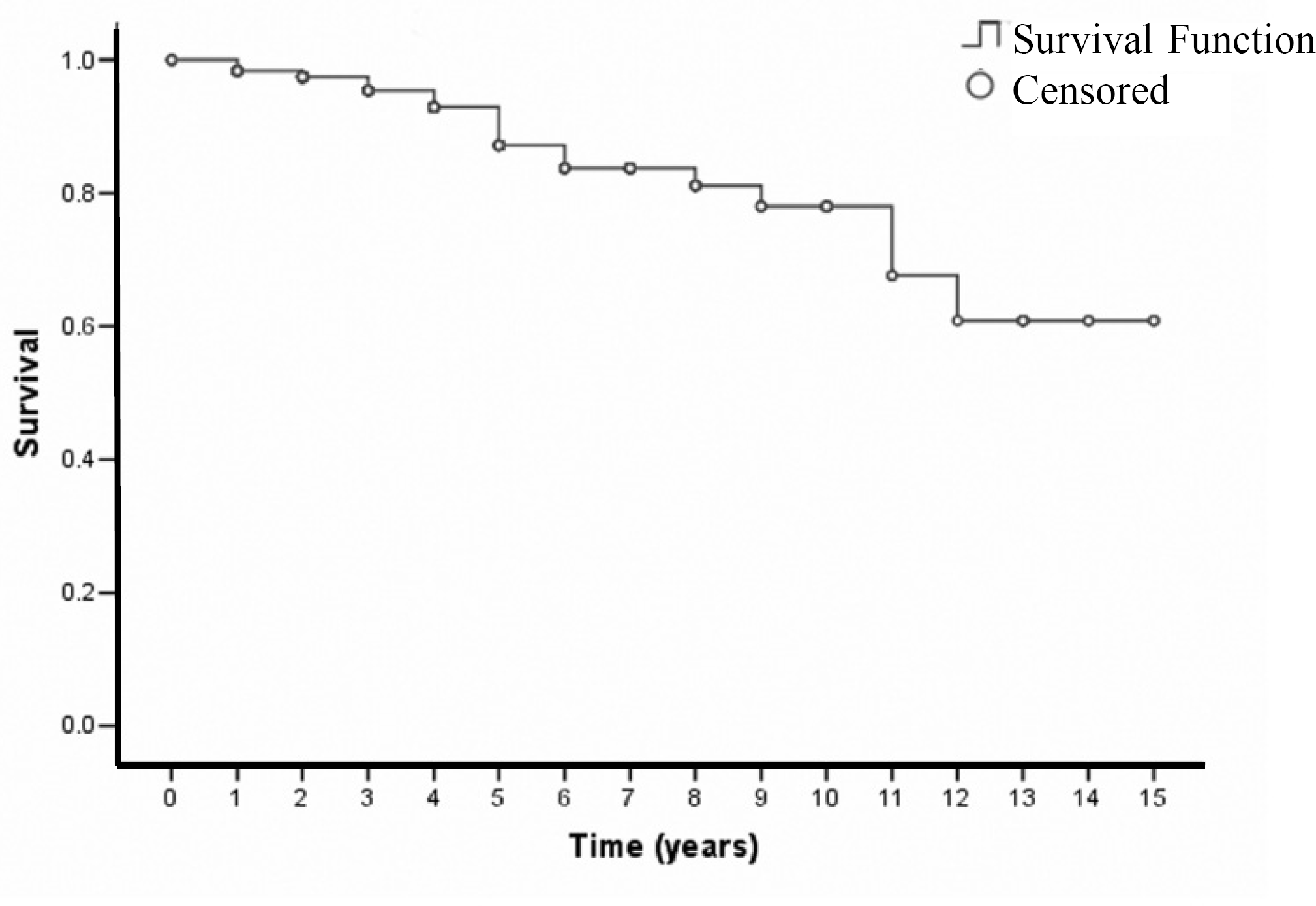
Kaplan-Meier survival curve (after discharge).
Causes of 18 Late Deaths
Discussion
Composite graft replacement of the aortic valve and ascending aorta, as originally described by Bentall and De Bono 1 or the modified button method, has become the accepted surgical treatment for a variety of proximal aortic conditions including ascending aortic aneurysm with aortic valve incompetence, aortic dissection, and infective endocarditis. 2 Various composite grafts can be used: cryopreserved aortic homografts, pulmonary autografts, stentless bioprostheses, and synthetic grafts. The currently available composite valved prostheses that have ultra-low porosity and ease of handling have greatly influenced the outcome in such patients.
In our study, the patients were relatively young (mean age, 46.20 ± 13.36 years) compared to other reports, and there was a male predominance (88%); others have reported a male-to-female ratio of 2:1 to 4:1. 6 The mortality of ascending aortic surgery varies from 2% to 13%. 2,6 Cohn and colleagues 6 noted the risk of mortality to be low, regardless of whether chronic ascending aortic dissection or aneurysm was present; however, acute aortic dissection poses a greater risk of early and late mortality. 4 Due to improved techniques, the surgical mortality rate for patients with acute type A dissections has been significantly reduced. 8,9 On the other hand, mortality in non-operated acute ascending aortic dissection is as high as 20% at 24 hours and 90% at 3 months. 10 In our study, the early mortality for ascending aortic aneurysm was 2.06%, while that for aortic dissection was 7.01%. Two of the 4 patients with dissection who died required preoperative cardiopulmonary resuscitation. Hata and colleagues 11 found preoperative cardiopulmonary resuscitation to be an important predictor of early mortality.
The type of surgery did not seem to influence early or late mortality, whether composite graft replacement or separate aortic valve replacement/repair and supracoronary replacement or only ascending aortic replacement. 6,12 However, separate replacement of the ascending aorta and aortic valve carries a higher complication rate for the remaining ascending aorta on long-term follow-up, compared with the Bentall procedure. 12 Ehrlich and colleagues 9 found concomitant procedures, hypothermic circulatory arrest time ≥ 30 min, and contained rupture to be risk factors for an adverse outcome. We found left ventricular ejection fraction ≤ 30% and contained rupture were the only factors associated with early mortality on multivariate logistic regression, but as the regression analysis was performed on a very small number of incidents, it should be interpreted as indicative. Bachet and colleagues 13 reported a 3% incidence of low cardiac output and 1.95% incidence of permanent stroke, which agree with our findings. The hospital morbidity in our study compares favorably with reports from other institutions. 4,14
Late survival has been reported to be approximately 80% at 5 years and 65% at 10 years. 13,15 Our long-term survival rates were higher at all time points (Figure 1). Degeneration of aortic valve substitutes, prosthetic valve endocarditis, vascular graft infection, and true or false aneurysm formation are late complications that can cause substantial mortality and morbidity. Hospital mortality for re-intervention on the ascending aorta and aortic root varies from 6% to 19%. 13 The estimated freedom from late re-operation for all patients was 84%, 67%, and 57% at 5, 10, and 15 years, respectively, with no significant differences among the subgroups of aortic dissection. 15 Gott and colleagues 4 found endocarditis to be the most common late complication. Another reported complication is false aneurysm, either from the aortic anastomosis or from the coronary artery button after a classic Bentall procedure, and its incidence varies from 7% to 25%. 16 Dossche and colleagues 5 did not find any significant difference in the incidence of pseudoaneurysm between the inclusion/wrap and open technique. On the other hand, Grey and colleagues 17 noted that wrapping was associated with a high risk of false aneurysm or graft tamponade. Similarly, a fistula between the wrapped ascending aorta and the right atrial appendage offers no advantage, and may even be deleterious. 3 Bachet and colleagues 13 found persisting left-to-right shunts in 4 of 11 patients, 2 of whom had to be re-operated on to close the shunt. The incidence of thromboembolism is reported to be 0.42% per 100 patient-years. 16 We had only one case of valve thrombosis in a Bjork-Shiley valved conduit.
Open distal anastomosis is widely used, especially in cases of severe atherosclerotic disease of the aorta. 9 Aortic clamping can produce dissection of the aorta beyond the anastomosis. As intimal disease in the aorta can be subtle and difficult to determine even on transesophageal echocardiography or epiaortic ultrasound, open distal anastomosis is a versatile option in cases of severe aortic disease. We applied a soft aortic crossclamp to perform the distal anastomosis in most of our patients, because the aorta was not atherosclerotic (due to the relatively young patient population), thus avoiding hypothermic circulatory arrest that has its own morbidity. Open distal anastomosis was performed in 5 (3%) patients because the distal aorta was atheromatous. When the aortic valve needs replacing and the coronary ostia are significantly displaced, the classic Bentall operation is widely performed with good early and long-term results, although reservations have been expressed as the coronary anastomosis is under tension and may result in pseudoaneurysm later. Hence, some surgeons routinely perform the coronary button re-implantation technique. 6 The button technique is used when the coronary ostia need to be mobilized. The Cabrol technique is not commonly used because of its associated complications of kinking and thrombosis of the limbs of the graft, but it is sometimes employed in redo procedures. A mixed technique has also been used, in which a Bentall type of anastomosis of the left ostium and saphenous vein grafting of the right coronary artery are carried out. 13 When there is no coronary displacement, a more conservative approach is preferred, such as separate valve repair or replacement and a supracoronary graft. When aortic regurgitation is mild, without sinus enlargement, the aneurysm can be resected and the graft down-sized and sculptured accordingly, as suggested by David and colleagues. 14
Transesophageal echocardiography was used in all our patients to study the pathology and extent of the aneurysm, and to differentiate between aortic dissection, penetrating aortic ulcers and intramural hematoma, as their natural histories are different, and recognition and localization are critical determinants of therapy. 18 Computed tomography and magnetic resonance imaging were used when the condition of the patient was stable. Coronary angiography was used in stable patients with ascending aortic aneurysm and chronic dissection who were aged over 40 years (64 patients; 43%). Creswell and colleagues 19 recommend coronary arteriography for all patients with acute type A dissection in a stable condition, and all patients with chronic type A dissection. They found coronary artery disease in 34.8% of patients with acute dissection and 42.9% of patients with chronic aortic dissection, while others observed the incidence of concomitant coronary artery disease in ascending aortic aneurysms to be 5% to 16%. 20
Due to advances in diagnostic, anesthetic, and surgical techniques, perfusion technology, perioperative and postoperative management, and closer postoperative surveillance, the surgical outcome for ascending aortic aneurysms and dissections has markedly improved. However, earlier diagnosis of acute aortic dissection before the development of cardiac tamponade and renal or visceral flow impairment is essential to improve survival even further.
Footnotes
Acknowledgment
We thank Mr. Sudhir Shekhawat for providing assistance in statistical analysis.