
Abstract
In deciding the surgical treatment for lung cancer, it is important to differentiate between a small satellite lesion that is probably benign, a pulmonary metastatic lesion, or a double cancer. The operative indications for lung cancer with small satellite lesions detected on preoperative helical computed tomography were retrospectively examined. We collected 43 small nodules ≤1 cm in diameter from 32 patients. A definitive diagnosis was made by follow-up computed tomography in 3 of 19 ipsilateral lesions and in 9 of 24 contralateral lesions. The final diagnosis of the satellite lesions was malignant in 13 and benign in 30. The 13 malignant lesions consisted of 2 pulmonary metastases and 11 double cancers. Two patients with stage IIb and IIIb disease on clinical staging of the main tumor had pulmonary metastases. Patients with clinical stage I disease had a higher probability that the small lesions were benign or double cancers than those with advanced disease beyond clinical stage I.
Introduction
Many studies have demonstrated the superiority of helical computed tomography (CT) in the detection of pulmonary nodules, identifying a greater number of nodules than conventional CT. 1 With the increasing application of helical CT, small pulmonary nodules ≤1 cm in diameter have been more frequently detected. 2,3 We have often encountered small satellite lesions on CT before surgery for non-small cell lung cancer (NSCLC). In deciding the surgical treatment, it is important to determine the probability that the small satellite lesion is benign, a pulmonary metastatic lesion, or synchronous multiple primary lung cancers (MPLC). 4 However, it is difficult to make a definitive diagnosis of the lesion preoperatively because of its small size. 1 –4 We retrospectively examined the operative indications for NSCLC with small satellite lesions detected on preoperative helical chest CT.
Patients and Methods
The data of patients who underwent surgery for NSCLC in our department from April 1999 to March 2003 were retrospectively collected. Thirty-two patients had 43 small satellite lesions ≤1 cm in diameter, which were detected on preoperative helical chest CT. There were 24 men and 8 women. The mean age was 69 ± 8 years. None of the patients received perioperative radiotherapy or chemotherapy. All chest examinations were performed using a Somaton Plus 4 scanner (Siemens, Erlagen, Germany). Helical scanning was carried out with a slice thickness of 2 mm, a table speed of 3 mm·sec−1, and an image reconstruction interval of 5 mm. Patients with clearly benign lesions (e.g., calcified nodules) were excluded from this study. Also, patients with ground-glass opacity lesions were excluded because most ground-glass lesions are early bronchioloalveolar carcinoma, and lung cancer with a satellite ground-glass lesion might be MPLC. 5 The radiologic findings were assessed by two chest radiologists. In addition to chest CT, all patients underwent CT of the upper abdomen, magnetic resonance imaging of the brain, and whole body bone scanning to rule out systemic metastasis. Positron-emission tomography (PET) using 18F-fluorodeoxyglucose was performed in 8 patients from August 2002. Postoperative follow-up CT for indeterminate lesions was undertaken every 4 to 6 months for over 2 years. Stability in the size of a pulmonary nodule seen on chest radiographs over 2 years has generally been accepted as an indicator of benignity. 4 Thus, in follow-up CT, we defined disappearing lesions as inflammation, those unchanged for over 2 years as benign, and enlarging lesions as malignant. MPLC were defined according to Martini and Melamed. 6
Categorical data were analyzed with the chi-squared test. Survival time for patients with MPLC was calculated from the date of the first operation to the date of the last follow-up or death. Cumulative survival was determined by the Kaplan-Meier method. A probability value less than 0.05 was accepted as statistically significant. Statistical analysis was performed using Stat-View 5.0 software (SAS, Inc., Cary, NC, USA).
Results
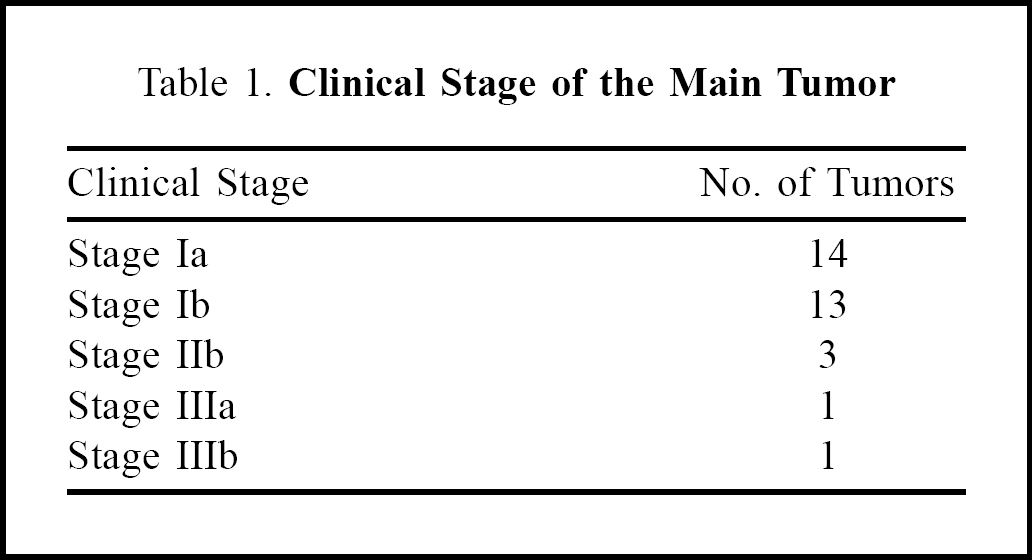
The clinical stages of the main tumors are given in Table 1. There were 21 lesions ≤5 mm in diameter, 22 were 6–10 mm, and 3 were > 10 mm. Six lesions ≤5 mm in diameter were malignant (29%). Five lesions of 6–10 mm were malignant (23%). There were no significant differences in malignancy rates between the two groups. Definitive diagnoses of lesions ipsilateral to the main tumor were made by histological examination in 16 cases and by follow-up CT in 3 (Figure 1). Among these 16 lesions, histology showed 15 were benign and 1 was a pulmonary metastasis. Follow-up CT showed that 2 of the 3 lesions were benign and 1 was MPLC. Definitive diagnoses of lesions contralateral to the main tumor were made by histological examination in 15 cases and by follow-up CT in 9 (Figure 1). We performed video-assisted thoracoscopic surgery (VATS) for histological diagnosis in contralateral lesions located peripherally. Among the 15 contralateral lesions, the histological diagnosis was made by VATS in 6 cases, and by re-operation in 9 that were enlarged on follow-up CT. Among the 6 lesions diagnosed histologically by VATS, 1 was a pulmonary metastasis and 5 were benign. Follow-up CT showed that of 18 contralateral indeterminate nodules after surgery, 8 were benign and 10 were MPLC (Figure 1). Nine of the 10 MPLC lesions were diagnosed histologically after re-operation.
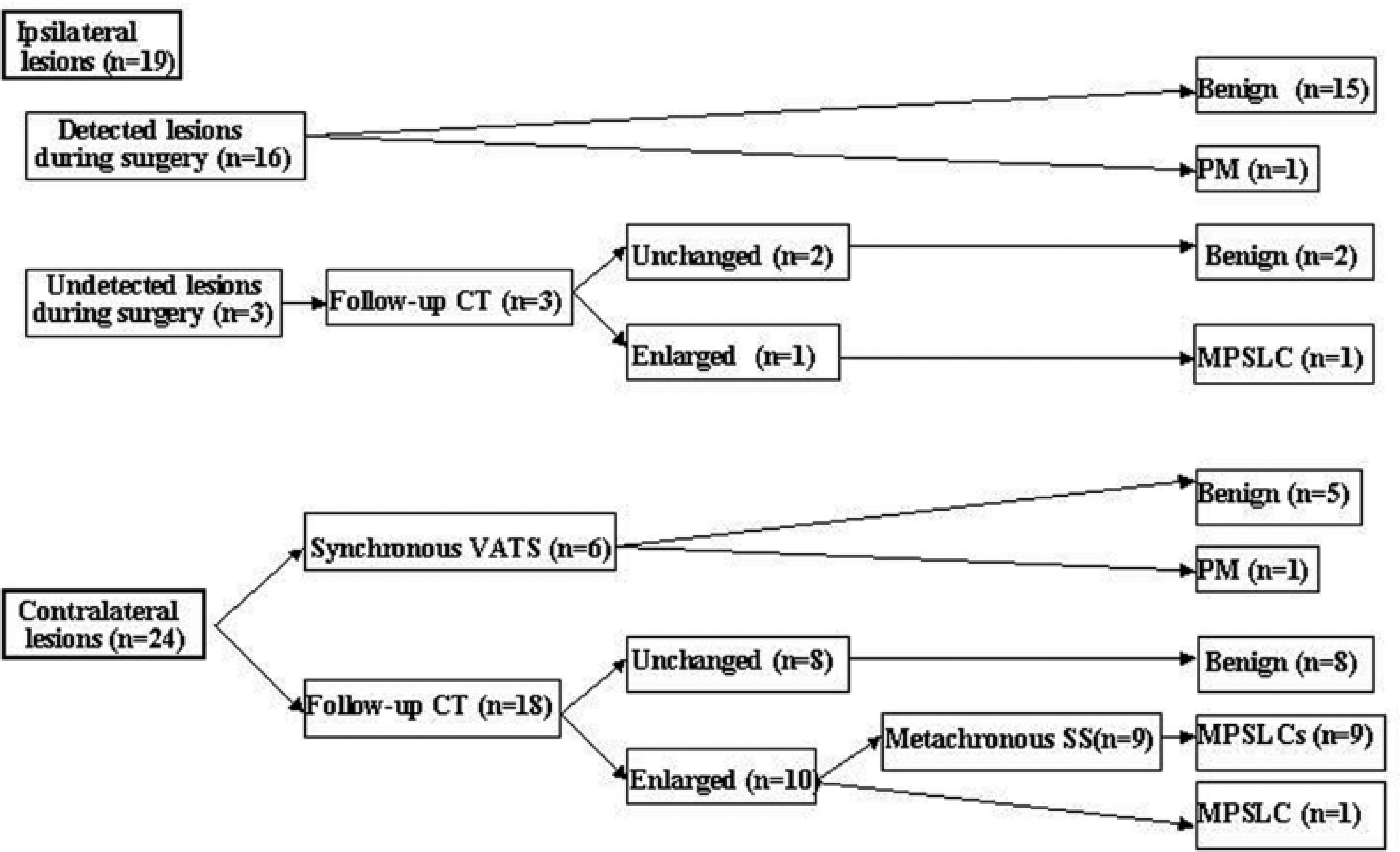
Flow sheet of diagnosis. Metachronous SS = metachronous second surgery, MPLC = multiple primary lung cancer, PM = pulmonary metastasis, VATS = video-assisted thoracoscopic surgery.
Clinical Stage of the Main Tumor
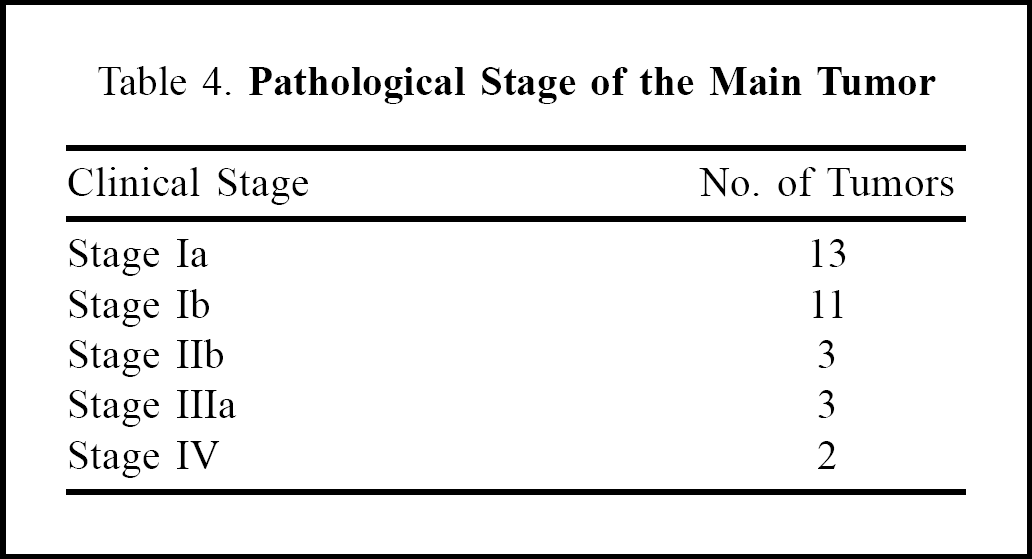
The definitive diagnosis of satellite lesions was malignant in 13 cases and benign in 30 (Table 2). Patients with clinical stage I disease had a higher probability that the small lesions were benign or MPLC than those with advanced disease beyond clinical stage I (p = 0.01). Of the 13 malignant lesions, 2 were located in the ipsilateral lung and 11 in the contralateral lung. The 30 benign lesions are listed in Table 3. Of these, 17 were located in the ipsilateral lung and 13 in the contralateral lung. Pathological stages of the main tumors are given in Table 4. Positron-emission tomography was performed in 8 patients, including 3 with MPLC. There was one patient with a lesion of 5 mm and two with lesions of 8 mm. Positron-emission tomography was negative in all the MPLC lesions. A second lung resection for MPLC was performed in 8 patients who had a stage I or II main tumor. Five-year survival from the date of the first operation was 83%. There was no significant difference in 5-year survival rates between MPLC and non-MPLC patients in pathological stage I and stage II (Figure 2).
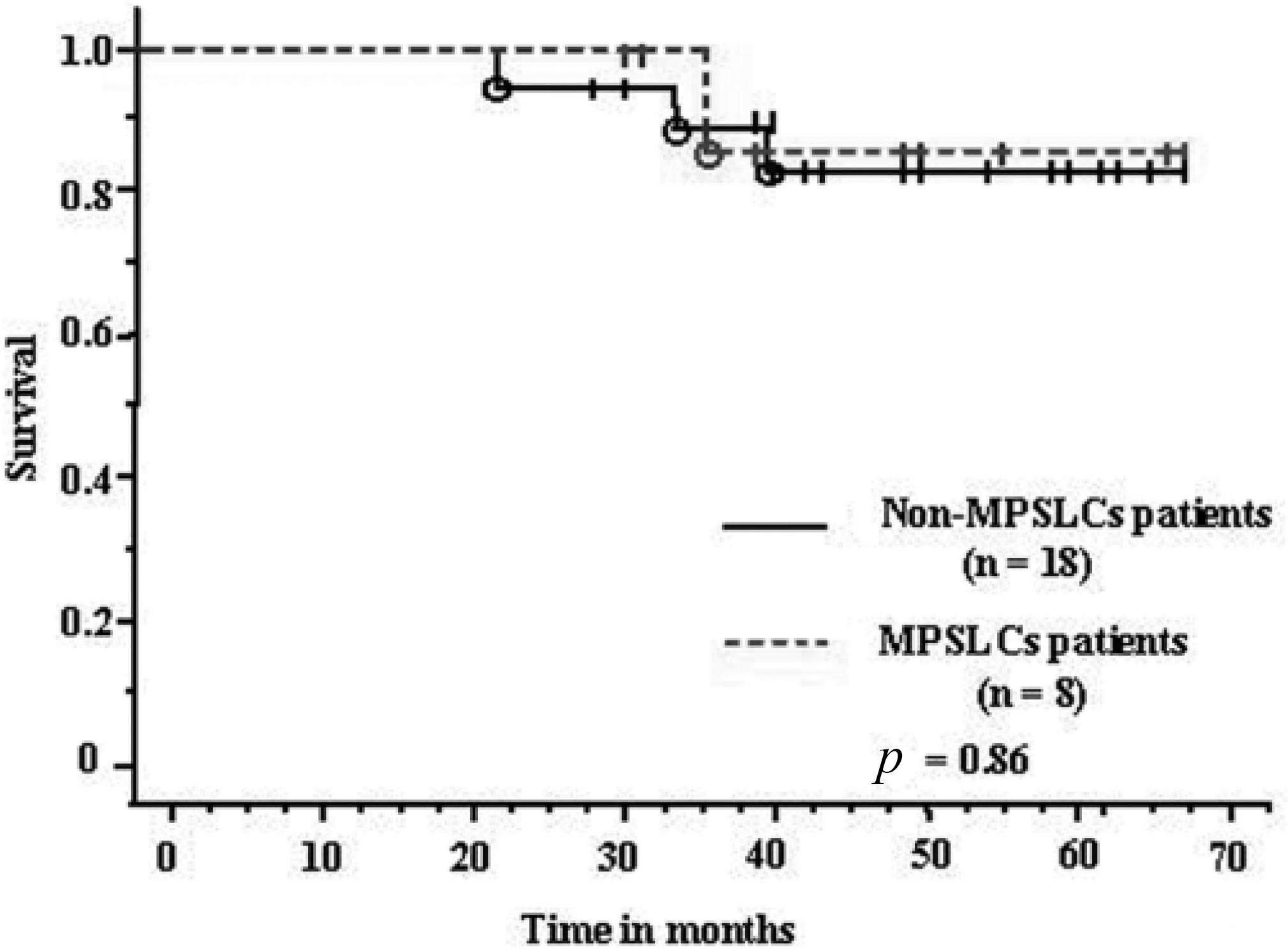
Cumulative survival curves of MPLC and non-MPLC patients in pathological stage I and stage II. There was no significant difference in 5-year survival rates between MPLC and non-MPLC patients. MPLC = multiple primary lung cancer.
Definitive Diagnosis of Satellite Lesions and Clinical Stage of the Main Tumor
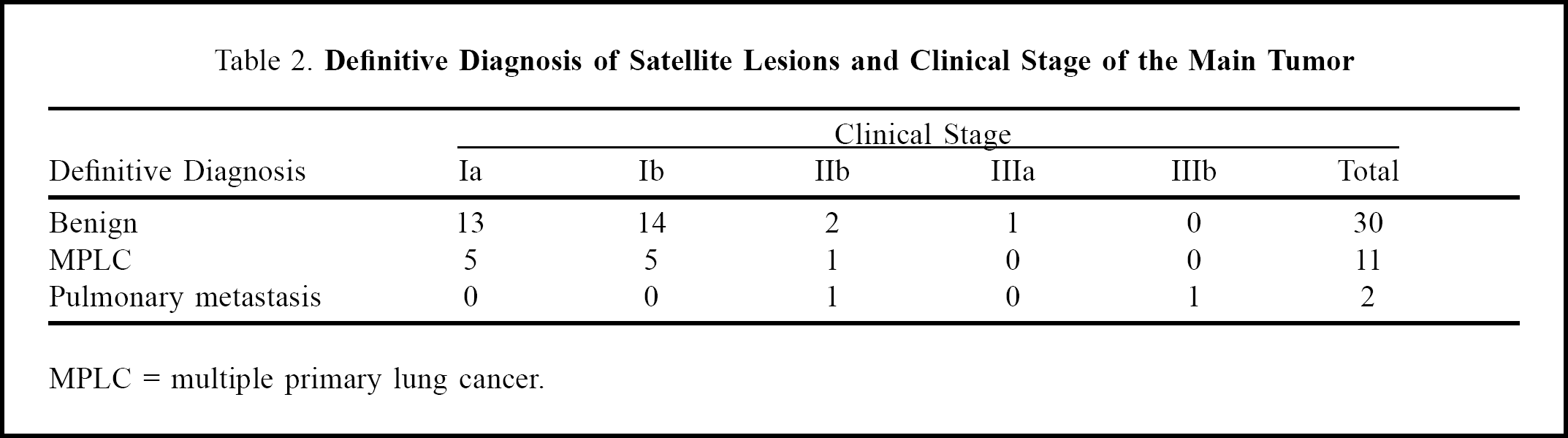
MPLC = multiple primary lung cancer.
Final Diagnosis of Satellite Lesions
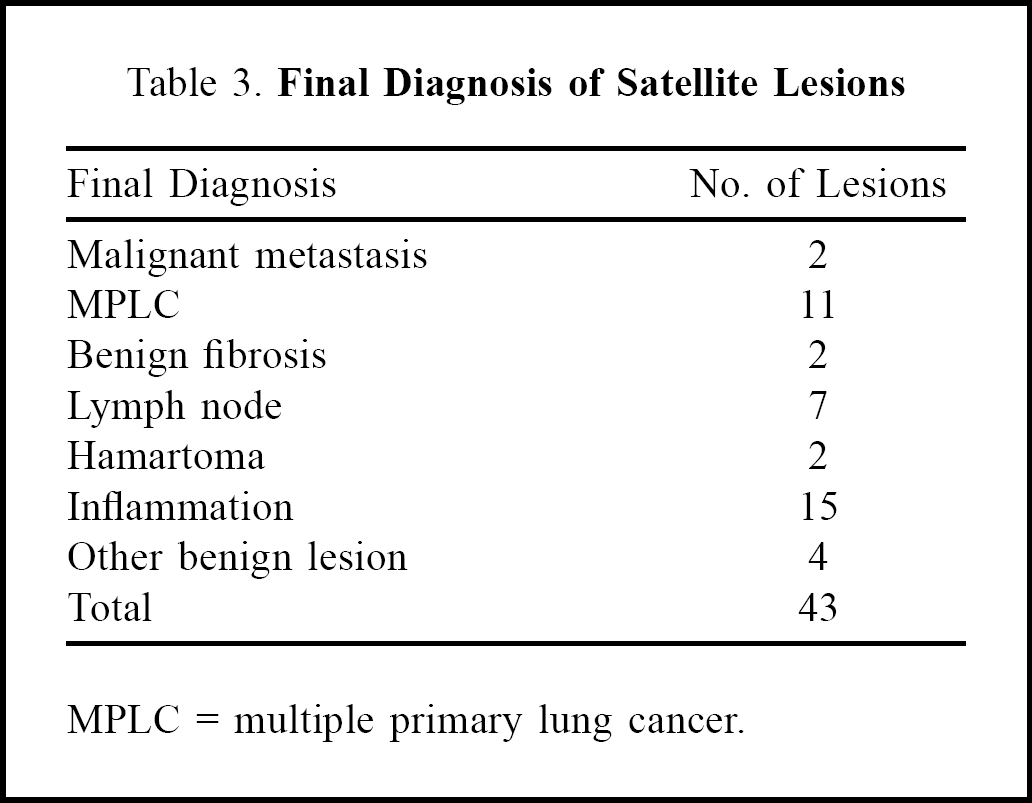
MPLC = multiple primary lung cancer.
Pathological Stage of the Main Tumor
Discussion
Since we introduced helical CT in 1998, we have more frequently found small satellite lesions on preoperative CT for NSCLC. We could not make a definitive diagnosis of the lesions before surgery, nor for most of the lesions after surgery. Thus, we performed follow-up CT for indeterminate nodules every 4 to 6 months postoperatively. Munden and colleagues 2 demonstrated in 64 patients with 65 small pulmonary lesions ≤1 cm in diameter detected by helical CT, that 58% were malignant. They reported that 37 (58%) patients had no previously known malignancy, while 27 (42%) had a previous malignancy. In those with a previous malignancy, a malignant lesion was diagnosed in 81% (22/27). This included 7 (26%) patients with bronchogenic carcinoma as a second primary carcinoma. Ginsberg and colleagues 3 reported that in patients with known malignancy, nodules smaller than 0.5 cm were more likely to be benign, whereas those over 0.5 cm but smaller than 1 cm were more likely to be malignant. Keogan and colleagues 4 noted that in patients with otherwise operable lung cancer, over 70% of noncalcified pulmonary nodules detected on conventional CT were benign. Positron-emission tomography is an accurate noninvasive test for diagnosis of pulmonary nodules and larger mass lesions, but few data exit for nodules < 1 cm in diameter. 7 As the spatial resolution of the current generation of PET scanners is 7 to 8 mm, use of PET for smaller nodules should await further technological refinements. In our series, PET was negative for all 3 MPLC lesions ≤8 mm in diameter. Thus, PET might not be useful for definitive diagnosis of lesions ≤1 cm in diameter.
In our series using helical CT in the staging of NSCLC, patients with clinical stage I disease had a higher probability that the small lesions were benign or MPLC than those with advanced disease beyond stage I (p = 0.01). Carretta and colleagues 8 also demonstrated that patients with nodules ≤5 mm in size, or with clinical stage I and II tumors, had a higher probability of benign lesions, although their data did not reach statistical significance. Different criteria for MPLC have been proposed. 6,9,10 We adopted the criteria of Martini and Melamed. 6 We performed a second lung resection for MPLC in 8 patients who had stage I or II on pathological staging of the main tumor. As their 5-year survival rate was 83% and the prognosis of MPLC is excellent, the small lesions in these 8 patients might not be intrapulmonary metastases but MPLC, and the criteria of Martini and Melamed 6 might be correct for such lesions.
The incidence of MPLC has been reported to vary from 1% for synchronous to 10% for metachronous lung cancers. 6,9,11 –16 Clinically, it is difficult to distinguish between MPLC and pulmonary metastases. The criteria of Martini and Melamed 6 have been adopted by most authors. 8,11 –14,16 Patients with MPLC have a relatively poor 5-year actuarial survival rate of 18% to 38%. 6,9,11 –13,15,16 In particular, patients with synchronous cancer have a poorer 5-year actuarial survival rate of 0% to 28% than those with metachronous cancer (11% to 44%). 6,9,11 –13,15,16 However, the postoperative survival rate of synchronous lung cancer still remains higher than that of recurrent disease. Recently, Okada and colleagues 10 reported that 5-year (from initial operation) actuarial survival rates of synchronous and metachronous lung cancer were 70.3% and 66.0%, respectively. Their patients with synchronous lung cancer had an excellent survival rate compared with other studies. 6,9,11 –13,15,16 They suggested that such patients would have a survival advantage because the possibility that some with recurrent or metastatic disease had been included in other reports could not be ruled out. In our study, patients with MPLC had an excellent 5-year survival rate of 83%, although this was only in the 8 patients with stage I or II on pathological staging of the main tumor. Most of the previous reports on MPLC in the 1980s did not employ CT for detection of MPLC. 11,14 Thus, the routine use of helical CT for NSCLC with small lesions before and after surgery, and careful follow-up of the lesions might aid early detection and treatment of MPLC, and thereby improve survival.
In reality, it is impossible to accurately differentiate between MPLC and pulmonary metastases preoperatively because accurate diagnosis relies on histological or molecular biological findings. 9 Therefore, Battafarano and colleagues 17 examined the impact of completely resected multifocal NSCLC on patient survival. They reported that node-negative patients with multifocal NSCLC had a favorable 3-year actuarial survival rate. Node-negative T1–T2 patients with multifocal NSCLC in the same lobe and/or a different lobe had 3-year survival rates of 66.5% and 63.6%, respectively. Tung and colleagues 18 found that node-negative patients with multifocal NSCLC of the same histological type in an ipsilateral different lobe had an excellent 5-year survival rate of 66.7%. Okada and colleagues 19 reported that node-negative patients with ipsilateral pulmonary metastases had an excellent 5-year survival rate of 45%.
This study demonstrated that if NSCLC patients with small satellite lesions detected on preoperative helical CT had stage I disease on clinical staging of the main tumor, the small lesions might be benign or MPLC, and those with MPLC had an excellent prognosis.