
Abstract
A 67-year-old man presented with hemoptysis following 2 previous operations on the descending thoracic aorta. Preoperative investigations and surgical exploration failed to demonstrate an aortobronchial fistula. It was subsequently detected at autopsy after the patient succumbed to a massive bout of hemoptysis.
Introduction
An aortobronchial fistula is a connection between the aorta and the airways. It is a rare cause of hemoptysis and is uniformly fatal in untreated cases. 1 It occurs most often after surgery (75%), especially after procedures on the descending thoracic aorta. 1 Aortobronchial fistula should be suspected in a patient presenting with recurrent hemoptysis, with either radiographic evidence or previous surgical repair of a thoracic aneurysm. 1 However, diagnosis before death is made in only 50% of cases. 1,2
Case Study
A 67-year-old man presented with a 3-month history of recurrent low-grade hemoptysis. He had undergone resection of an aneurysm of the descending thoracic aorta and replacement with a Dacron graft. Further aneurysmal dilatation necessitated replacement of his entire supradiaphragmatic descending thoracic aorta with a Dacron conduit 22 years later. An aortobronchial fistula was suspected, but investigation by aortography, pulmonary angiography, computed tomography (CT) and bronchoscopy failed to reveal any communication. He was readmitted 8 months later due to hemoptysis and collapse. Bronchoscopy showed a clot in the apical segment bronchus of the left upper lobe. A CT scan of his chest revealed no pseudoaneurysm or secondary lung changes. An aortogram failed to demonstrate an aortobronchial fistula. A magnetic resonance angiogram (MRA) suggested a pseudoaneurysm at the site of the proximal aorta-conduit anastomosis (Figure 1).
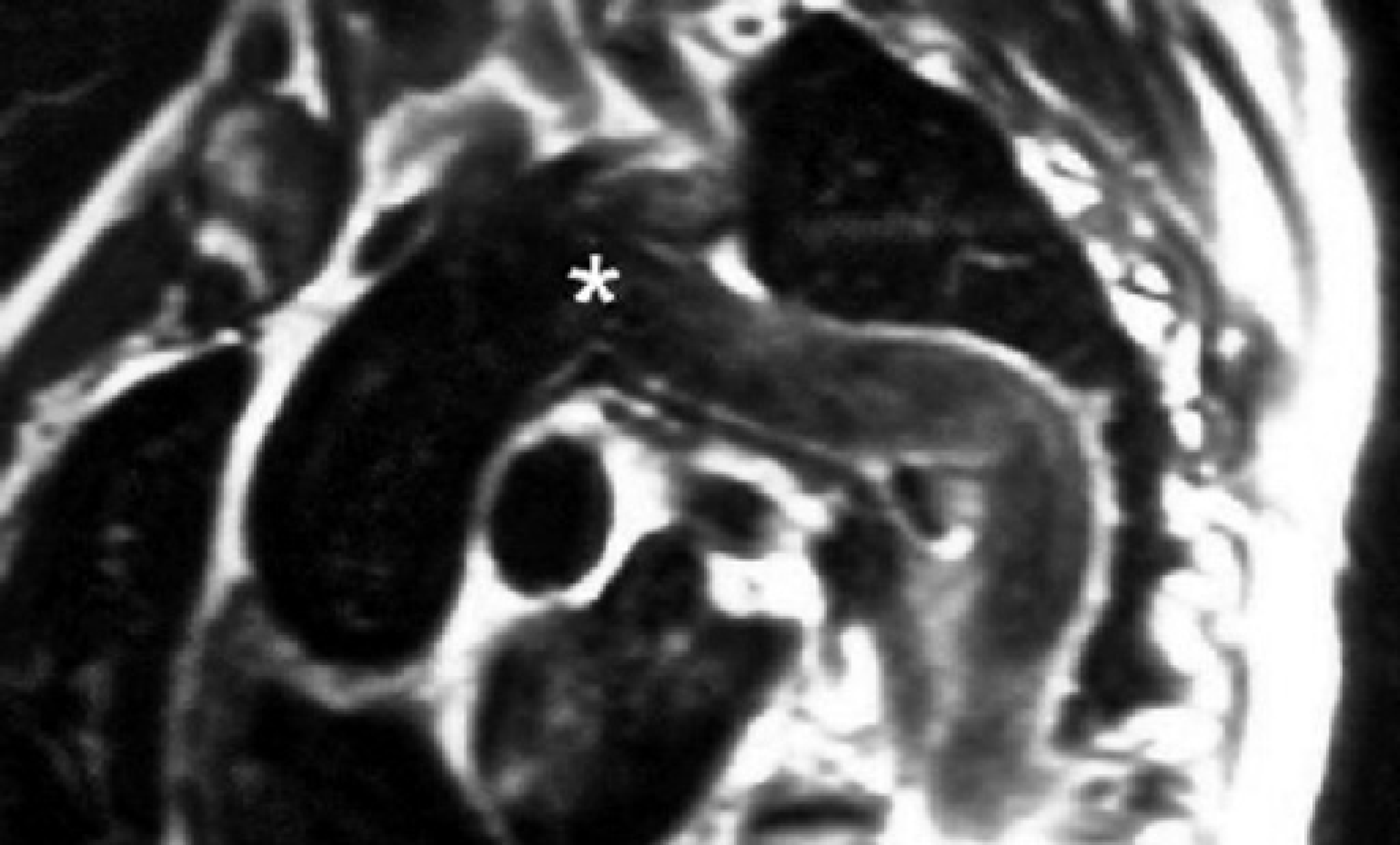
Magnetic resonance angiography: The asterisk (
In view of the two previous thoracotomies, it was decided to approach the aortic arch through a median sternotomy. The proximal anastomosis was examined and found to be pristine. The left lung was densely adherent to the rest of the graft, and the graft could not be mobilized. Under deep-hypothermic circulatory arrest, the aortic arch was incised and the graft examined from within. No obvious communication was apparent. In view of the greatly increased technical hazard of replacing the graft a third time, it was decided to reinforce the proximal suture line of the graft-aortic anastomosis with pledgetted sutures. The patient's recovery was complicated by seizures and a methicillin-resistant Staphylococcus aureus infection of his sternum. One month after surgery, he succumbed to a massive bout of hemoptysis. At autopsy, the left lung was found to be densely adherent to the circumference of the graft. The graft was opened along its entire length. Careful examination revealed a pinhole communication between the graft lumen and a subsegmental bronchus from the apical segment of the left upper lobe.
Discussion
The incidence of aortobronchial fistula is low. A review up to October 2002 reported 79 fistulas in 76 patients. 3 A pseudoaneurysm often precedes the development of post-surgical aortobronchial fistula. 3 As with true aneurysms, the pseudoaneurysm progressively enlarges and causes pulsatile erosion of the adjacent lung (usually the left). 3 Hemoptysis, typically intermittent, is the most common presenting symptom and occurs in over 95% of cases. 4,5 Other symptoms include chest pain, cough, and dyspnea. 5 Chest radiography may show nonspecific parenchymal consolidation related to hemorrhage or a new enlarging mass. 2 Fibre-optic bronchoscopy may identify the site of bleeding and occasionally the fistula itself. However, fatal hemoptysis after removal of the clot has been described. Angiograms often show an aneurysm (78%) but only occasionally demonstrate a fistula (17%). 2 Conventional chest CT can reveal both the aortic pathology and secondary changes in the adjacent lung. 1 In the presence of hemoptysis, these findings are virtually diagnostic of an aortobronchial fistula. 6 Demonstration of a fistula by CT is very rare. 3 Recently, MRA and CT angiography have proved to be more precise noninvasive techniques for diagnosis and follow-up of aortic pathology. 6
Even successful surgery for aortobronchial fistula carries considerable mortality and morbidity. 3 Surgical treatment consists of repair of both the aortic and pulmonary defects. The aortic side is managed by patch closure, direct suture, or a prosthetic graft. When a previously placed vascular prosthesis is present, it should ideally be replaced. 2 The bronchial side is managed by lung resection or simple closure. 2 New graft and suture lines should be protected by interposing viable tissue such as pleural or pericardial flaps, omentum or muscle. 2 Patients unsuitable for conventional surgical repair may undergo endovascular stent-graft exclusion of the fistula. 7 Although experience is limited, no mortality has been reported with this procedure. 3 In our case, repeated investigations failed to demonstrate a fistulous connection between the aorta and the lung. Surgical exploration was decided on the basis of the history and an MRA suggestive of a pseudoaneurysm at the level of the proximal anastomosis. In view of the 2 previous operations and our operative findings, it was felt that a further surgical procedure posed unacceptable risks. Stent-grafting was a possible primary option despite the lack of evidence of a fistulous connection and the unknown long-term outcome. However, MRA findings suggested a pseudoaneurysm at the site of the proximal anastomosis at the level of the left subclavian artery, which can be difficult to exclude with a stent-graft. Another option may have been stent-graft implantation in the early postoperative period. Although previously never described, this may have precluded the fatal hemoptysis.
In conclusion, post-surgical aortobronchial fistula is a rare and challenging entity and modifications of technique may be necessary to achieve a successful outcome.