
Abstract
Re-fixation of the sternum after sternal dehiscence is still a problem following cardiac surgery. An original technique that allows reinforcement against various causes of dehiscence is described. The technique consists of 3 additional overlapping longitudinal wires set on both sides of the sternum. Over 2 years, this technique was applied in 34 patients, with complete sternal re-fixation in all, and no signs of recurrence on follow-up.
Introduction
Despite the proposal of several techniques, re-fixation of the sternum after failure of the primary closure still represents a surgical dilemma. 1 –8 A variety of different techniques using single stitches, figure-of-8 stitches, or combined single and figure-of-8 stitches have been described previously, and the advantages and disadvantages of each have been elucidated. We describe a modification of the pericostal suture technique introduced by Katz 6 in 1997, which allows reinforcement against diverse causes of dehiscence.
Technique
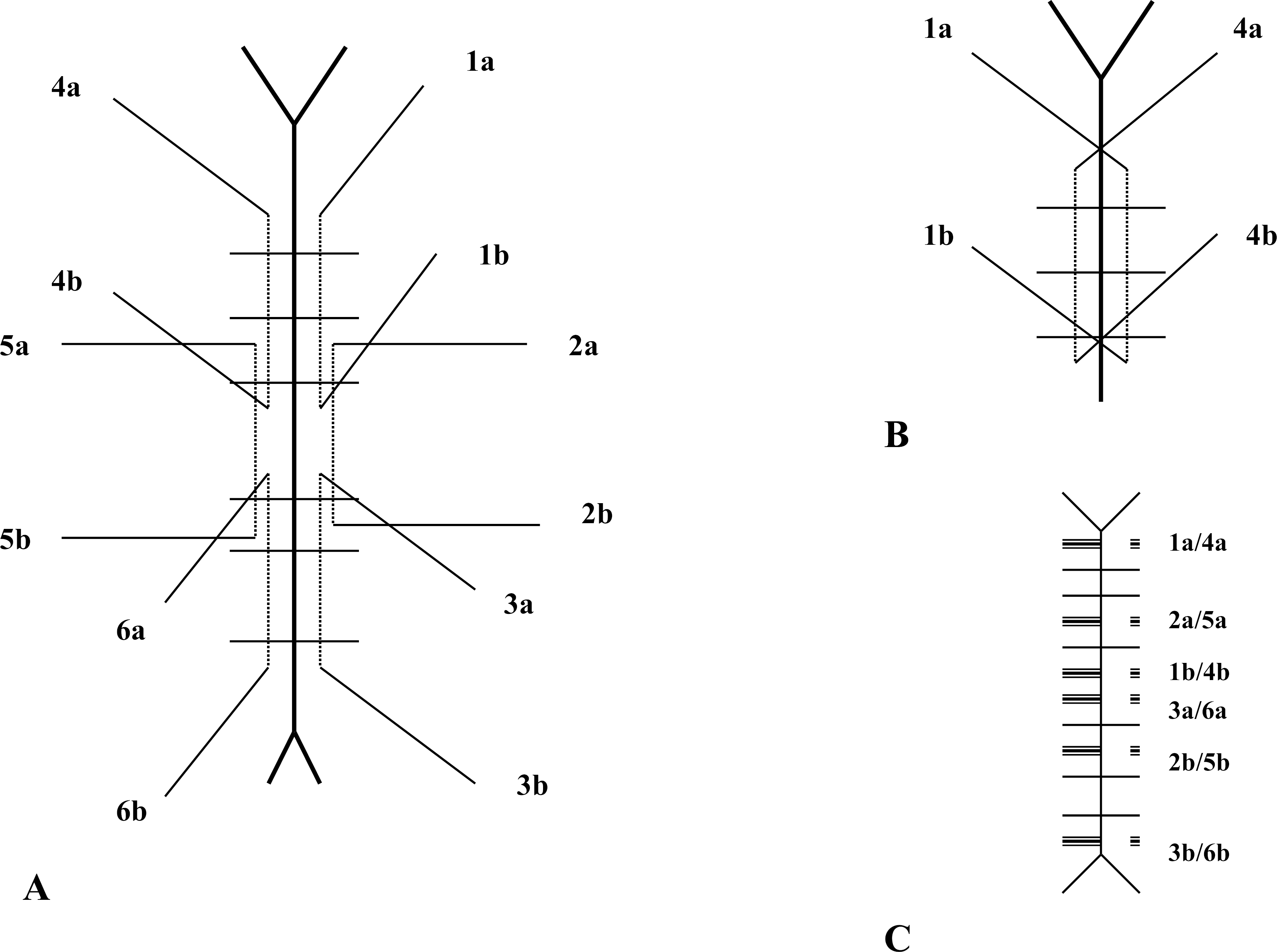
Before placing single transverse steel wires, 3 overlapping longitudinal steel wires are inserted through both sides of the sternum so that they are completely reinforced (Figure 1). After implementing the longitudinal reinforcement, 6 or more conventional single steel wires are placed, being careful to enter the sternum laterally to the longitudinal chain. After placing all the wires, 12 strands of steel wire are located at each side of the sternum. The transverse wires are tightened first in the usual fashion (Figure 2A). In the second step, the longitudinal steel wires are tightened using the schema shown in Figure 2B. Each strand of the longitudinal steel wires is tightened with the facing strand of wire at the opposite side of the chest, being careful to tighten forcefully only the inferior couple of strands of each longitudinal wire. The final aspect of the sternum is shown in Figure 2C. In case of emergency surgical revision, this reinforced closure, despite the apparent complexity, can easily be reopened by cutting the sequence of transverse wires alternately to the right and left of the notch.
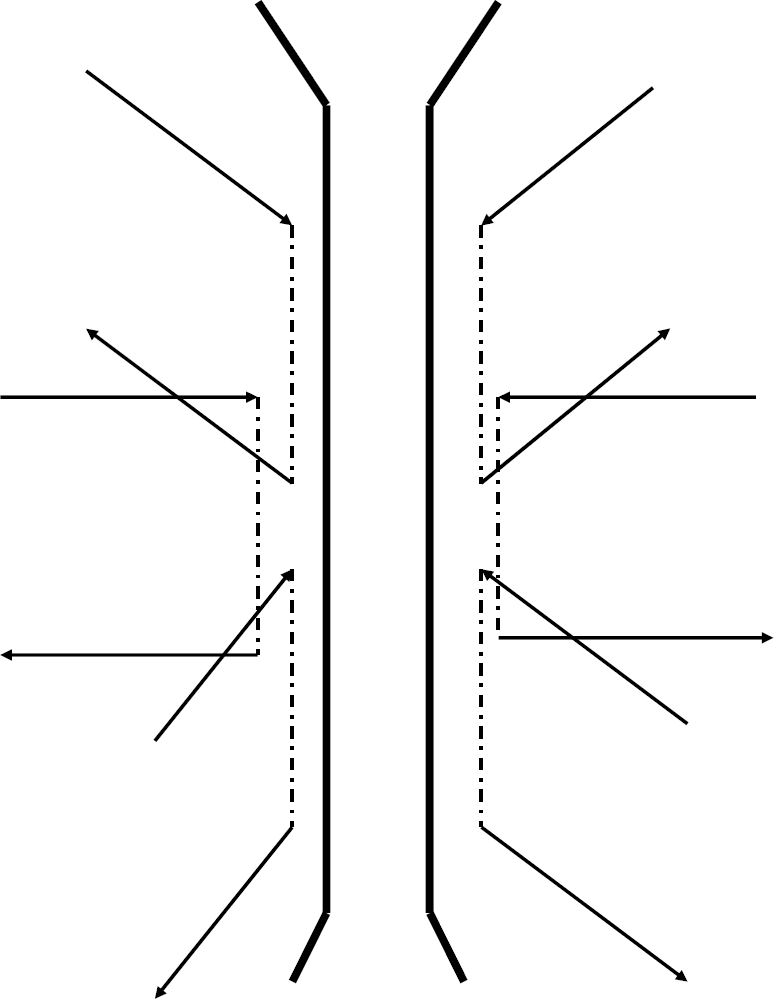
Three overlapping steel wires are placed through both sides of the sternum, before placement of the conventional six transverse wires.
Discussion
During a 2-year period (January 2000 to December 2001), 34 of the 1,619 (2.1%) patients who underwent cardiac surgery by a midline sternotomy experienced sternal dehiscence and underwent sternal re-fixation by this technique. The sternal dehiscence was septic in only 4 patients (11%); the other 30 were aseptic. None of these patients presented with sternal osteomyelitis. The mechanism of dehiscence was fracture of the sternal wire in 11 patients (33%) and a sternal tear in 23 (67%). The re-fixation procedure was performed 6 to 73 days (mean, 13 ± 14 days) after the primary closure. The postoperative course was uneventful in all patients and they were discharged 4–21 days (mean, 7 ± 4 days) later. Follow-up ranged from 30 to 52 months (mean, 41 ± 7 months), and no infection or recurrence of dehiscence occurred.
Sternal dehiscence is still reported in 1%–2% of patients after cardiac surgical procedures, and its incidence is related to several risk factors including older age, obesity, diabetes, chronic obstructive pulmonary disease, chronic steroid treatment, and bilateral mammary artery harvesting. 8 Several different techniques have been described for reinforcing the approximation of the sternum in the case of re-fixation. In 1977, Robicsek and colleagues 1 introduced the concept of longitudinal reinforcement. This is still one of the best-known techniques for re-fixation and it is especially indicated in dehiscence due to multiple transverse fractures. Others simplified this technique, retaining the concept of longitudinal reinforcement. 2,3 Nevertheless, different approaches have been described using figure-of-8 pericostal wires or fixed longitudinal reinforcement. 4,5 In 1997, Katz 6 proposed a simple technique that involved pericostal wires tightened against the facing wire at the opposite side of the sternum. We started to use this technique but experienced a recurrence of dehiscence due to fracture of the longitudinal wire. Therefore, we decided to modify the technique to achieve additional reinforcement.
The two main differences in our technique from that described by Katz 6 are overlapping of the longitudinal wires, which allows residual stabilization even when one of the wires is fractured, and placement of the longitudinal wires through the sternum instead of pericostally, which allows overlapping and avoids the risk of postoperative bleeding. This technique allows a further mechanism of reinforcement against repeat sternal dehiscence. The longitudinal wires provide reinforcement against sternal tear, which is especially frequent in the osteoporotic patient, and stabilize transverse fractures of the sternum. Simultaneously, the transverse fixation of two facing longitudinal wires provides reinforcement against fracture, which can be especially frequent in obese patients as well as in those with chronic obstructive pulmonary disease and severe postoperative cough. In our series, we did not encounter any case of sternal osteomyelitis; therefore, the feasibility of the technique in this condition needs further evaluation. In case of severe sternum osteomyelitis, however, we believe that complete sternal debridement remains the treatment of choice.
Recurrent sternal dehiscence can be caused by different mechanisms and reinforced closure should prevent against all the potential causes. This technique allows diverse reinforcement and thus could further reduce the risk of recurrent dehiscence. Our satisfactory clinical experience with this technique tends to confirm its feasibility in the treatment of sternal dehiscence after cardiac surgery through a midline sternotomy.