
Abstract
Starr-Edwards ball valves removed more than 15 years after implantation were retrospectively investigated macroscopically. Eight patients required re-operation. Valve models used in the initial operations were a non-cloth-covered valve in 2 patients and a cloth-covered valve in 6. Two patients had replacement of an aortic ball valve (model 1260 and model 2320) and 6 underwent mitral valve replacement (model 6120 in one, model 6320 in 5). The mean time to re-operation was 23.0 ± 4.8 years after implantation. Cloth wear causing significant hemolysis was observed in all cloth-covered valves, regardless of valve position. Autologous tissue growth was noted on the orifice ring and struts in both aortic and mitral prostheses. Thrombus formation was not found in any of the valves. Ball variance in silicone rubber balls was mild in the non-cloth-covered valves, even in the aortic position. The most significant problem with the cloth-covered ball valve was cloth wear. Cloth wear should always be considered when 15 years or more have passed since valve implantation. Significant hemolysis, elevation of lactate dehydrogenase values, and echocardiographic detection of transvalvular regurgitation are diagnostic of cloth wear, and are indications for replacement of a cloth-covered ball valve.
Introduction
The Starr-Edwards (S-E) ball valve prosthesis was the first artificial cardiac valve introduced for valvular heart disease in 1961. 1 Since the first clinical use of the original S-E ball valve, several modifications in materials and design have been made to improve the hemodynamic performance and durability, and to decrease the incidence of thromboembolism. This valve prosthesis has shown excellent durability, however, some specific complications have also been experienced, such as cloth wear, embolism, pannus formation, and ball variance. 2 –8 We examined 8 S-E ball valves that were removed from the aortic or mitral position more than 15 years after implantation. The diagnostic and therapeutic strategies for complications related to the S-E ball valve are discussed.
Patients and Methods
The S-E ball valve was employed for replacement of left heart valves at our hospital between 1965 and 1975; 46 patients received a ball valve in the aortic or mitral position. Of the 24 long-term survivors, 8 required re-operation due to prosthetic valve dysfunction or progression of other cardiac valve diseases. The clinical characteristics of these 8 patients are summarized in Table 1. The 2 aortic S-E ball valves were replaced at 20 and 28 years after implantation, and the 6 valves in the mitral position were explanted after 15 to 30 years (mean, 23 years). Indications for re-operation are listed in Table 1. Replacement of the S-E ball valve with a mechanical bileaflet valve was performed under moderate hypothermic cardiopulmonary bypass and cardioplegic arrest, through a median sternotomy incision in all 8 patients. The S-E ball valves removed at re-operation were studied for cloth wear, pannus formation, thrombus, and ball variance.
Clinical Data Relating to 8 Explanted Starr-Edwards Ball Valves
AR = aortic regurgitation, ARF = acute renal failure, ASR = aortic stenotic regurgitation, CAD = coronary artery disease, LA = left atrial, MS = mitral stenosis, PVL = paravalvular leak, TIA = transient ischemic attack, TSR = tricuspid stenotic regurgitation.
Results
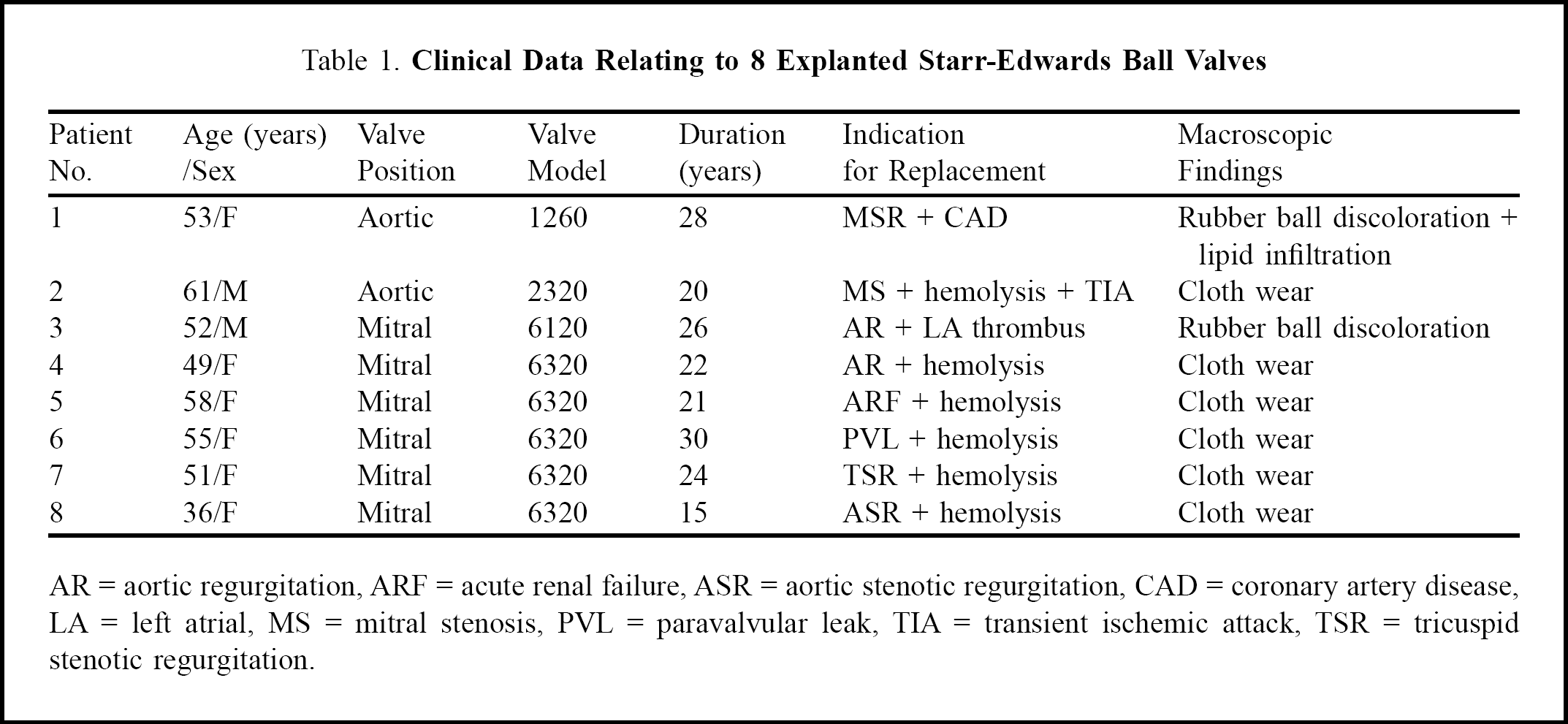
Cloth wear was observed in all 6 cloth-covered S-E ball valves (model 2320 aortic valve in one patient and model 6320 mitral valve in 5). The explanted valve prostheses showed extensive cloth wear with exposure of the metal along 3 or 4 of the struts. The metal on the orifice ring was also exposed where the poppet is normally seated during valve closure. The severity of cloth wear on the struts and the orifice ring did not differ between valves in the aortic or mitral position, as shown in Figure 1.
Explanted aortic (
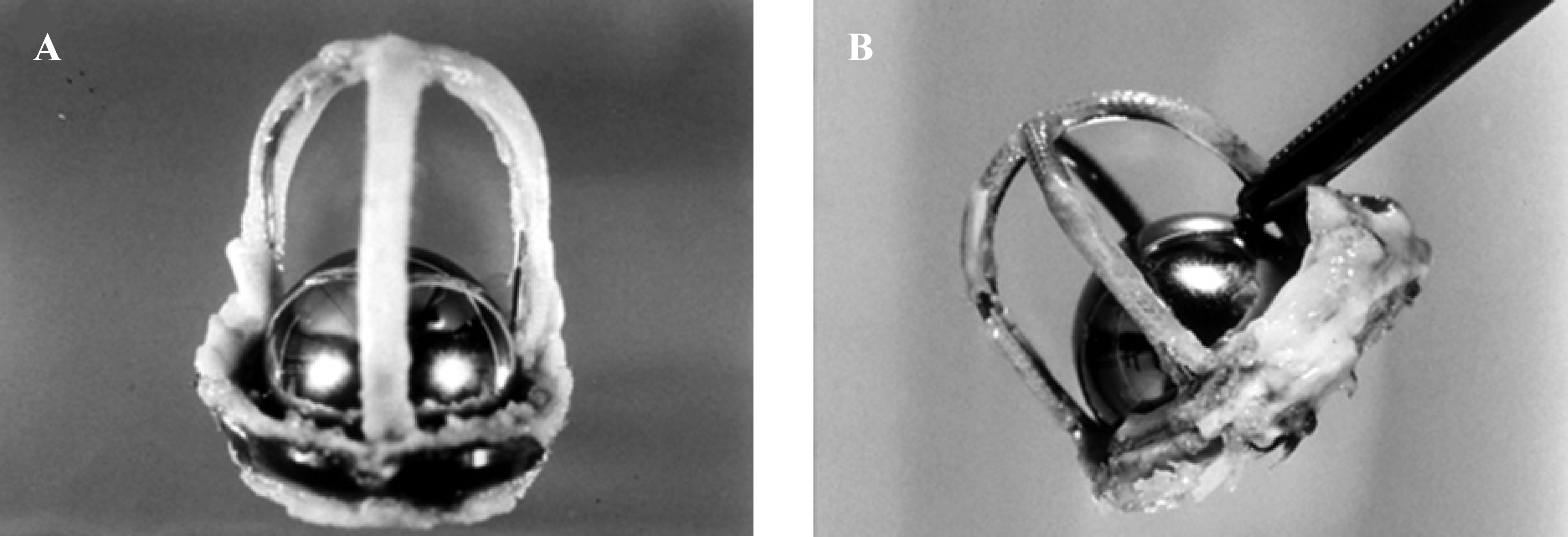
Autologous tissue growth was found on the struts of all 6 cloth-covered valves, but was not observed on the bare metallic struts in 2 non-cloth-covered ball valves (model 1260 aortic and model 6120 mitral), as shown in Figure 2. Excessive fibrous tissue growth on the sewing ring was detected in all 8 of the S-E ball valves, regardless of valve model. However, excessive pannus overgrowth on the valve orifice leading to prosthetic valve obstruction or incompetent closing was not observed. Continuous oral anticoagulant therapy with warfarin was maintained to keep the Thrombotest index at 20% to 30% or the international normalized ratio at 1.5 to 1.8 in all 8 patients. No thrombi on the struts or valve orifice were seen in any of the prosthetic valves.
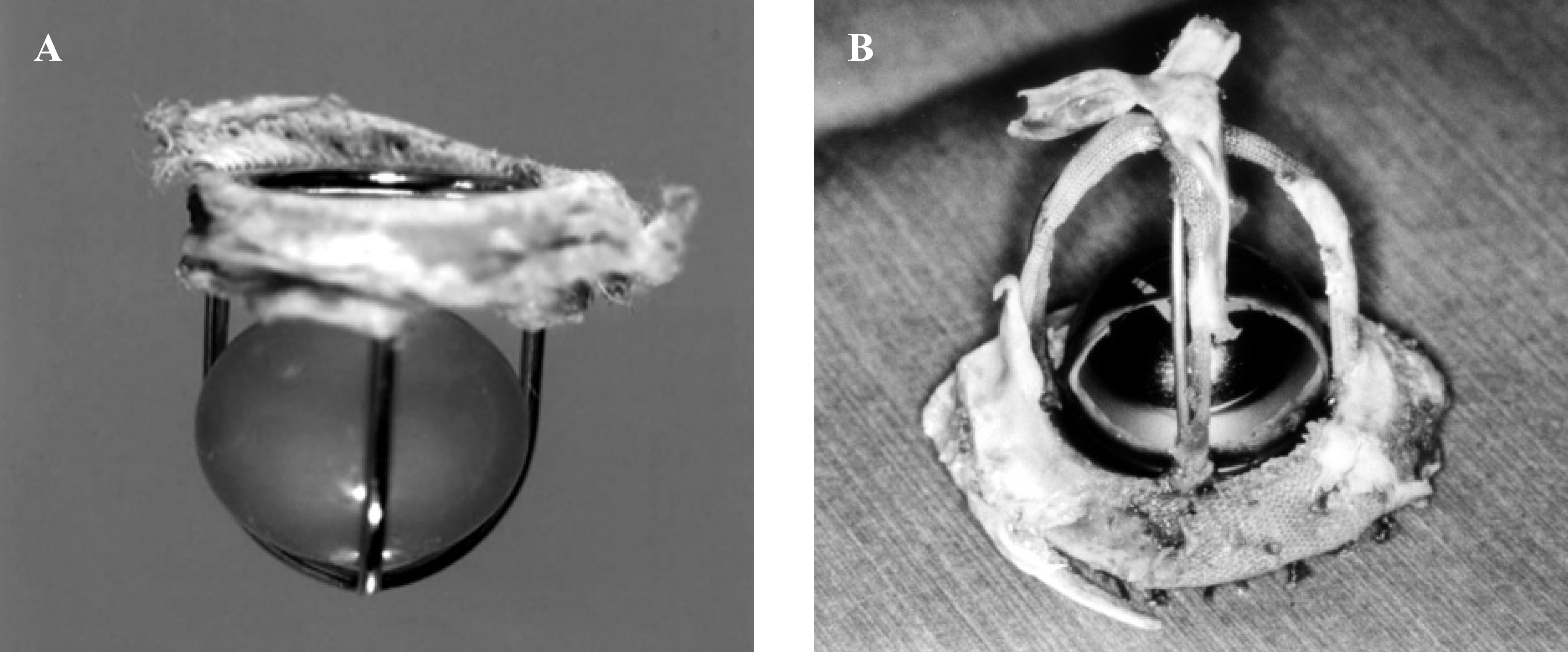
An explanted aortic non-cloth-covered ball valve (
Of the 8 S-E ball valves removed, 2 had a silicone rubber ball and 6 had a hollow Stellite ball. Discoloration and small spots of lipid infiltration on the surface of the silicone rubber ball were found in the model 1260 aortic valve, and discoloration alone was observed in the model 6120 mitral valve, as shown in Figure 2. Ball variance in these cases was classified as mild. 9 No ball variance, including discoloration, was seen among the hollow Stellite balls in the aortic and mitral positions.
Significant hemolysis was noticed in 6 patients who had a cloth-covered ball valve with cloth wear; one had a model 2320 aortic valve and 5 had a model 6320 mitral valve. Serum lactate dehydrogenase levels were remarkably high in all 6, and total bilirubin levels were over 1.2 mg·dL−1 in 4 of the 6 patients. Blood smears revealed fragmentation of erythrocytes in 3 patients. Hematologic data in these 6 patients are summarized in Table 2. Systemic embolism was experienced in one patient with a model 2320 aortic ball valve. After the 4th postoperative year, transient cerebral ischemic attacks occurred 4 times during the next 15 years. At re-operation, severe cloth wear was found in this ball valve (Figure 1A).
Hematologic Data in 6 Patients with Valves Exhibiting Cloth Wear
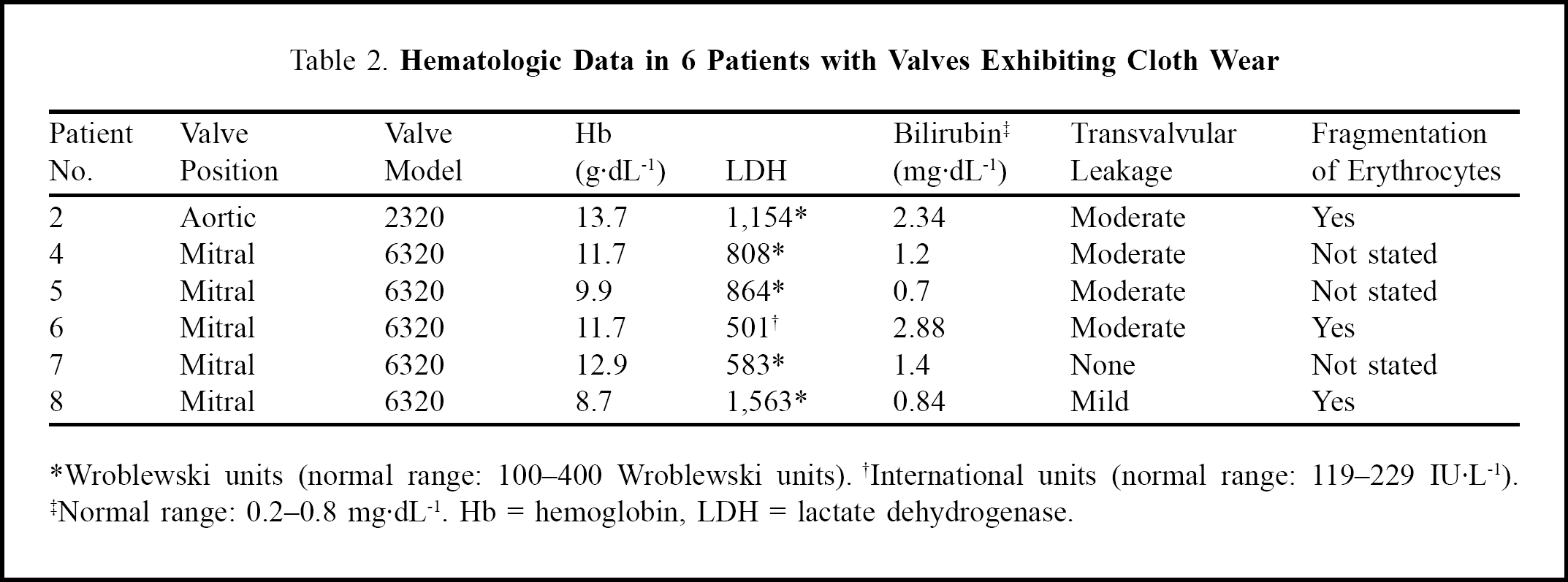
Wroblewski units (normal range: 100–400 Wroblewski units). †International units (normal range: 119–229 IU·L−1). †Normal range: 0.2–0.8 mg·dL−1. Hb = hemoglobin, LDH = lactate dehydrogenase.
Echocardiography was performed to evaluate prosthetic valve function in all 8 patients. Although significant prosthetic valve obstruction was not found, transvalvular regurgitation was detected in 5 of the 6 patients with cloth-covered ball valves. Transvalvular regurgitation was diagnosed as moderate in 4 patients and mild in one. In the remaining cloth-covered ball valve, transvalvular regurgitation was not detected, but cloth wear was found at re-operation.
Discussion
Three models of the S-E ball valve prostheses, non-cloth-covered, cloth-covered, and a composite strut (track) model, were introduced for clinical use. The non-cloth-covered valves (models 1260 and 6120) had bare metallic struts composed of Stellite without any cloth covering, and a silicone rubber ball. In the cloth-covered valves (model 2320 aortic and model 6320 mitral), the metallic struts and orifice ring were completely covered by Dacron or Teflon cloth, and a hollow Stellite ball was incorporated. The composite strut models (2400 aortic and 6400 mitral) resembled the model 2320 aortic and 6320 mitral valves except that it had metallic tracks on the inner aspect of the cloth-covered struts. Only the first two types of S-E ball valve were implanted in our hospital.
Ball variance due to lipid infiltration as well as thromboembolism was a major problem with the non-cloth-covered ball valve. However, ball variance occurred mainly in the model 1000 aortic prosthesis, and only a few cases of abnormal poppets showing discoloration have been reported in the model 1260 aortic prosthesis that was employed in our series. In our experience, discoloration was found on the silicone rubber ball in the model 1260 aortic and 6120 mitral prostheses implanted 28 and 26 years previously, respectively, but moderate or severe ball variance was not observed even 25 years or more after implantation. Although the introduction of cloth-covered ball valve prostheses has substantially reduced the incidence of thromboembolism in patients receiving anticoagulant therapy, cloth-covered valves have been associated with problems of cloth wear resulting in hemolysis and systemic arterial embolization. 1,2 Cloth wear was found in all of the model 2320 and 6320 cloth-covered ball valves used in our 6 patients. In an early report from the New York Veterans Administration Hospital, 4 (3.3%) of 121 survivors with cloth-covered aortic S-E valve prostheses, and one (1.2%) of 83 survivors with cloth-covered mitral S-E valve prostheses had re-operations for consequences of cloth wear, an overall incidence of 2.5%. 3 Similarly, one Japanese study initially reported that cloth wear of the S-E ball valve was more frequent and remarkable in the aortic position than in the mitral position. 2 A recent follow-up study over 15 years from the same group has emphasized that cloth wear is frequently detected not only in the aortic position but also in the mitral position. 10
The two major complications due to cloth wear are cloth fiber emboli to the systemic circulation and hemolysis with or without regurgitation across the prosthesis. According to a previous study, cloth fiber emboli can occur with either aortic or mitral valve prostheses, while clinically significant hemolysis is associated only with the aortic prosthesis. 8 In our experience, however, significant hemolysis was seen in 6 patients, and 5 of them had a ball valve in the mitral position. A sail or parachute effect of the worn cloth in the bloodstream jet plays an important role in the severe hemolysis caused by cloth wear of the S-E valve prostheses (Figure 3). This effect creates increased turbulence and accelerated hemolysis. 11,12 Thus, it is logical that significant hemolysis due to cloth wear can occur with S-E valves even in the mitral position. Based on our experience and that of others, even when no clinical findings that suggest significant cloth wear have been demonstrated, cloth wear should always be considered when 15 years or more have passed after valve replacement with a cloth-covered S-E ball valve. 2
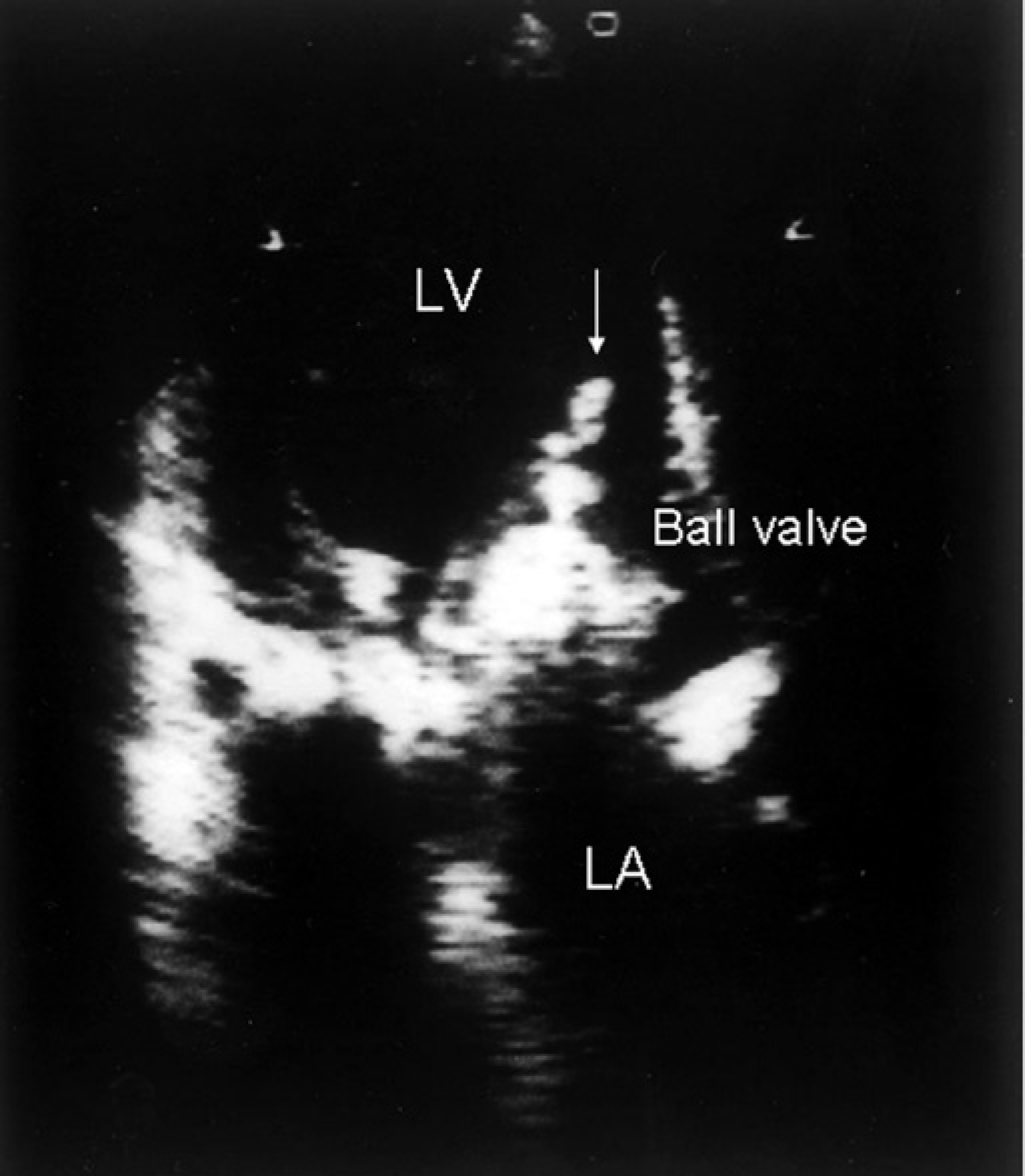
Transthoracic echocardiogram demonstrating excessive tissue attached to the cage of the prosthesis, which was fluttering in the blood stream; a sail or parachute effect of the worn cloth in the bloodstream jet is also observed (white arrow). LA = left atrium, LV = left ventricle.
In our patients, the diagnosis of clinically significant cloth wear was made by the presence of significant mechanical hemolysis (anemia or jaundice) with fragmentation of erythrocytes, elevation of serum lactic dehydrogenase, and trans-prosthesis regurgitation on echocardiograms. As cloth wear resulting in incomplete seating of the poppet allows transvalvular regurgitation, echocardiographic detection of transvalvular regurgitation in patients with cloth-covered ball valves will imply the presence of cloth wear. 2 In addition, the incidence of thromboembolism is uncommon after 4 years in patients with cloth-covered ball valves, thus recurrent systemic arterial embolization despite adequate anticoagulation more than 4 years after valve replacement should strongly arouse suspicions of cloth fiber emboli rather than thromboemboli. 13 One of our patients experienced repeated transient cerebral ischemic attacks after the 4th postoperative year. Once cloth fiber emboli are identified, the valve should be replaced as soon as possible, even if patients are asymptomatic, to prevent the occurrence of fatal systemic emboli, because the operative mortality rate for redo valve replacement is very low.