
Abstract
In the subcontinent, improving life expectancy may increase the number of elderly patients requiring coronary artery bypass. The elderly have a higher risk of mortality, and cost vs benefit is presumed to be unrewarding, leading to a disinclination to operate on such patients. We reviewed the records of patients ≥ 70 years old undergoing coronary revascularization in a 10-year period. Between 1995 and 2004, 3,312 coronary bypass operations were performed, including 242 (7.3%) in patients ≥ 70 years. Of these, 207 (86%) were male, 73 (30%) had non-elective surgery, and 177 (73%) had a high-risk EuroSCORE. Early postoperative mortality was 8.7% (21/242), and 33 (13.6%) patients experienced morbidity. One-year follow-up of 106 (44%) patients was possible. There were 4 (1.7%) late deaths from noncardiac causes. Death, morbidity, and postoperative functional class were significantly associated with preoperative functional class. Meticulous selection of elderly patients for coronary artery bypass may help maximize the benefits of this surgery.
Introduction
Demographic and epidemiologic transitions have changed the population structure. 1 Life expectancy at birth is increasing globally. In Europe, it has been raised from 71 to 83 years in the last four decades, and life expectancy at age 65 ranges from 16 to 19 years. 2 In the USA, it has increased by 2 years since 1989; this smaller increment may be due to an already high life expectancy of 75.5 years. 3 A much sharper 5–6 year increase has been observed in Southeast Asia in the last 7–8 years. By 2020, the number of elderly people is projected to reach more than 1000 million, with 70% living in developing countries, especially in China, India, Indonesia, Brazil, and Pakistan. 4 –6 On one hand, this is an indicator of good health in the early years of life, but paradoxically, it also serves as an indicator of the higher prevalence of degenerative diseases in later age. 7 For example, an increasing incidence of coronary artery disease with age has been reported in the absence of any other risk factor. 8,9 Further, diabetes mellitus, an established risk factor for coronary heart disease (CHD) is on the rise worldwide, while obesity, smoking, dyslipidemia, and hypertension are highly prevalent. 10 –12 This has led to a rapid rise in the number of elderly people with CHD requiring surgical intervention in the developed countries during the last two decades. 13 Higher prevalence of these risk factors has been reported among Asians who are also at higher risk of developing diabetes mellitus. 14,15 This may subsequently lead to a higher incidence of CHD and it may be anticipated that a greater number of elderly patients with CHD will be considered for revascularization procedures. However, due to the relative lack of data from our region, management strategies in such patients are not clearly defined. At times, concerned factions are disinclined to offer surgery as these patients have a higher risk of morbidity and mortality after surgery. 16 Uncertainty increases in the presence of multiple comorbidities, raising complex healthcare issues such as benefit vs cost of treatment. Whether such patients should undergo surgery has assumed great importance both for the individual and for society. We at The Aga Khan University have embarked on measures to gain an insight from our 10-year experience of isolated coronary artery bypass grafting (CABG) in the elderly.
Patients and Methods
The Aga Khan University hospital is a private tertiary care hospital that also provides subsidized treatment to a number of poorer patients. Using our computerized database, we selected all patients ≥ 70 years of age who underwent isolated CABG from 1995 to 2004. The medical records were retrieved, and information was added to a dataset developed specifically for this study. Age was an important variable in this study; it was determined at the time of first contact at the registration desk, as reported by the patient, and verified by national identity card when available. Other variables considered were indication for surgery, severity of disease, comorbidities, EuroSCORE, priority of admission, and type of surgery. Renal failure was defined as serum creatinine 1.5 mg·dL−1. Left ventricular (LV) dysfunction was categorized on the basis of ejection fraction and considered severe, moderate, mild, or normal if ejection fraction was < 35%, 35 to < 45%, 45 to < 55%, or 55% and above, respectively. Perioperative variables included use of an intra-aortic balloon pump, type of graft, and duration of surgery. Postoperative characteristics included length of stay and outcome; outcomes included 30-day mortality, complications, and New York Heart Association (NYHA) functional class improvement. Functional class improvement was assessed at follow-up and by telephone questionnaire. All patients who remained in the same functional class postoperatively were considered ‘not improved’, except for those in class I preoperatively.
Surgical revascularization was indicated on the basis of clinical and angiographic findings. A standard operating strategy with cardiopulmonary bypass was used. After induction of anesthesia, a median sternotomy was performed, bypass conduits (arterial and venous) were procured, and cardiopulmonary bypass was established using right atrial and aortic cannulation after systemic heparinization (300 units·kg−1). Myocardial protection was achieved with blood cardioplegia infused antegradely via the aortic root, and retrogradely through the coronary sinus in selected cases, along with moderate hypothermia (28°C–32°C). Topical cooling was used to enhance myocardial protection. Distal coronary anastomoses were performed on an arrested heart. After rewarming and aortic declamping, the proximal ends of the vein grafts were anastomosed to the aorta using a partial occluding clamp. In certain cases, a single clamp was used for both distal and proximal anastomoses when the aorta was diseased. Subsequently, the heart was allowed to perfuse, and the patient was weaned from cardiopulmonary bypass. Protamine was given to neutralize heparin. Aortic and venous cannulas were removed. Standard chest closure was carried out after ensuring hemostasis and placement of drains and a pacing wire.
The data were analyzed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA). Frequencies, normal distribution curves, and outliers were checked for continuous variables, and in case of doubt, were verified from patients’ files. For categorical variables, we looked at counts and percentages. No replacement was made for missing values. Student's t test and McNemar's test were used for evaluating the association of death, complications, and postoperative NYHA class vs preoperative class. To determine the factors associated with death, the chi-square or Fisher's exact tests were used.
Results
Figure 1 shows the distribution of cases over the 10-year period. Of 3,312 CABG operations, 242 (7.3%) were performed on patients ≥ 70 years of age, and the proportion of elderly patients undergoing CABG remained more or less unchanged during these 10 years. Table 1 lists the preoperative characteristics of the patients; most were male, 7 (2.9%) were ≥ 80 years old, 14 had a history of transient ischemic attack or cerebrovascular accident, 6 were positive for hepatitis B, and 2 had malignancy. Perioperative characteristics are shown in Table 2. One nephrectomy and 3 endarterectomies were performed concomitantly. The postoperative data are given in Table 3. No patient required reinstitution of ventilatory support, and none experienced postoperative myocardial infarction. There were 25 deaths, including 21 hospital deaths (8.7%) within 30 days; 9 of these were due to multi-organ (cardiorespiratory and/or renal) failure, 4 due to respiratory failure, 3 due to cardiac failure, 1 each due to cerebrovascular accident and acute renal failure, and no cause could be established in the other 3. Most (95%) of the patients who died were from the high-risk group (EuroSCORE 6+). The 4 late deaths were due to noncardiac causes (late mortality, 1.7%).
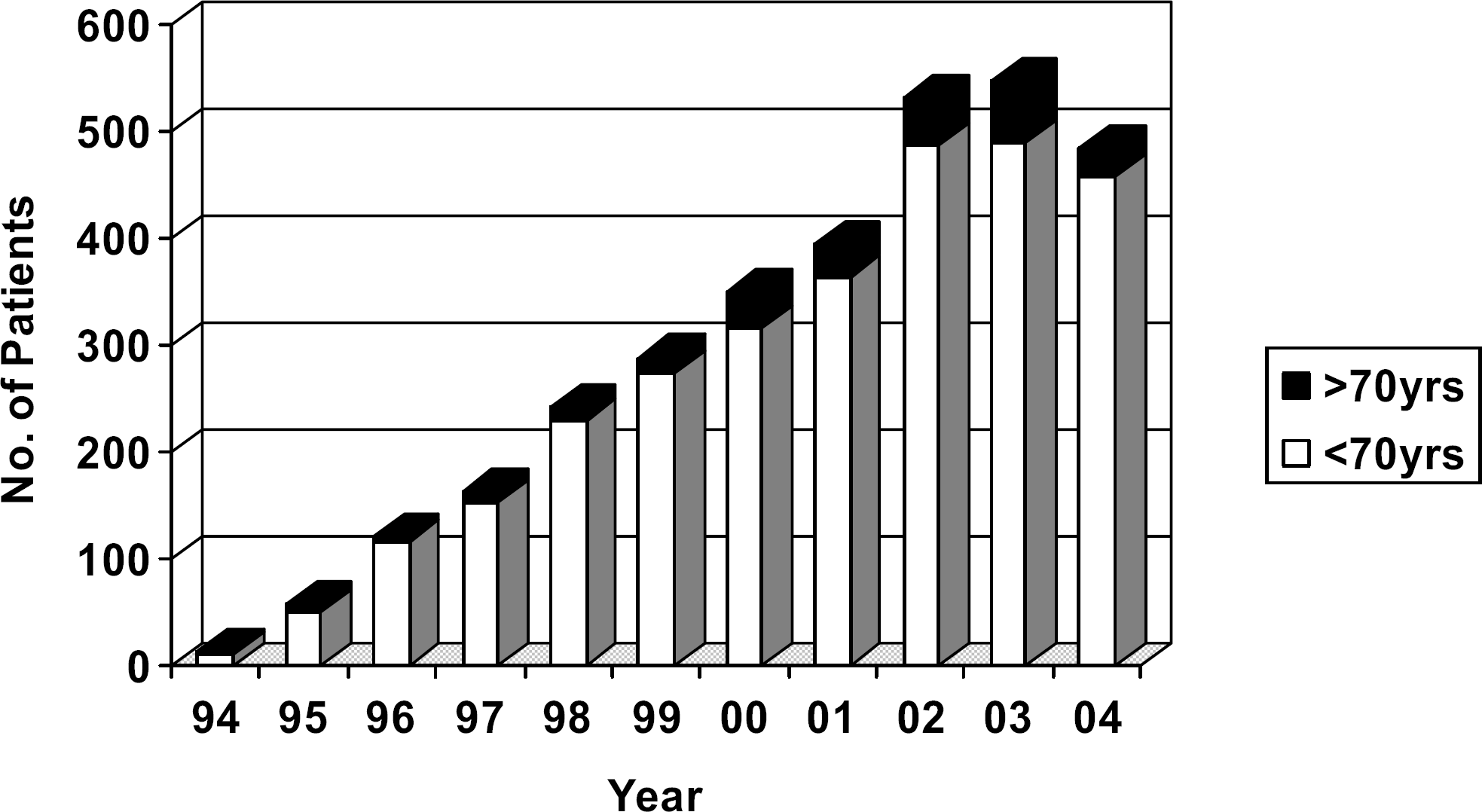
Yearly rates of isolated coronary artery bypass operations at The Aga Khan University, Karachi, Pakistan, 1995–2004.
Preoperative Characteristics of 242 Elderly Patients Undergoing Coronary Artery Bypass
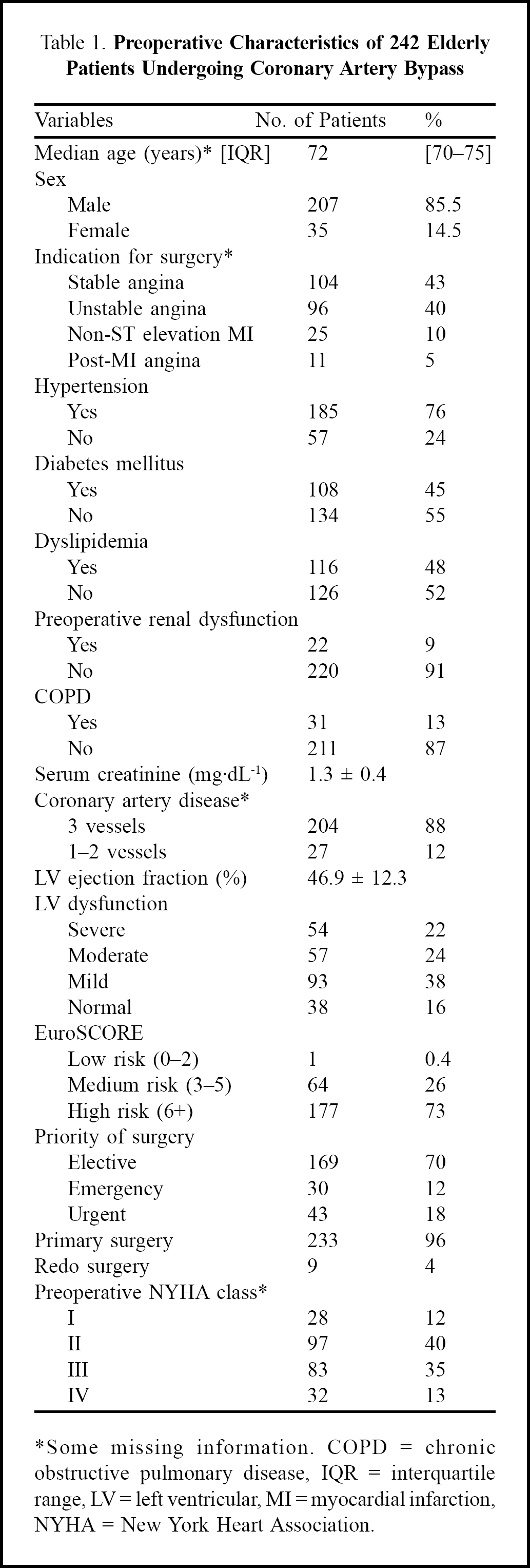
Some missing information. COPD = chronic obstructive pulmonary disease, IQR = interquartile range, LV = left ventricular, MI = myocardial infarction, NYHA = New York Heart Association.
Perioperative Characteristics of 242 Elderly Patients
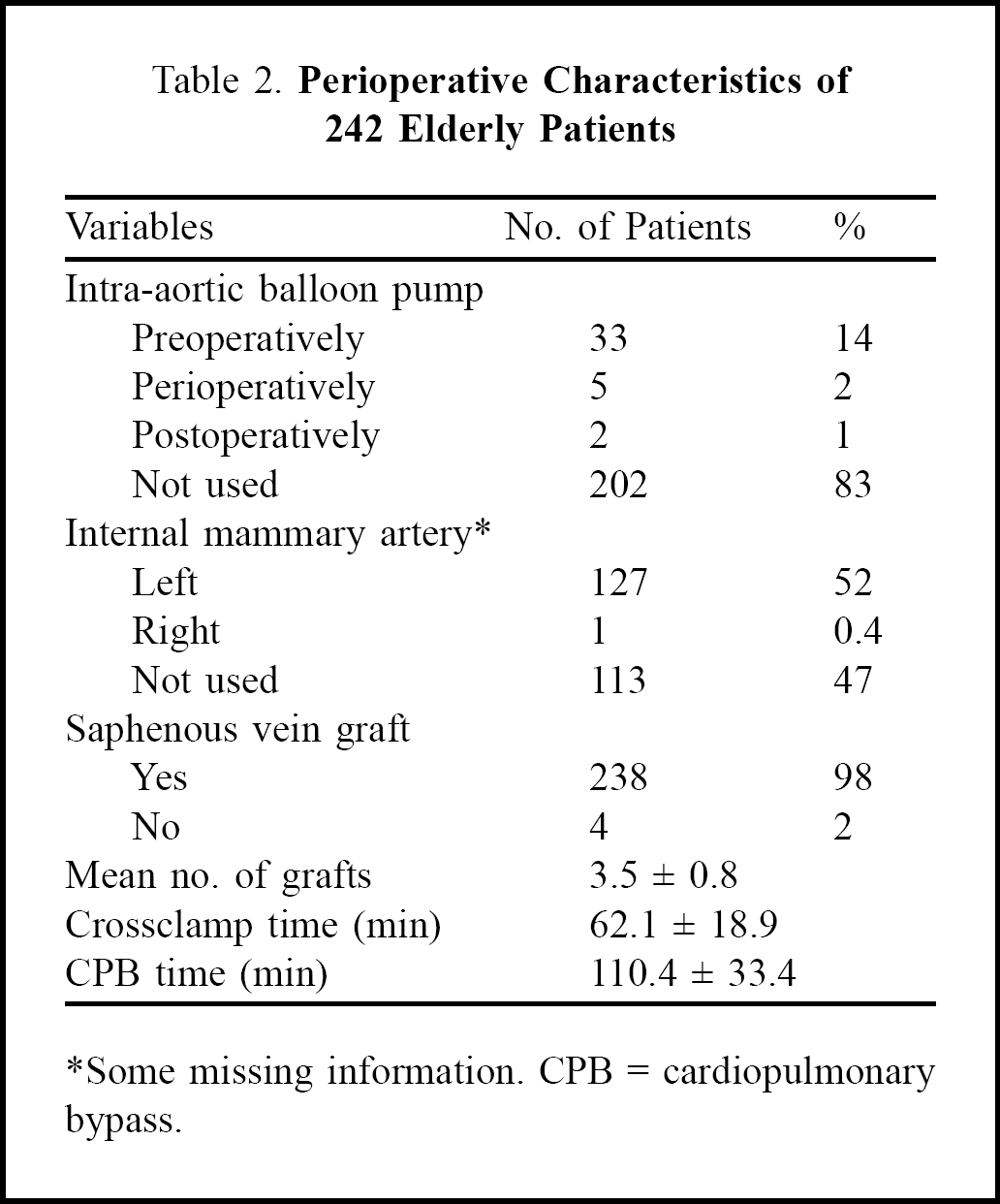
Some missing information. CPB = cardiopulmonary bypass.
Postoperative Characteristics of 242 Elderly Patients
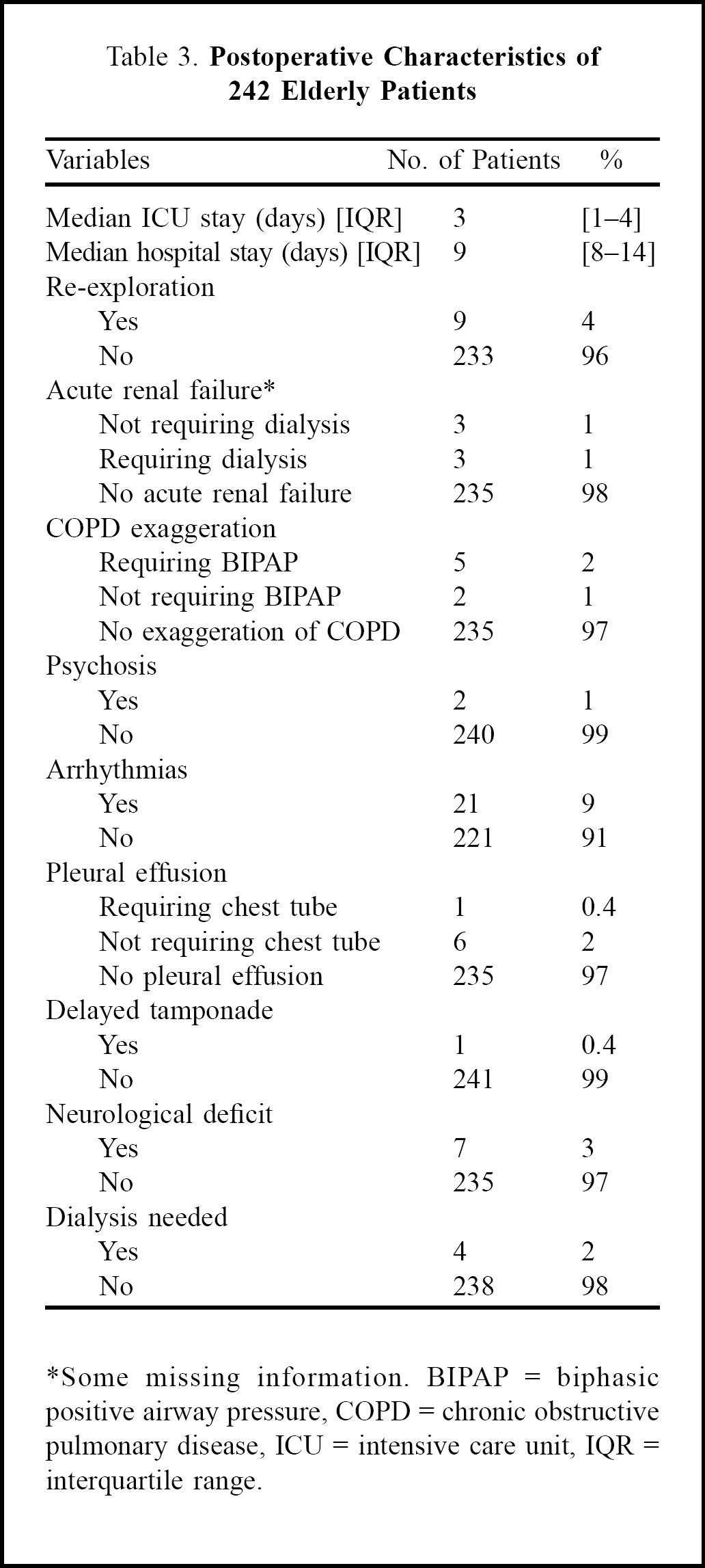
Some missing information. BIPAP = biphasic positive airway pressure, COPD = chronic obstructive pulmonary disease, ICU = intensive care unit, IQR = interquartile range.
Postoperative complications were observed in 33 (13.6%) patients; the most common complications were arrhythmias followed by re-exploration for bleeding. Mortality (30-day) and morbidity were associated with preoperative NYHA class (Table 4). Postoperative NYHA class improved in 81 (78%) of 104 patients from whom both pre- and postoperative functional status could be obtained; 45.8% were lost to follow-up. Median duration of follow-up was 2 years (interquartile range, 1–4 years). No significant association was found between postoperative functional class improvement and EuroSCORE (p = 0.96). Figure 2 shows the pre- and postoperative functional class. It can be seen that more of the patients in poor preoperative functional classes benefited from surgery, compared to those with good preoperative functional status, quite a few of whom deteriorated. The effects of various preoperative factors on the surgical outcome are shown in Table 5.
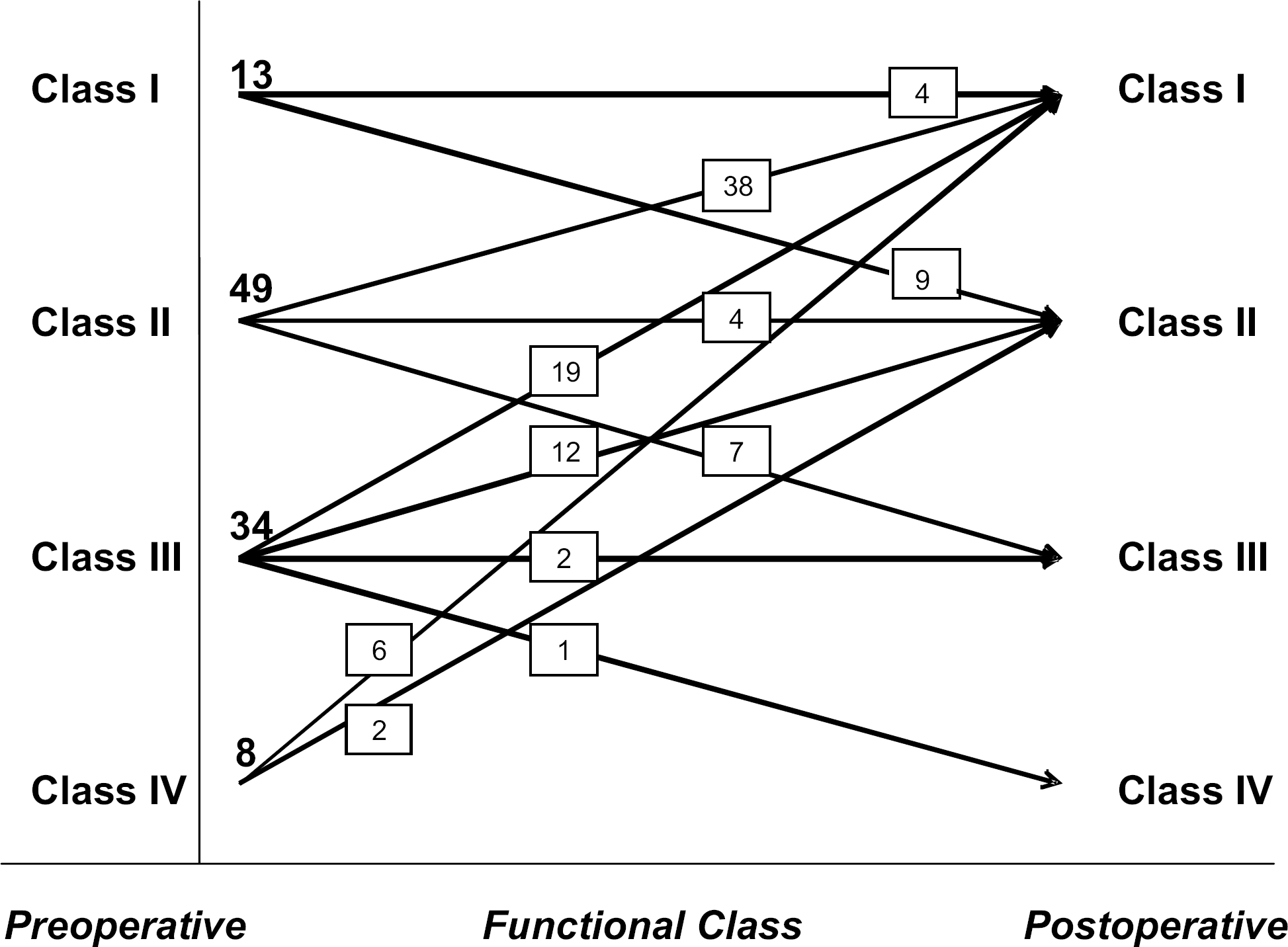
Pre- and postoperative functional class in 104 elderly patients.
Association of Preoperative Functional Class with Outcomes
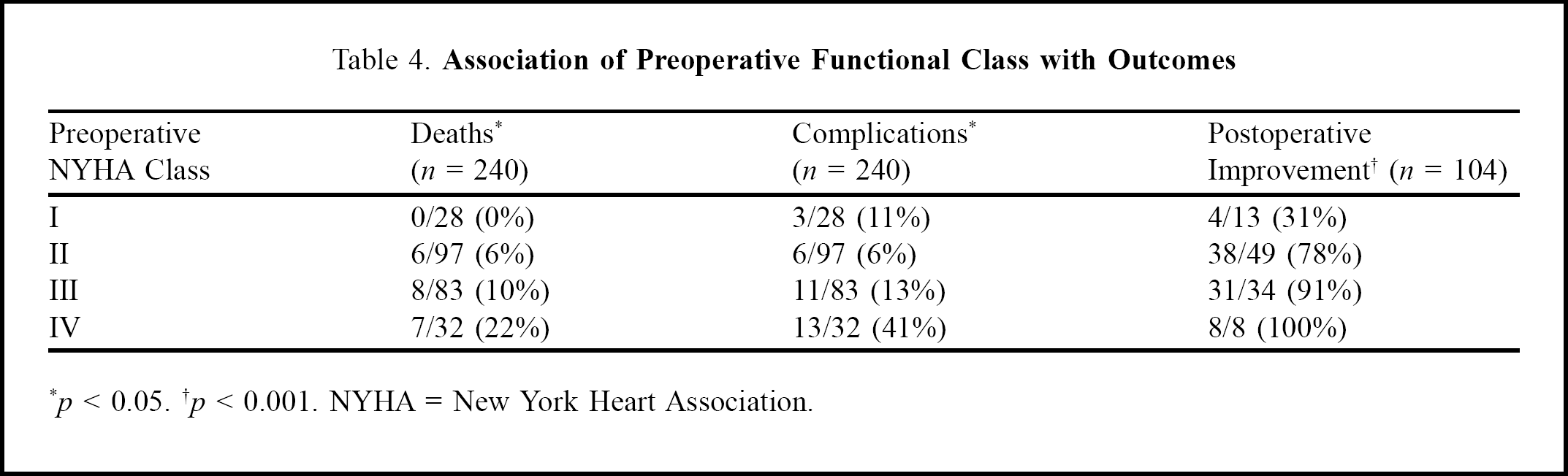
p < 0.05. †p < 0.001. NYHA = New York Heart Association.
Comparison Of Survivors And Non-survivors
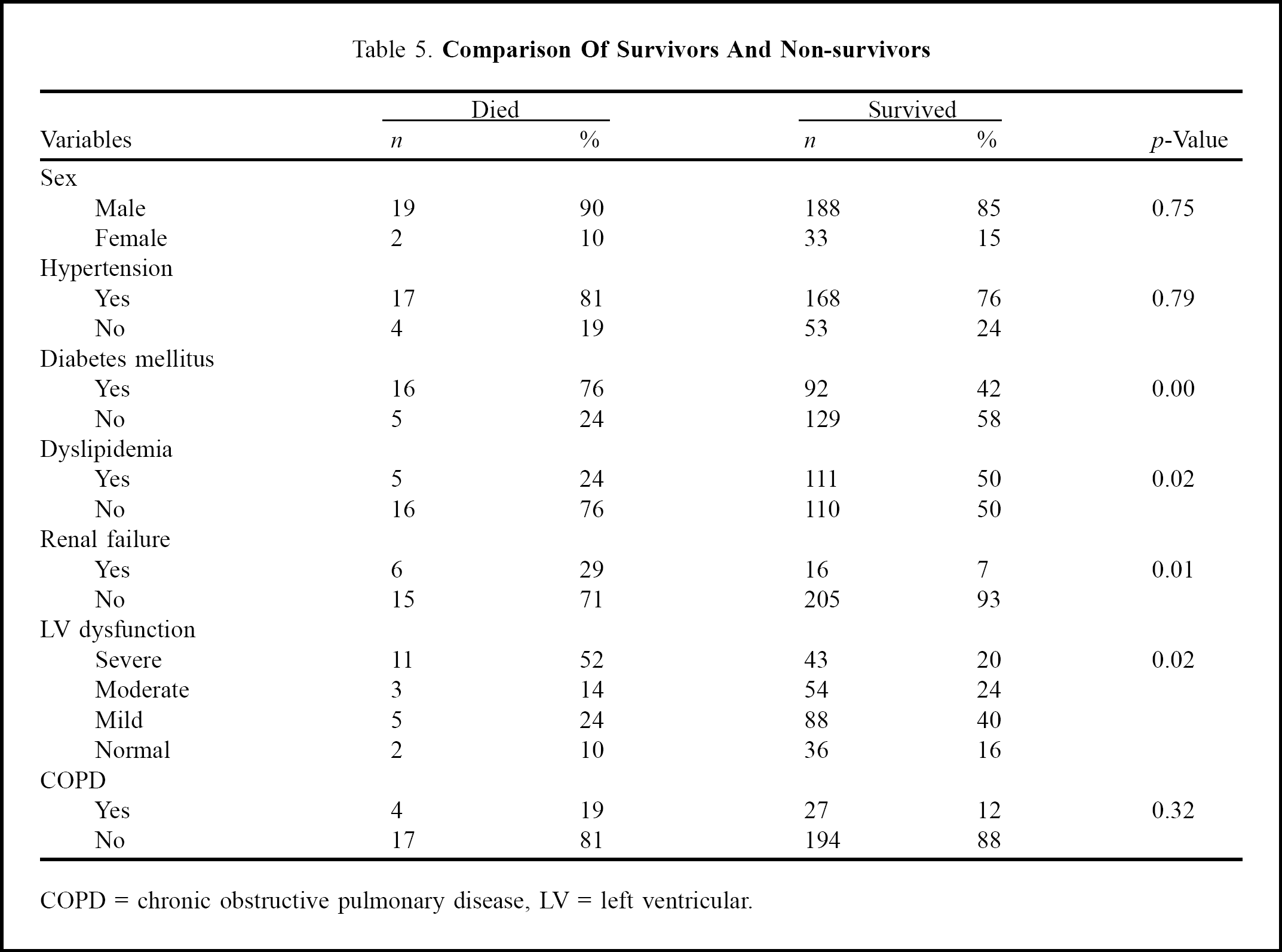
COPD = chronic obstructive pulmonary disease, LV = left ventricular.
Discussion
The finding that the proportion of the elderly patients undergoing CABG has remained more or less unchanged over the last 10 years is contrary to what we expected. This may be due to the fact that although the number of elderly people is rising, CHD is increasingly affecting younger patients, so the proportion remained the same. We collected information from our hospital where cardiac surgery was initiated. At that time, there were only 2 other cardiac surgery units in the city. Despite treating an increasing number of patients in this period, many elderly patients without healthcare insurance may have utilized services in the other, heavily subsidized, cardiac surgery facilities. As no data-sharing mechanism exists among these centers as yet, the extent of this effect on the results cannot be quantified. The period of study was also in an era of increasing use of less invasive techniques. This might have affected the outcomes of CABG in the elderly. Our percutaneous transluminal coronary angioplasty data for the last decade showed that 11.1% of procedures were on patients aged over 70 years. The ratio of PTCA to CABG procedures changed from 1:2 in 1996 to almost 1:1 in 2004.
Most of the elderly patients in our study were men, although women have a higher life expectancy. 4 This may be due to differences between the sexes in seeking healthcare, as has been reported from other parts of the world. 17,18 In Pakistan, men are given priority for healthcare provision as in most cases they are the family breadwinners. Although in old age they may no longer be earning, they still retain the privileges. It is not surprising that we had only one patient in the low-risk group (EuroSCORE 0–2). Due to old age and the high prevalence of diabetes and hypertension, most cardiac surgical patients in Pakistan are found to be at high risk. This partly reflects the reluctance to operate on functionally more independent elderly, and an inclination towards more conservative management. Almost half of the patients needed urgent surgery due to unstable angina or non-ST elevation MI, but only a third of the admissions were on an emergency or urgent basis. This discrepancy can be explained by the fact that undergoing a major surgical procedure is not an easy decision. Despite the surgeons’ advice of immediate admission, the type of admission usually remains elective. Most of our patients were also at high risk because of extensive comorbidity. Coronary artery bypass grafting mortality is higher in this group compared to younger patients, due to the high risk status of the group; but it is not far from the death rate in this age group without the disease. 19
Outcomes in terms of morbidity and mortality among patients in NYHA class I preoperatively were better than those in higher NYHA classes (Table 4). As far as the lack of improvement among 13 patients in NYHA functional class I is concerned, it is unlikely to be due to the small number. Instead, we defined this variable conservatively by considering all those who did not deteriorate from functional class I as ‘improved’, in contrast to other classes. Otherwise, all patients would have been classified as ‘not improved’. Despite this conservative approach, we found a statistically significant difference. Moreover, the steady increase in the proportion who improved with increasing functional class further supports our premise. Diabetes mellitus, renal failure, and left ventricular dysfunction were found to have a significant adverse effect on surgical outcome and must be taken into consideration when deciding on surgery. Dyslipidemia was less prevalent among patients who died.
Poor documentation 70 or more years ago prevented confirmation of all data, but this did not substantially affect the description of the study population. We were able to follow up only 106 patients, with a wide range of duration of follow-up. Due to the long period of the study, many of the patients and their relatives could not be contacted. This was unavoidable due to the design of the study, but the representation included both older and newer patients, hence chances of bias were minimal. Moreover, the skewness of the follow-up data is more likely due to the gradually increasing number of elderly undergoing CABG in recent years.
Coronary artery bypass grafting in the elderly is potentially rewarding. Meticulous selection of these patients can help maximizing the benefit of surgery. In this situation, preoperative functional class cannot serve as the sole variable in deciding on surgery. Diabetes mellitus, renal failure, and left ventricular dysfunction must be considered before a decision to operate is made; however, the exact roles of these factors must be evaluated by further studies to help surgeons take such difficult decisions on even firmer criteria.