
Abstract
Heterotaxy syndrome encompasses a wide range of anatomical variants including poor pulmonary vascular development. Surgical outcome remains poor in this difficult subgroup. Between April 1996 and November 2004, 27 patients with visceral heterotaxy were enrolled in this study. The median age at presentation was 25 days. There were 11 patients with asplenia and 16 with polysplenia. There were 5 deaths (4 in patients with asplenia, 1 in a patient with polysplenia). All patients with asplenia were scheduled for single-ventricle repair, and 5 completed a modified Fontan procedure. Of the 16 patients with polysplenia, 8 completed 2-ventricle repair and 6 had a modified Fontan. In polysplenia, actuarial survival was 93.8% at 4 months, and remained constant thereafter. In asplenia, survival was 81.8% at 1 month, and 53.0% at 1 year. A significant correlation was found between nonconfluent pulmonary arteries and mortality. The medium-term result in polysplenia was satisfactory, but not in asplenia. Nonconfluent pulmonary arteries carry a high risk of mortality, and a strategy to create pulmonary vascular confluence and satisfactory pulmonary blood flow is mandatory.
Introduction
The complexity of the cardiac malformations associated with visceral heterotaxy syndrome has been well described. Patients with asplenia syndrome remain at high risk of mortality, particularly if total anomalous pulmonary venous connection (TAPVC) coexists. Patients with polysplenia syndrome might also have a significant risk of poor outcome after single-ventricle repair. Although the surgical outcome has been improved in some institutions, further modifications may be required for the treatment of this complex patient subgroup. 1 Because heterotaxy syndrome includes a wide range of anatomical variants, the strategy for treating these patients is complicated. The purpose of this study was to review our recent patients with heterotaxy syndrome who underwent surgical repair, and determine potential problems to improve future outcomes.
Patients and Methods
Between April 1996 and November 2004, 27 patients with visceral heterotaxy were admitted to our institution and underwent surgery. There were 14 males and 13 females. The study was approved by the Ethical Committee at the University of Tokyo Hospital. Eleven patients were assigned to the asplenia group and 16 to the polysplenia group according to echocardiography and surgical findings. Medical records including the surgical report, echocardiography report, and cardiac catheterization data were retrospectively reviewed. The following data were retrieved and entered as covariates in the Cox regression model to determine risk factors for mortality: demographic data including age at presentation and sex; morphological variables including nonconfluent pulmonary arteries (PAs), pulmonary atresia/stenosis, atrioventricular (AV) valve regurgitation, number of ventricles, morphology of the main ventricular chamber, aortic arch obstruction and/or anomalies, type of pulmonary venous drainage and presence of pulmonary venous obstruction; and hemodynamic data including oxygen saturation at presentation. Other data retrieved were the type of surgical intervention and the outcome; for patients who died, the age at death and cause of death; and for survivors, their further management and follow-up duration.
Results are expressed as mean ± standard error of mean, unless otherwise specified. The survival was analyzed by Kaplan-Meier actuarial survival analysis and patient groups were compared by log rank test. The independent effects of demographic, morphological, hemodynamic variables on survival were analyzed by the Cox regression model. Probability analyses were performed using SPSS version 9.0 (SPSS Inc, Chicago, IL, USA).
Results
The median age at presentation was 25 days (range, 1 day to 9 years). Median follow-up time was 30.5 months. Fourteen patients presented in the neonatal period. One patient who had asplenia syndrome died from severe cyanosis before surgery and the other 26 underwent surgery. Of 11 patients with asplenia, 3 had nonconfluent PAs, 9 had more severe pulmonary stenosis or pulmonary atresia. Although 3 patients had 2 ventricles with an unbalanced AV canal defect and hypoplastic ventricle, all patients were scheduled for single-ventricle repair. Complete AV canal defect was seen in 4 patients and moderate or greater AV valve regurgitation was found in 5 during follow-up. Two patients underwent AV or mitral valvuloplasty. Only one patient with multiple AV valvuloplasty survived. TAPVC was seen in 4 patients. In polysplenia syndrome, 9 of the 16 patients had 2 ventricles. Moderate or greater AV valve regurgitation was seen in 4 patients and 2 had TAPVC (Table 1). One patient underwent tricuspid annuloplasty and another had AV valve replacement. Another 2 patients have improved AV valve regurgitation during follow-up.
Associated Anomalies in 27 Patients with Visceral Heterotaxy
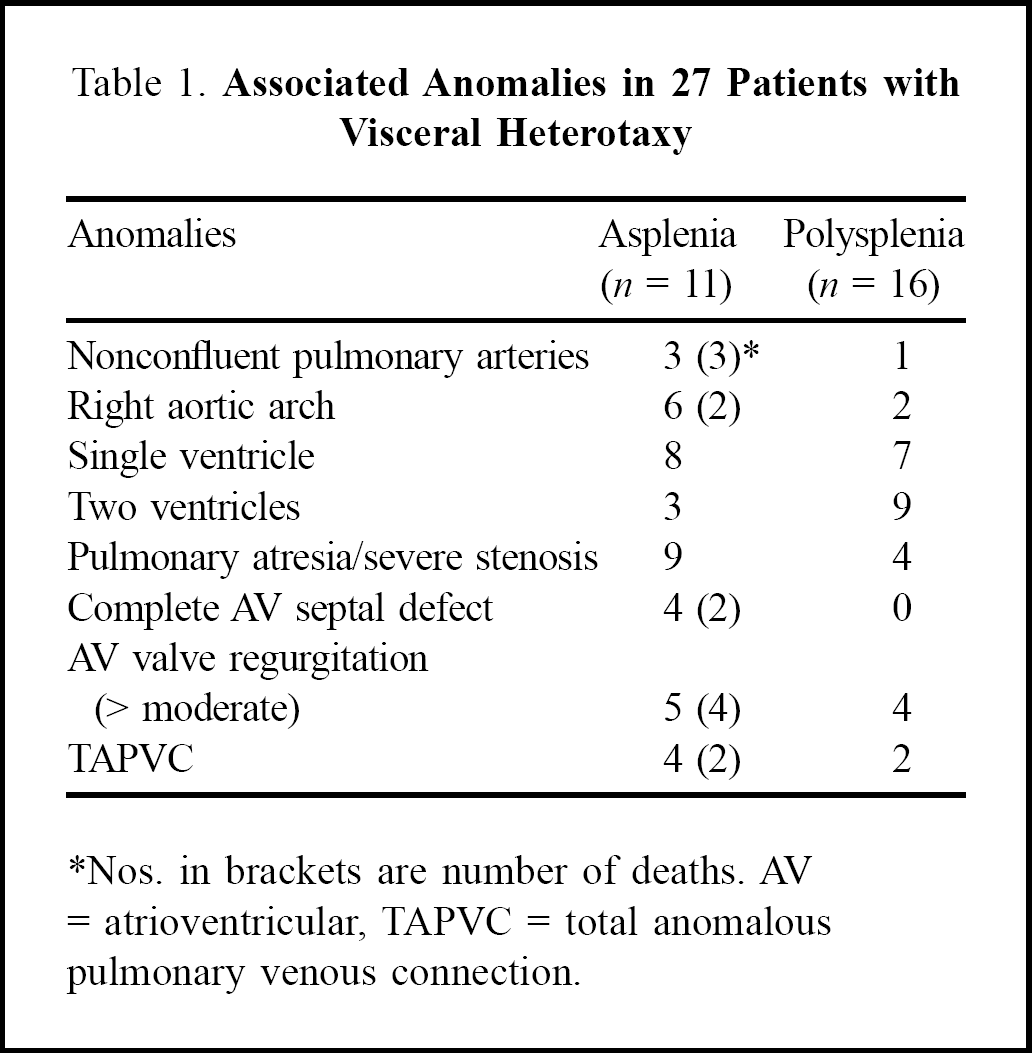
Nos. in brackets are number of deaths. AV = atrioventricular, TAPVC = total anomalous pulmonary venous connection.
The first palliative operations were a modified Blalock-Taussig (B-T) shunt in 6 patients, and TAPVC repair with PA banding, TAPVC repair with a modified B-T shunt, PA banding, and unifocalization plus modified B-T shunt in one patient each. Four deaths occurred postoperatively in this group. Two patients who had a modified B-T shunt with and without unifocalization died after surgery from sustained cyanosis. Both patients had patent shunts and one had severe AV valve regurgitation. High pulmonary vascular resistance might be related to cyanosis. In one patient with nonconfluent PAs, a unilateral B-T shunt was created at the initial operation, because she had a patent ductus arteriosus without prostaglandin. She developed desaturation after unifocalization and required a central shunt and left PA plasty at a second operation at 6 months of age. Another patient with nonconfluent PAs had multiple gastrointestinal problems (esophageal hiatus hernia, gastroesophageal reflux, malrotation of the intestine, and anal atresia) that were repaired at 3 days old, underwent unifocalization and a right modified B-T shunt (3 mm) simultaneously. Cardiac catheterization showed poor development of the PAs (PA index: 104 mm2·m−2) and unobstructed TAPVC (cardiac type) at 6 months after unifocalization and a B-T shunt. He developed progressive desaturation in the next few days and died before surgery. Another patient with AV valve repair after multiple B-T shunts died from pulmonary infection with pulmonary hypertension. Another patient with single ventricle, pulmonary atresia, dextrocardia, and infracardiac TAPVC underwent a left modified B-T shunt and TAPVC repair at 17-days old, and developed pulmonary venous obstruction 2 months later. She was taken to the operating room for possible surgical repair and developed myocardial infarction during dissection around the heart, although no significant abnormality of the coronary arteries had been detected by echocardiography. She required extracorporeal membrane oxygenator support for her low cardiac output syndrome postoperatively but developed mediastinitis and sepsis and died on the 15th postoperative day.
Three patients required an additional systemic-to-pulmonary shunt and 5 completed a bidirectional Glenn procedure as a step to a Fontan or modified Fontan operation (Figure 1). There were 6 patients with TAPVC: 4 in the asplenia group (2 supracardiac, 1 cardiac, 1 infracardiac) and 2 in the polysplenia group (both cardiac). Two patients underwent TAPVC repair: in addition to one described above, another patient who had mitral atresia, single right ventricle, severe pulmonary stenosis and TAPVC underwent TAPVC repair and PA banding. Nine months later, she had a right modified B-T shunt followed by a bidirectional Glenn procedure and common AV valve repair; she completed a modified Fontan operation. Five patients completed total cavopulmonary connection with only one fenestration. Fenestration used to be indicated only for high-risk Fontan candidates, but it has been preferred for all patients not only with heterotaxy syndrome, but also with other single-ventricle physiology.
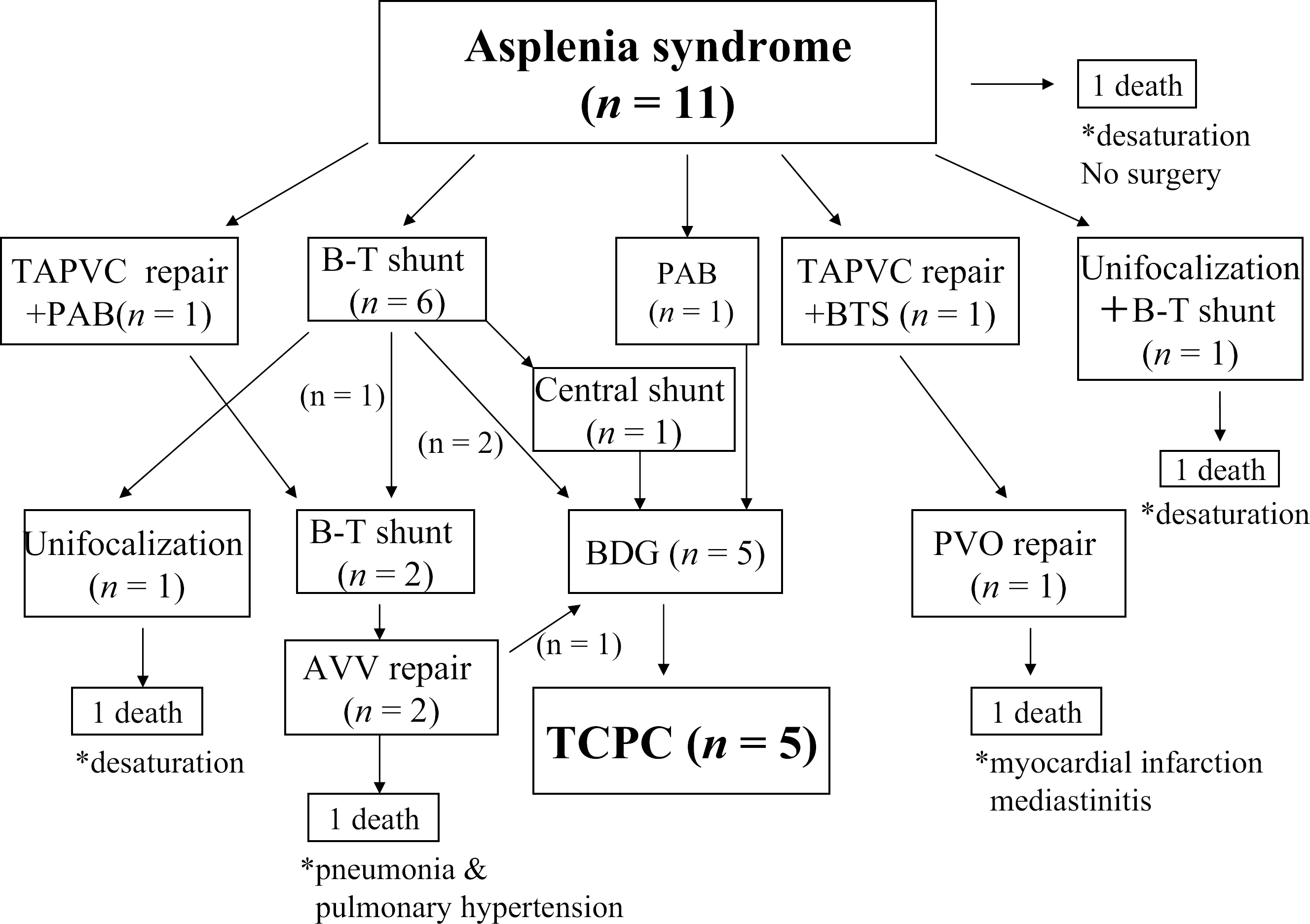
Surgical interventions in 11 patients of asplenia syndrome. BDG = bidirectional Glenn, B-T = Blalock-Taussig, PAB = pulmonary artery banding, PVO = pulmonary venous obstruction, TAPVC = total anomalous pulmonary venous connection, TCPC = total cavopulmonary connection.
In the polysplenia group, each 8 patients underwent single- or biventricular repair. In the single-ventricle repair subgroup, the first palliations were a modified B-T shunt in 4, PA banding in 3, and a modified B-T shunt with PA plasty in 1. One patient died after a modified BT shunt with PA plasty followed by a central shunt, because of pneumonia. One patient with nonconfluent PAs had bilateral B-T shunts in separate operations and a left pneumonectomy for a lung abscess. Because of his low saturation, he had a central shunt, which caused aggravation of his AV valve regurgitation, so he underwent tricuspid valvuloplasty in a further operation. This patient remains in a pre-Glenn state with a single lung and his saturation has been in the low 80s with reduced right ventricular function (right ventricular ejection fraction 38%–45%). Meticulous management may bring the chance of a bidirectional Glenn procedure in this patient. Six of these 8 patients have completed the modified Fontan operation. One patient underwent multiple systemic-to-pulmonary shunts and remains a candidate for a bidirectional Glenn procedure or modified Fontan operation (Figure 2). Among 8 patients with 2-ventricle repair, 4 underwent primary repair and 4 had PA banding with or without patent ductus arteriosus ligation, and then underwent surgical correction (Figure 3).
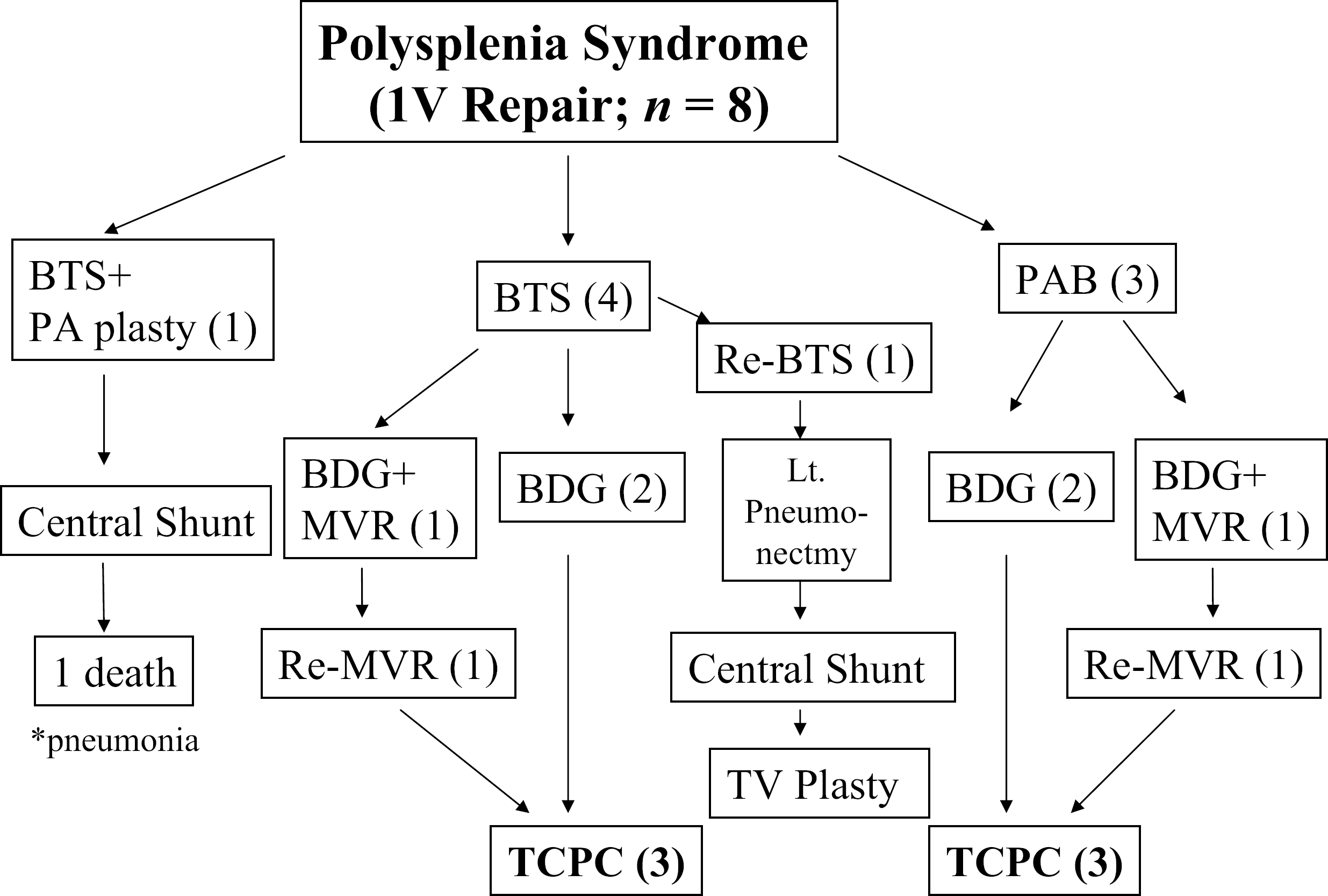
Surgical interventions in 8 patients intended for single-ventricle repair with polysplenia syndrome. BDG = bidirectional Glenn, BTS = Blalock-Taussig shunt, MVR = mitral valve replacement, PAB = pulmonary artery banding, TAPVC = total anomalous pulmonary venous connection, TCPC = total cavo pulmonary connection, TV = tricuspid valve.
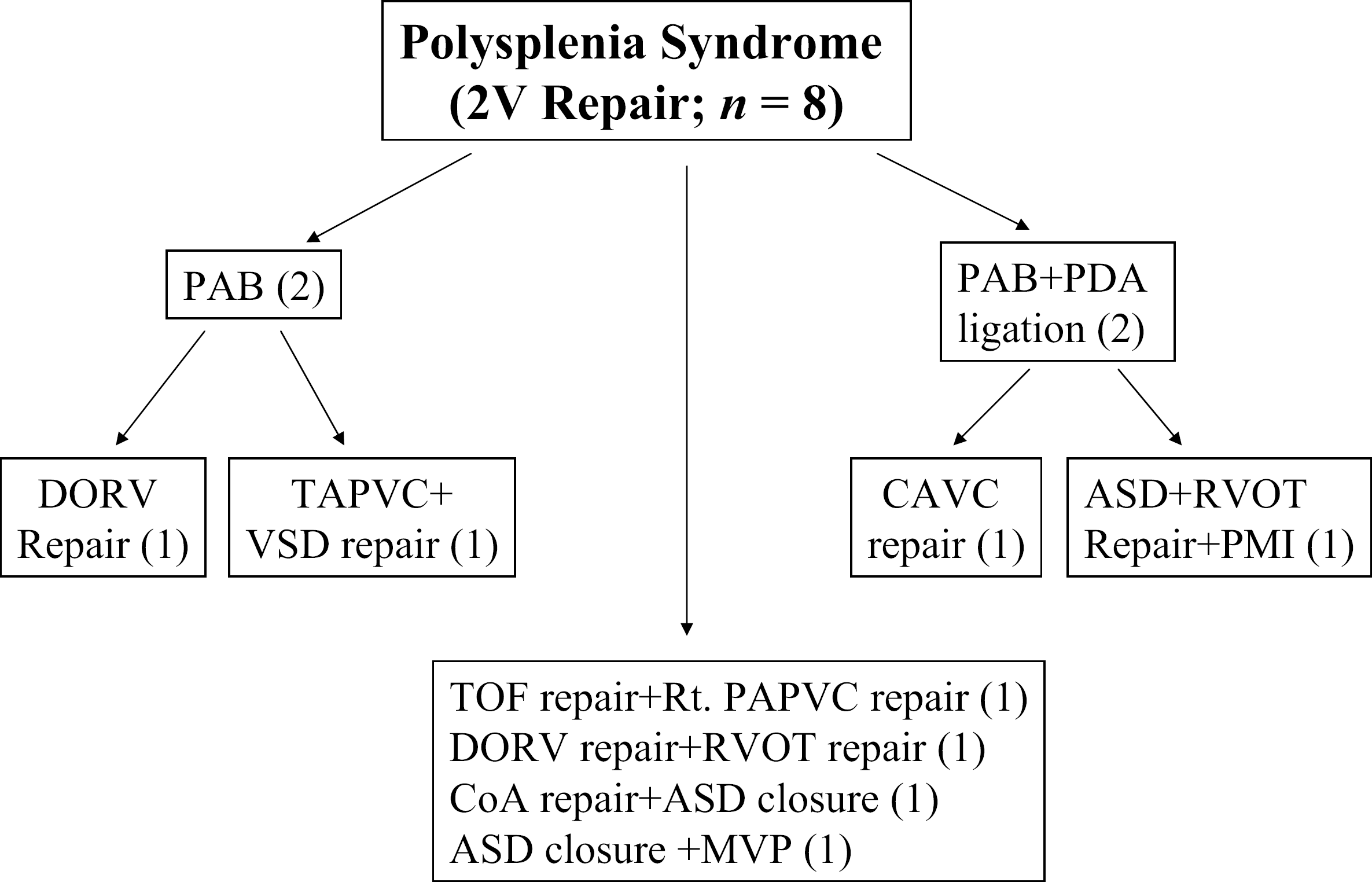
Surgical procedures in patients with polysplenia syndrome intended for 2 ventricle repair. ASD = atrial septal defect, CAVC = complete AV canal defect, CoA = coarctation of aorta, DORV = double-outlet right ventricle, MVP = mitral valve plasty, PAB = pulmonary artery banding, PAPVC = partial anomalous pulmonary venous connection, PDA = patent ductus arteriosus, PMI = pace maker implantation, RVOT = right ventricular outflow tract, TAPVC = total anomalous pulmonary venous connection.
Actuarial overall survival estimated by the Kaplan-Meier method was 96.3% with a 95% confidence interval (CI) of 92.7%–99.9% at 1 month, 81.5% (95%CI 74.0%–89.0%) at 6 months, and 77.4% (95%CI 69.3%–85.6%) at 1 year. In patients with polysplenia, actuarial Kaplan-Meier survival was 93.8% (95%CI 87.7%–99.8%) at 4 months, and then remained constant. On the other hand, in patients with asplenia, actuarial survival was 81.8% (95%CI 70.2%–93.5) at 1 month, 63.6% (95%CI 49.1%–78.1) at 6 months, and 53.0% (95%CI 37.5%–68.5) at 1 year. Although there was no independent risk factor determined by Cox regression analysis, a significant correlation was found between nonconfluent PAs and mortality (correlation coefficient 0.671; p < 0.05).
Discussion
This study found the short-term surgical outcome in infants and children with asplenia syndrome remains unfavorable despite an excellent surgical outcome in patients with polysplenia syndrome. Poor growth of the pulmonary vascular tree is relatively common in asplenia syndrome and often associated with nonconfluent PAs, which correlated significantly with a poor surgical outcome in this study. 2 Thus, the first palliation should be a systemic-to-pulmonary shunt in most cases. Our initial surgical strategy for nonconfluent PAs was to establish reasonable pulmonary blood flow in the unilateral lung by a systemic-to-pulmonary shunt to let the pulmonary vascular tree grow, and then create unifocalization of the PAs. Because of poor outcome, we changed our strategy from 2003 towards to create a systemic-to-pulmonary shunt and unifocalization simultaneously. Even with this modification, one patient died from progressive cyanosis. This patient had multiple problems in the gastrointestinal tract and might have been behind schedule for surgery to establish reasonable pulmonary blood flow. Another patient with polysplenia and nonconfluent PAs underwent multiple operations to establish a systemic-to-pulmonary shunt, remove his purulent lung, and reduce AV valve regurgitation after a central shunt. He developed left pulmonary venous obstruction followed by a left lung abscess and hemoptysis, and this led to a left pneumonectomy. Although his management is very critical, he might be able to undergo a bidirectional Glenn procedure in the near future.
The timing of TAPVC repair is very important in single ventricle. Previous reports have suggested that the association of TAPVC with single ventricle, particularly in patients with heterotaxy syndrome, is a risk factor for poor outcome. 3 –5 In a recent report from Boston on 123 patients with TAPVC, actuarial survival was 65% at 1 month and 47% at 36 months for single ventricle; single ventricle had a 4.8-time higher risk of mortality compared with 2-ventricle repair. Pre-repair pulmonary venous obstruction was found to be a risk factor in multivariate analysis. 6 Gaynor and colleagues 7 suggested that factors influencing survival of patients with heterotaxy syndrome undergoing the Fontan procedure included > mild AV valve regurgitation, hypoplastic PAs, and high PA pressure (> 15 mm Hg) after 6 months of age. Survival rates of 54% at 6 months of age, 44% at 1 year, and 23% at 5 years were reported, and they postulated that inadequate development of the pulmonary vasculature, especially the pulmonary veins, occurring even in children without clinical evidence of pulmonary venous obstruction, resulted in high early mortality and a continuing risk of late death. In another report from Boston, neither the presence of TAPVC nor TAPVC repair was found to be a definite risk factor for early death in newborns with visceral heterotaxy. 8 However, mortality was very high in TAPVC with obstruction (41.7%; 5/12 patients). Improving results of the modified Fontan operation in patients with heterotaxy syndrome has been reported. 1
Patients with asplenia syndrome have a worse survival rate than those with polysplenia (64% vs 99.4%). Actuarial survival for patients with asplenia was 81.8% (95%CI, 70.2%–93.5%) at 1 month, 63.6% (95%CI, 49.1%–78.1%) at 6 months and 53.0% (95%CI, 37.5%–68.5%) at 1 year. This is similar to the results from Toronto: of 91 patients with asplenia syndrome, 68 (75%) underwent surgery, overall estimated survival was 71% at 1 month, 49% at 1 year, and 35% at 5 years. 9 Independent risk factors for early death included the absence of pulmonary outflow obstruction, a major AV valve anomaly, and obstructed pulmonary veins. 9 Even in patients with asplenia syndrome and normal pulmonary venous drainage, an unfavorable long-term outcome has been reported. 10
In patients with polysplenia syndrome, overall estimated survival was excellent in this study. The fact that many patients can undergo biventricular repair in polysplenia syndrome may be the reason for a better outcome than those with asplenia. 11,12 However, a large retrospective review of polysplenia syndrome from Toronto showed that 71 of 163 patients were suitable for biventricular repair and another 70 for single ventricular repair, but survival remained unsatisfactory: 80% at 1 year, 71% at 5 years, 66% at 10 years in the 2-ventricle group; and 73% at 1 year, 61% at 5 years, 53% at 10 years in the single-ventricle group. Independent factors associated with time-related death included congenital AV block, aortic coarctation, and single ventricle. 13 Again, these risk factors are very different from those in patients with asplenia syndrome.
Nine patients developed AV valve regurgitation; 4 of 5 with asplenia syndrome died, and 2 with polysplenia had spontaneous improvement of AV valve regurgitation. A systemic-to-pulmonary shunt is known to cause volume overload and aggravation of AV valve regurgitation. A relatively longer and wider shunt can be a risk factor for mortality in patients with single-ventricle physiology. 14 Indeed, an additional shunt was frequently required and AV valve regurgitation was common in patients with asplenia. Even with multiple surgical interventions for valve regurgitation, the outcome was not satisfactory in this study and in others. 15 In our institution, the indication for AV valve repair before a Fontan operation is moderate or greater AV valve regurgitation. An important strategy may not be changing this indication for AV valve repair, but reducing the source of volume overload by adjusting the shunt size and position.
Eight patients underwent biventricular repair in this study, and half of them required PA banding as initial palliation. Biventricular repair is possible in some cases of heterotaxy syndrome, although intracardiac anatomy varies from one side to the other. 16,17 In our study, no patient required a systemic-to-pulmonary shunt as a step to biventricular repair. This suggests that a fully developed pulmonary vascular tree and its associated conditions are very important for biventricular repair in heterotaxy syndrome.
Based on our data, we concluded that the early surgical result is satisfactory in patients with polysplenia, but not in those with asplenia and nonconfluent pulmonary arteries. Strategies to create confluence of both vascular beds and satisfactory pulmonary blood flow are mandatory early in the life of a patient with nonconfluent pulmonary arteries. This was a retrospective review with a small number of patients and relatively short follow-up; however, this study was carried out in a single institution with excellent follow-up, and it may provide some insight into the treatment of patients with heterotaxy syndrome.