
Abstract
Combined coronary bypass grafting and valve procedures for mitral valve regurgitation result in poor outcomes, but the impact of the etiology of valve regurgitation on operative and long-term outcomes is not well defined. A retrospective analysis of 468 patients who had combined coronary bypass grafting and valve operations for mitral regurgitation showed that 78% had valve repairs and 22% had replacements for ischemic (45%) or degenerative (55%) disease. Predictors of operative mortality were ischemic mitral regurgitation, failure to use the internal mammary artery for grafting, severe coronary disease, acute myocardial infarction, low ejection fraction, advanced heart failure, emergency operation, and mitral valve replacement. The 5-year survival rates for propensity-matched patients with ischemic or degenerative disease were similar (66%). Low ejection fraction (< 35%), advanced age (> 67 years), valve replacement surgery, residual mitral regurgitation, and severe coronary artery disease were predictors of poor long-term outcome. Although the operative outcomes of ischemic mitral regurgitation were poor compared to those of degenerative disease, the long-term survival was similar in both groups of propensity-matched patients. Left ventricular remodeling, an optimal valve procedure without residual mitral regurgitation, and left ventricular function are more important determinants of long-term outcome than the etiology of valve regurgitation.
Introduction
Mitral regurgitation (MR) in patients undergoing myocardial revascularization often results in a poor outcome. Shorter long-term survival is also expected after surgery for MR due to ischemic heart disease compared to MR in the absence of coronary artery disease. 1,2 The etiology of MR, New York Heart Association (NYHA) functional class, preoperative left ventricular (LV) function, and techniques utilized for correction of MR (valve repair or replacement) were found to be important determinants of long-term outcome. 3 –5 However, the influence of etiology of MR and valve procedures on outcomes after coronary artery bypass grafting (CABG) has yet to be clearly defined. To identify predictors of operative mortality and long-term outcomes, we conducted this study in patients with ischemic or degenerative disease who underwent CABG and concomitant valve operations for MR.
Patients and Methods
From July 1985 through June 2002, 1,687 mitral valve procedures were performed at Newark Beth Israel Medical Center. Our study group consisted of 468 patients who underwent a valve procedure for MR and simultaneous CABG; MR was due to degenerative disease in 253 (55%), and of ischemic origin in 215 (45%). We excluded patients having combined major cardiac operations such as arrhythmia ablation, aortic valve repair or replacement, repair of post-infarction ventricular septal defect or ventricular aneurysm, mitral valve procedures for infarcted and ruptured papillary muscles following acute myocardial infarction (MI), and those with severely calcified mitral valves (rheumatic origin) and calcified annulus. Outcome differences in 2 time periods were analyzed: July 1985 through June 1992, and July 1992 through June 2002. Patients’ hospital charts, preoperative cardiac catheterization data, and echocardiographic reports were reviewed. The Institutional Review Board of Newark Beth Israel Medical Center approved this investigation.
The etiology of MR was determined by the patient's clinical history, echocardiographic findings, and observations on the operating table. The diagnosis of MR was established after the agreement of 2 expert echocardiographers. Histological examination of resected leaflet tissue confirmed the diagnosis. The patients were classified on the basis of etiology of MR (ischemic or degenerative disease) and technique of correction (valve repair or prosthetic valve replacement). Patients in the ischemic group were older and more predominantly female than those with degenerative disease, with increased incidences of hypertension, diabetes, renal dysfunction, 3-vessel coronary artery disease, and acute MI, and more likely to be in NYHA class III—IV with Canadian Cardiovascular Society class III symptoms (Table 1). This group also had more emergency operations, more bypass grafts per patient, fewer internal mammary artery grafts, and longer cardiopulmonary bypass times than patients with degenerative disease. An equal percentage (22%) of patients with ischemic and degenerative disease had valve replacements. Patients who had prosthetic valve replacement rather than valve repair had a greater incidence of diabetes, hypertension, 3-vessel coronary disease, and more of them presented with acute MI and NYHA class III—IV symptoms. This group also had more emergency operations, fewer internal mammary artery grafts, and longer cross clamp and cardiopulmonary bypass times (Table 1). During valve replacement, attempts were made to preserve the posterior leaflet in 60 (58%) patients, the anterior leaflet in 6 (6%), and both leaflets in 2 (2%). 6 Preoperative tricuspid regurgitation ≥ grade 2+ was repaired. Failed repair was defined as the need for redo valve surgery or recurrent MR ≥ grade II.
Characteristics of 468 Patients Undergoing Mitral Valve and Coronary Bypass Procedures
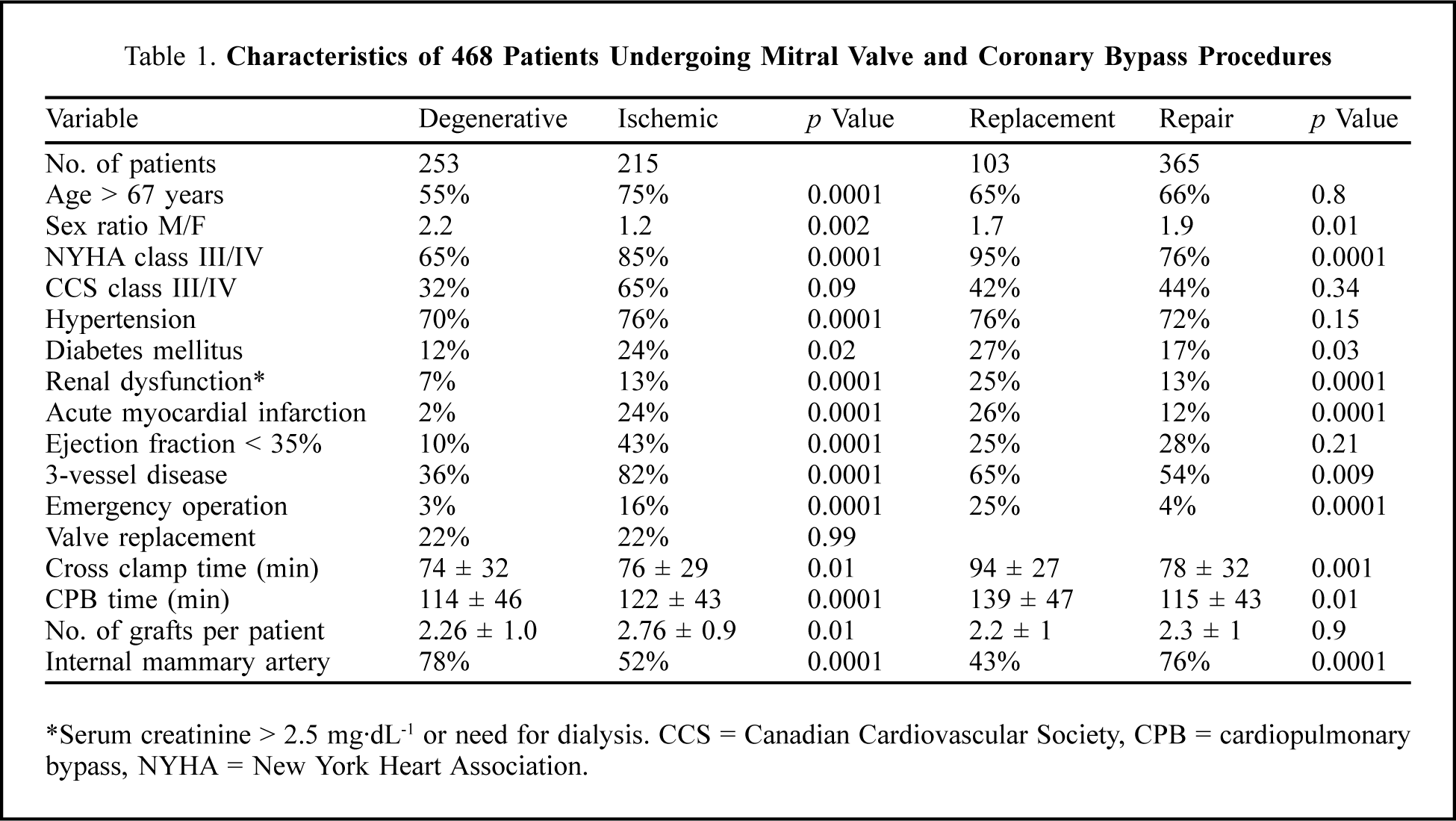
Serum creatinine > 2.5 mg·dL−1 or need for dialysis. CCS = Canadian Cardiovascular Society, CPB = cardiopulmonary bypass, NYHA = New York Heart Association.
All patients with ischemic mitral valve disease had one or more prior MI, mostly inferior, with associated regional wall motion abnormalities. 7 In ischemic MR, the regurgitant jet is central when valve leaflets, chordae, and papillary muscles are normal. The leaflets failed to coapt or there was restricted mobility of the leaflets (Carpentier type IIIb) with annular dilatation in all 215 patients with ischemic MR, of whom 168 (78%) had valve repairs. A simple repair technique of annuloplasty alone was performed in 88% (posterior ring in 72%, commissural in 22%, and full ring in 6%). Complex repair techniques included annuloplasty combined with leaflet and chordal procedures in 12% (leaflet resection in 8%, commissural resection in 2%, bileaflet repair in 2%, and shortening of chordae in 2%). In no patient was an undersized mitral ring used. Valve replacement was carried out in 47 patients (22%) for annular enlargement, without or with papillary muscle dysfunction (40%).
In patients with degenerative mitral valve disease, the regurgitant jet was non-central or peripheral and the leaflets were floppy and thickened with elongated or ruptured chordae tendineae. In some patients with annular dilatation but no discernible leaflet prolapse, thick billowing of the valve leaflets was noted. Leaflet prolapse was the most common finding (posterior 86%, anterior 50%, bileaflet prolapse 35%). Chordal elongation and/or rupture were observed in 62% of patients. Valve repairs in 197 (78%) patients with degenerative MR included leaflet plication or quadrangular resection of the posterior leaflet, supplemented by annuloplasty (60%), leaflet transposition (11%), commissural leaflet resection (6%), bileaflet repairs (31%), chordal procedures (13%), or annuloplasty alone (9%). The repair was simple (136 patients) when it involved annuloplasty with or without leaflet resection or plication, and complex (61 patients) when there was chordal, anterior leaflet, or bileaflet repair. Valve replacements were undertaken in 56 (22%) patients, mostly for bileaflet prolapse (67%) and chordal rupture (55%).
Intraoperative echocardiograms were analyzed in 48% of valve repairs and 20% of valve replacements. Transesophageal echocardiograms supplemented preoperative transthoracic echocardiographic studies when needed. After discharge from the hospital, most patients were followed up as outpatients, and the records of subsequent hospital admissions were reviewed. For those not seen as an outpatient, telephone contact was made with the patient, their family, the referring physician and/or cardiologist. The NYHA functional class, valve-related complications (thromboembolism, anticoagulant-related hemorrhage, recurrent MR) and other significant clinical events were noted. Echocardiograms were obtained on hospital discharge in 384 (82%) patients, but this evaluation was complete in only 67% during follow-up. Follow-up ranged from 3 to 246 months (median, 9.2 years), and 20% of patients were followed up for 16 years or more. The time of the last follow-up echocardiogram ranged from 32 days to 17.9 years (median, 7.6 years).
All statistical analysis was performed using SAS software (SAS Institute, Cary, NC, USA). Univariate analyses included two-tailed Wilcoxon rank sum or t tests for continuous variables and chi-squared or Fisher's exact tests for discrete variables. A p value ≤ 0.05 was considered significant. New York Heart Association functional class III/IV symptoms and patient survival was estimated by the Kaplan-Meier technique, with log-rank tests to compare stratified groups. The important influencing variables or risks were analyzed by univariate and multivariate Cox proportional hazard models, and expressed as risk ratios with 95% confidence intervals (CI). Propensity scoring was carried out to match patients with degenerative and ischemic MR to compare long-term survival. A saturated model was used in propensity analysis. Variables that were not significant in the logistic regression analysis (diabetes mellitus, hypercholesterolemia, family history of coronary artery disease, history of MI, congestive heart failure, stable vs unstable angina, LV ejection fraction, peripheral vascular disease, prior cerebrovascular accident, pulmonary hypertension, chronic obstructive pulmonary disease, chronic renal insufficiency, and current dialysis requirement) were added to significant variables (age, smoking history, hypertension, other comorbidity, extent of coronary disease, ventricular dysfunction, NYHA functional class III and IV, several clinical factors, preoperative intra-aortic balloon counterpulsation, grade of preoperative MR, elective or emergency operations, and valve repair or replacement) in a logistic regression analysis yielding a model with 70 variables. Using the significant regression coefficients, a propensity score was calculated, which matched 117 pairs of patients with degenerative and ischemic MR. The characteristics of these propensity-matched patients are shown in Table 2.
Patient Characteristics of 117 Propensity-Matched Pairs
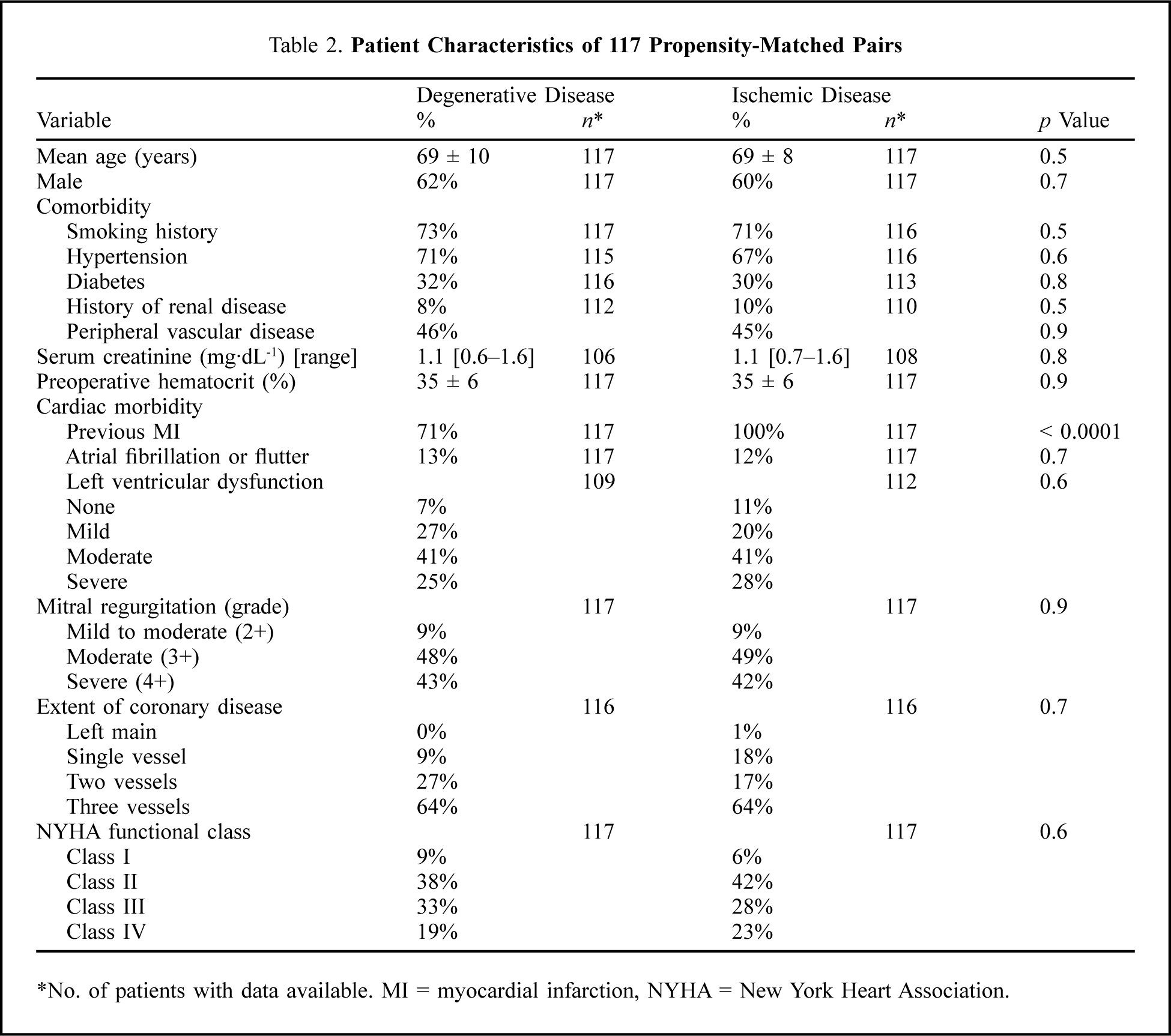
No. of patients with data available. MI = myocardial infarction, NYHA = New York Heart Association.
Results
There were 39 hospital deaths (within 30 days of operation or during the same hospitalization); the overall mortality rate was 8.3%. Hospital mortality during the earlier period of the study (1985 to 1992) was 12% compared to 5% in the more recent phase (1992 to 2002). During the early period, emergency surgery was more common (13% of 212 cases vs 5.5% of 256 later cases), the internal mammary artery was used less frequently (49% vs 80%), and valve repairs were carried out in 71% vs 84%. The percentage of patients undergoing surgery early after MI was similar in both periods (12% vs 12.5%). The hospital mortality was higher for ischemic disease than for degenerative disease, and mortality after prosthetic valve replacement was higher than that after valve repair (Table 3). There was more major operative morbidity in the ischemic group than the degenerative group, and valve replacement was associated with more complications than valve repair. The median length of hospital stay for the entire cohort was 10 days, and median intensive care unit stay was 3 days.
Postoperative Complications in 468 Patients
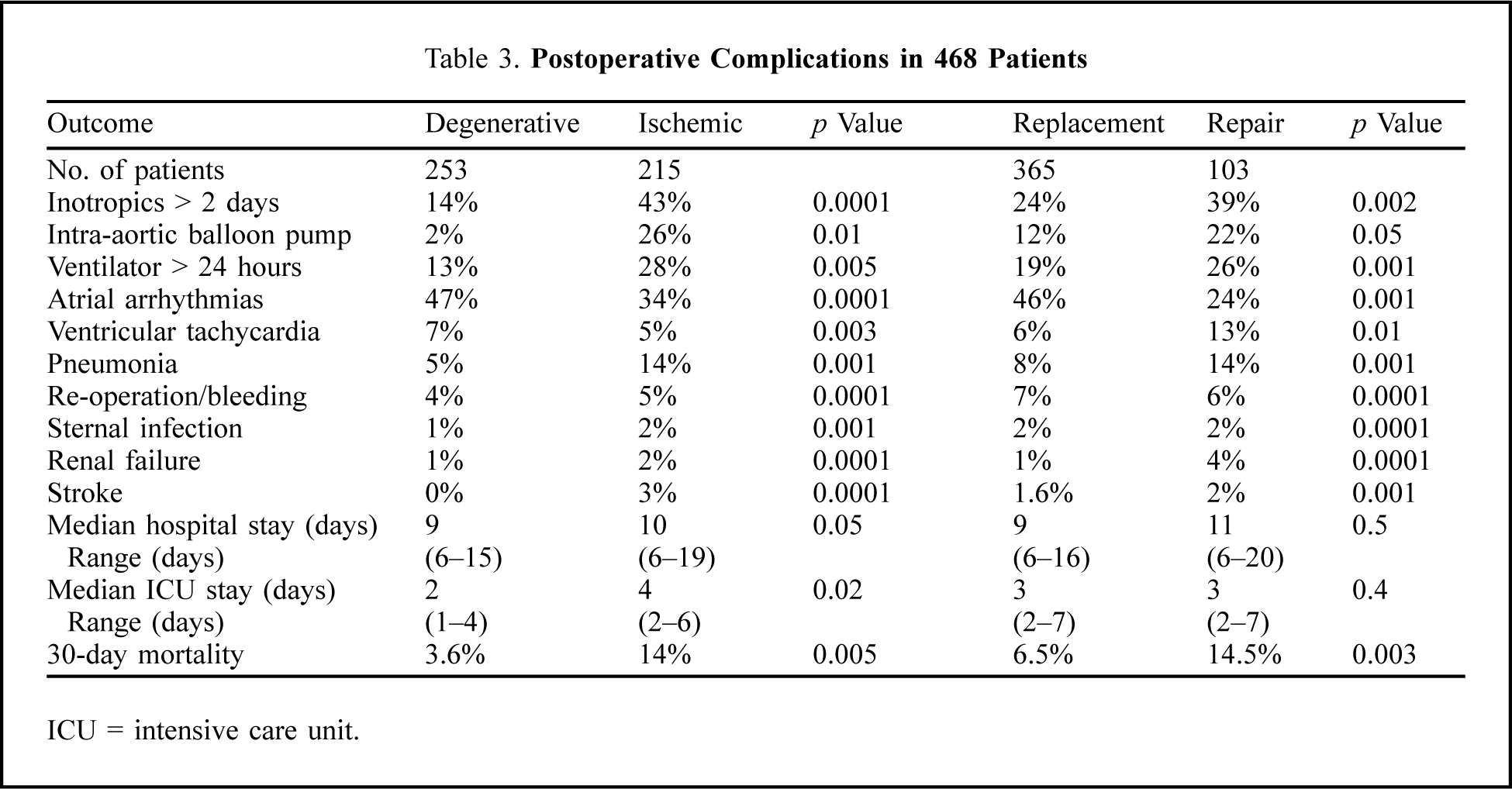
ICU = intensive care unit.
The predictors of 30-day mortality by univariate analysis included NYHA class III/IV symptoms, significant preoperative right ventricular dysfunction (mean pulmonary artery pressure > 45 mm Hg ± tricuspid regurgitation ≥ grade II), emergency operation, 3-vessel coronary disease, acute MI, low ejection fraction, ischemic MR, valve replacement, renal failure, failure to use the internal mammary artery as a bypass graft, and surgery during the earlier period which was characterized by more emergency operations, less frequent use of internal mammary artery grafts, and fewer valve repairs (Table 4).
Predictors of 30-day Mortality (Univariate Analysis)
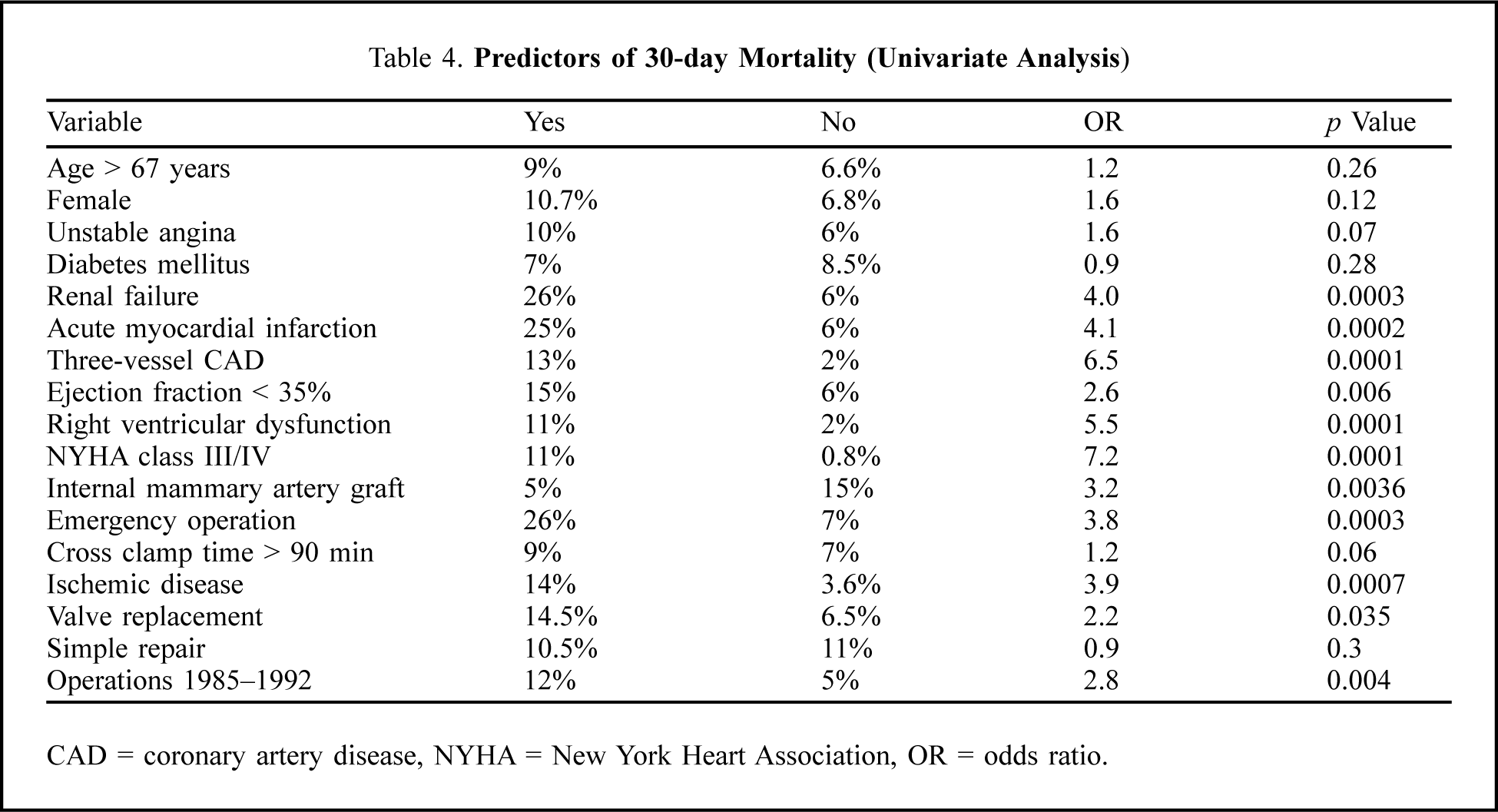
CAD = coronary artery disease, NYHA = New York Heart Association, OR = odds ratio.
Overall survival at 5 and 10 years was 73% (95% CI: 65%–76%) and 52% (95% CI: 42%–56%), respectively (Figure 1A), but freedom from congestive heart failure (CHF) was 63% (95% CI: 54%–66%) at 5 years, and only 39% (95% CI: 26%–42%) at 10 years (Figure 1B). The 5 and 10-year survival rates in the early (1985–1992) vs recent phases (1992–2002) were 67% and 44% vs 72% and 48% (p = 0.06), respectively. Patients > 67-years old had poor survival compared to those aged ≤ 67 years (62% vs 78% at 5 years, 54% vs 37% at 10 years; p ≤ 0.0001). Acute MI perioperatively had no influence on long-term survival (60% and 42% vs 69% and 45% at 5 and 10 years, respectively (p = 0.09). Lower survival rates were associated with preoperative NYHA class III—IV (Figure 2A), diminished LV function (Figure 2B), 3-vessel coronary artery disease (Figure 2C), valve replacement (Figure 2D), and right ventricular dysfunction (Figure 2E). Survival was worse for ischemic MR compared to degenerative MR (67% [95% CI: 62%–74%] vs 83% [95% CI: 71%–86%] at 5 years; 47% [95% CI: 43%–55%] vs 62% [95% CI: 54%–72%] at 10 years; Figure 3A), but it was similar for propensity-matched patients (65% vs 66% at 5 years, and 46% vs 48% at 10 years; p = 0.23; Figure 3B).
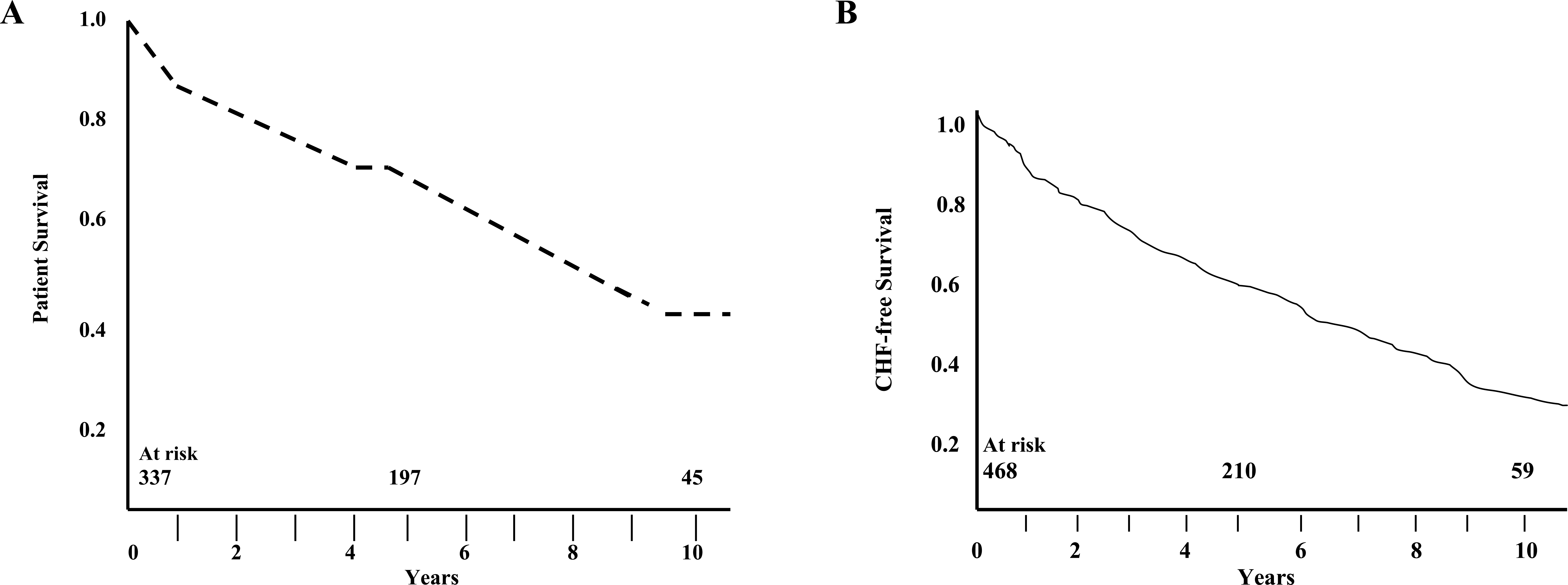
(A) Overall survival (Kaplan-Meier) of patients undergoing mitral valve repair or replacement plus coronary artery bypass. (B) Overall congestive heart failure (CHF)-free survival of patients undergoing mitral valve repair or replacement plus coronary artery bypass.
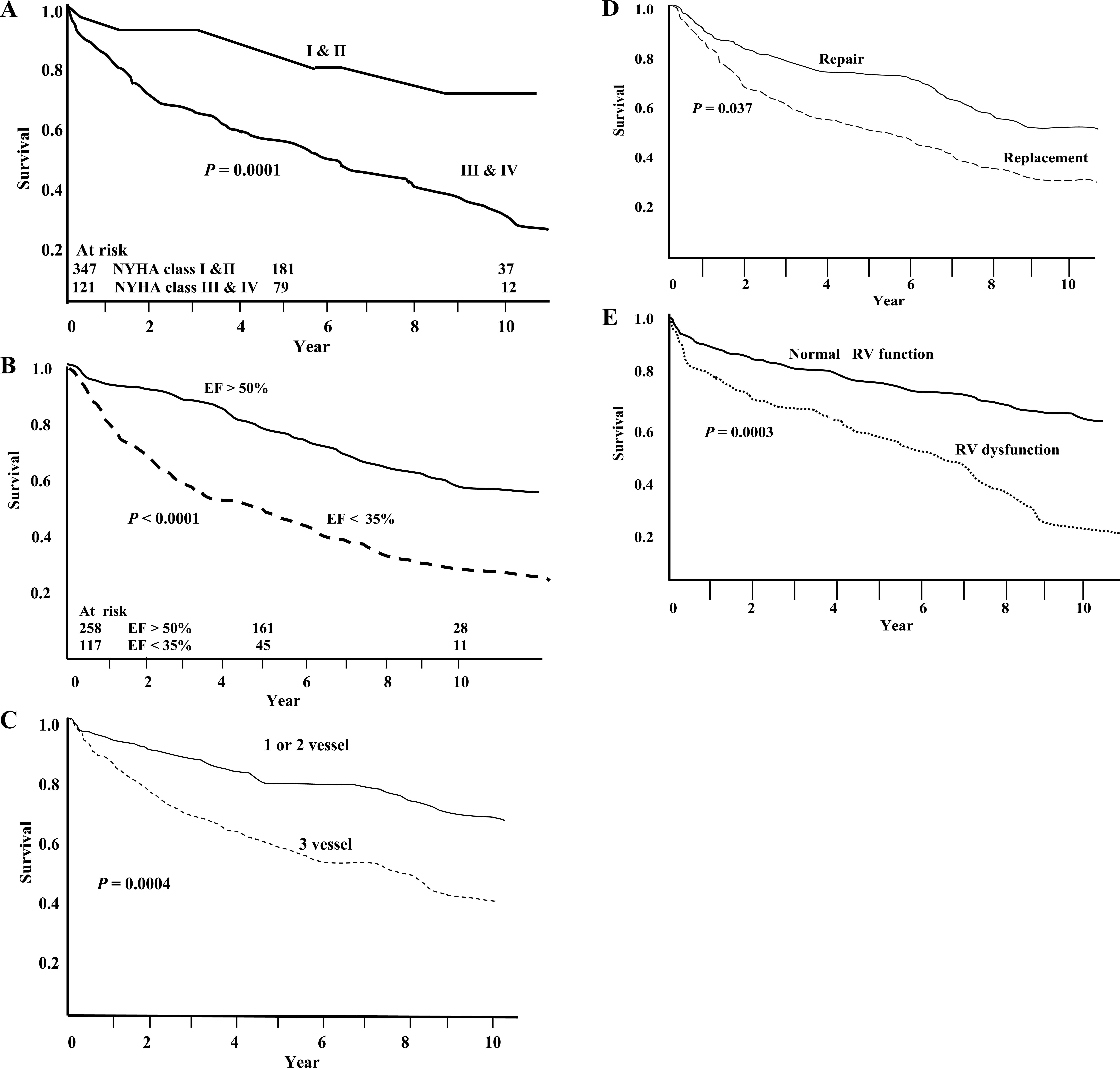
(A) Survival according to preoperative New York Heart Association functional class. (B) Survival according to preoperative left ventricular ejection fraction (EF). (C) Survival stratified by extent of coronary artery disease. (D) Survival based on valve repair or valve replacement. (E) Survival according to preoperative right ventricular (RV) function.
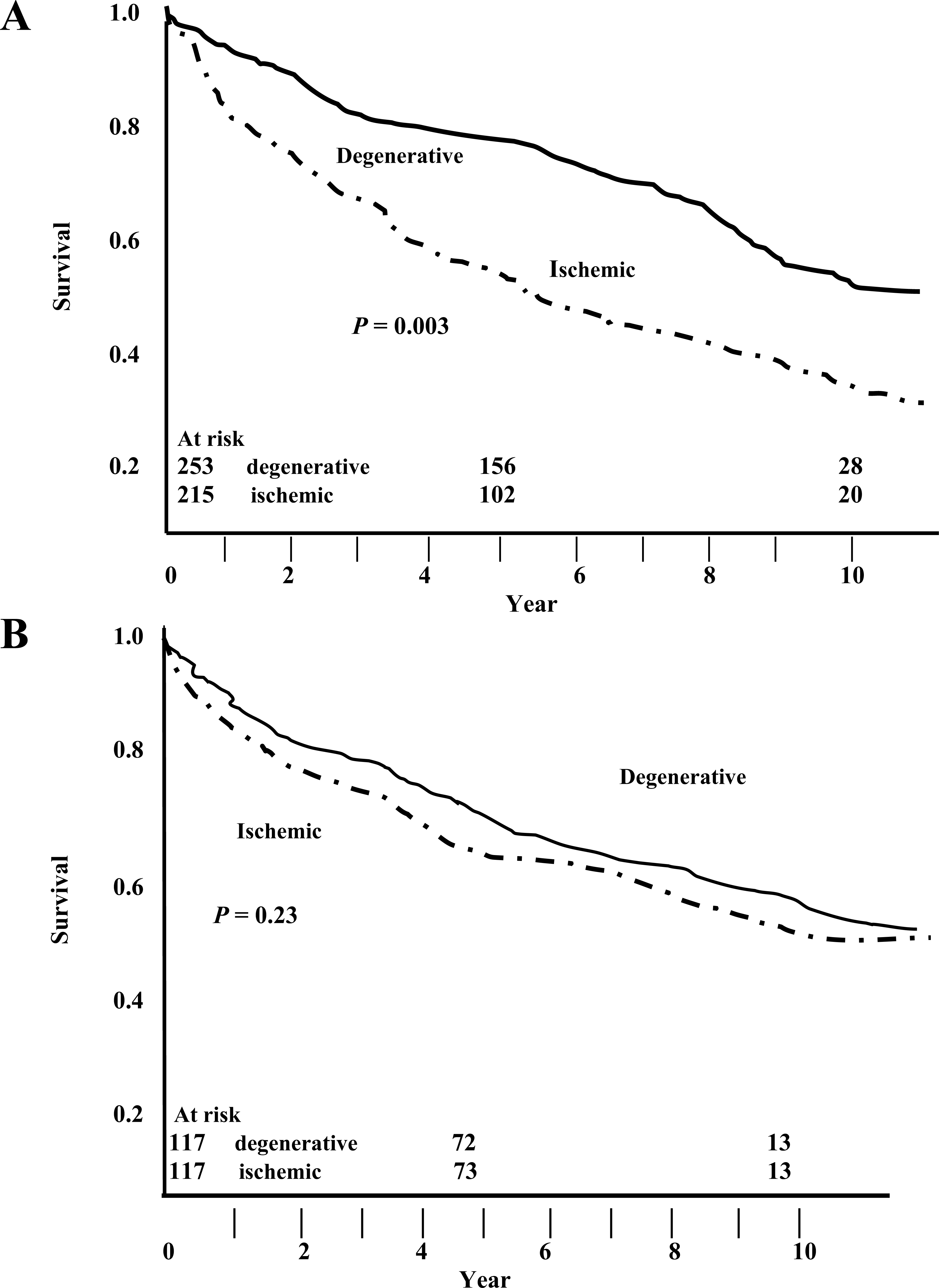
(A) Survival of 468 unmatched patients with degenerative or ischemic mitral regurgitation. (B) Survival of 117 pairs of propensity-matched patients with degenerative or ischemic disease.
The predictors of survival on univariate and multivariate analyses are shown in Table 5. The important independent predictors of poor long-term survival were residual MR (≥ grade II) at hospital discharge, 3-vessel coronary artery disease, reduced ventricular function, and valve replacement surgery, but not the etiology of MR.
Predictors of Long-Term Survival (Univariate and Multivariate Analyses)
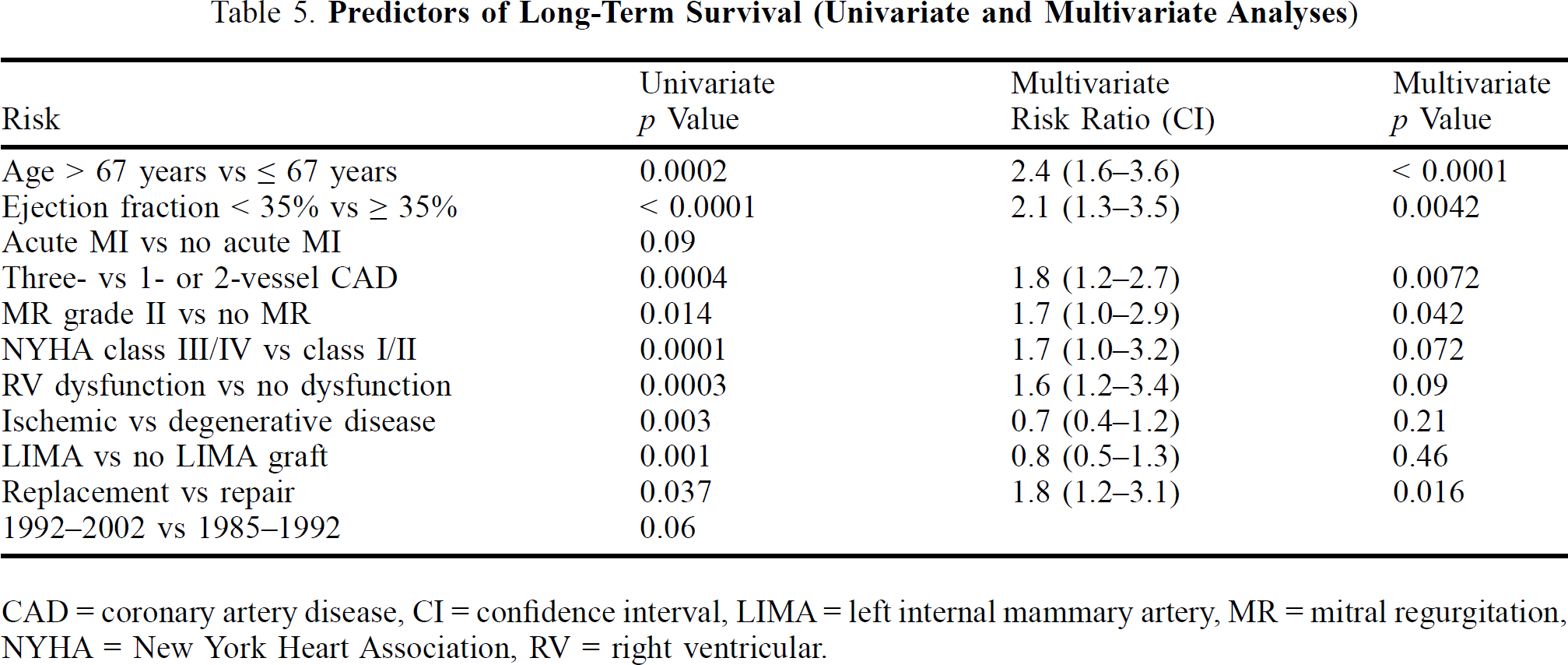
CAD = coronary artery disease, CI = confidence interval, LIMA = left internal mammary artery, MR = mitral regurgitation, NYHA = New York Heart Association, RV = right ventricular.
The cumulative risk of developing CHF was 22% (95% CI: 18%–32%) at 5 years, and 46% (95% CI: 38%–58%) at 10 years. Residual MR ≥ grade II was associated with increased incidence of CHF (Figure 4A) and decreased survival (Figure 4B). The independent predictors of CHF on long-term follow-up were residual MR ≥ grade II at hospital discharge, ejection fraction < 35% (p = 0.002), preoperative NYHA class III/IV symptoms (p = 0.014), and significant right ventricular dysfunction (p = 0.02)
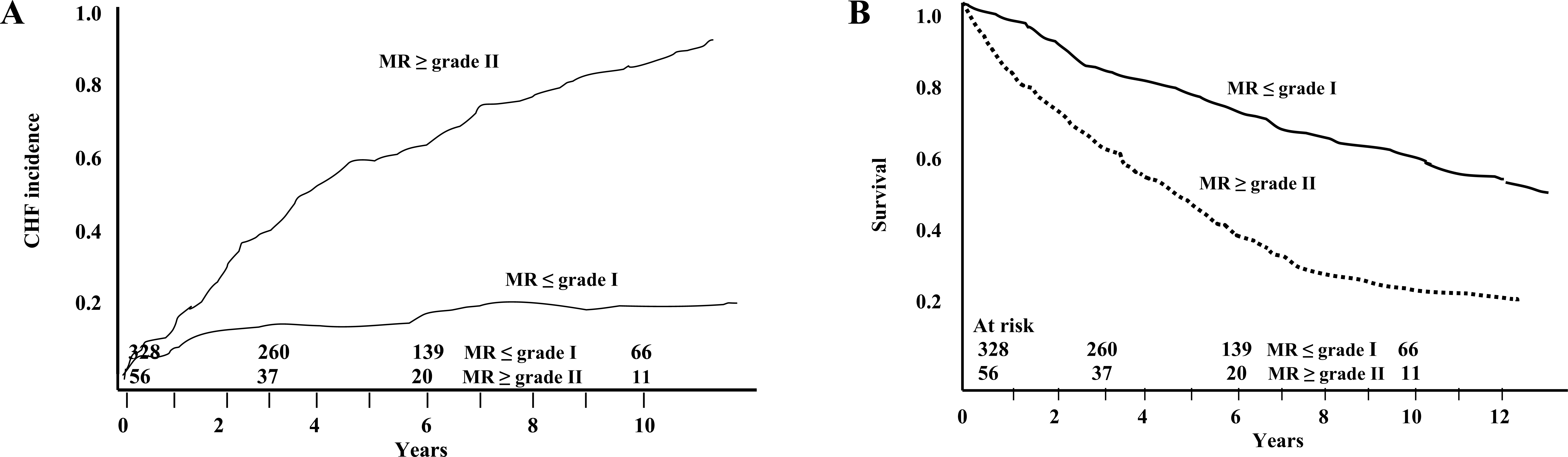
(A) Freedom from congestive heart failure (CHF) according to presence or absence of residual mitral regurgitation (MR) ≥ grade II at hospital discharge; (B) Survival according to presence or absence of residual MR ≥ grade II at hospital discharge.
Freedom from re-operation was 95% (95% CI: 87% to 98%) at 5 years and 87% (95% CI: 72% to 94%) at 10 years after valve repair, and 89% (95% CI: 75% to 99%) at 5 years and 78% (95% CI: 57% to 100%) at 10 years after valve replacement. The overall failure rate for simple repairs (degenerative and ischemic disease) was 14.5% (41 patients) compared to 18.5% for complex repairs (15 patients). In degenerative disease, valve repair failure was less common, and the failure rates for simple and complex valve repairs were similar (6% vs 5%). In ischemic disease, the failure rates for simple and complex valve repairs were 21.6% and 60%, respectively; and 5 of 20 patients (25%) with complex valve repairs required valve replacement.
Discussion
The LV remodeling that occurs as a consequence of MI results in dilatation of the mitral annulus with incomplete coaptation of the valve leaflets and/or displacement of papillary muscles with restricted motion of the valve leaflets, both of which produce MR in ischemic disease. 8,9 The novel techniques of infarct restraint, ventricular reconstruction, Paneth suture annuloplasty, and chordal transection were not established in clinical practice for correction of ischemic valvular dysfunction in this study. Mitral valve annuloplasty was employed to correct ischemic MR, whereas several leaflet procedures combined with annuloplasty were performed to correct MR in degenerative disease.
The determinants of operative risk and poor long-term survival after surgery for MR and CABG noted in this study are consistent with those of other reports. 7,10 However, ischemic etiology of MR was not found to be an independent predictor of long-term survival. The equally poor long-term outcomes after degenerative and ischemic MR surgery in matched patients suggests that LV remodeling, which occurs after MI, may continue for several months. 11,12 In addition to an optimal valve repair technique without residual MR, 3-vessel coronary disease, poor LV function, and prosthetic valve replacement are important determinants of long-term survival rates.
Post-repair MR, preoperative NYHA functional class, and right ventricular function influence the recurrence of CHF and poor functional outcome. 11,12 The early ventricular remodeling that occurs subsequent to a transmural MI results in expansion of the noncontractile infarct zone. The non-infarcted region also undergoes important lengthening. Late remodeling involves the left ventricle globally, and failure to normalize increased wall stress results in progressive dilatation and deterioration in contractile function. Although an increase in cavity size tends to restore stroke volume despite persistently depressed ejection fraction, ventricular dilation has been associated with reduced survival. 13 The volume burden imposed by residual MR further aggravates ventricular remodeling and the progress to CHF. 14,15 Long-term therapy with an angiotensin-converting enzyme inhibitor can favorably alter loading on the left ventricle and reduce progressive ventricular enlargement, as demonstrated in both experimental and clinical studies that were associated with improved survival. 13 Mitral regurgitation detected in the postoperative period is best managed by optimizing the preload and afterload with beta blockers, angiotensin-converting enzyme inhibitors, and inotropics, when a faulty valve repair technique is ruled out. 10,16 Insertion of a prosthetic valve is mandatory if the mitral valve repair technique is inadequate.
The poor long-term results observed with residual MR dictate valve repair when the regurgitant jet is moderate in patients undergoing CABG. Several important studies have demonstrated that MR persisting long term in patients with significant coronary artery disease results in poor survival. 16,17 Despite a lack of consensus on the choice of optimal corrective technique for ischemic MR, mitral valve repair in low-risk patients is associated with lower operative mortality and better survival than prosthetic valve replacement. However, this advantage in survival is not seen in high-risk patients. 1,18
The extent of left and right ventricular dysfunction, severity of coronary disease, and optimal corrective technique in ischemic MR are paramount. Recurrent MR late after ring annuloplasty for ischemic MR is associated with continued LV remodeling, emphasizing its dynamic relationship to the left ventricle. 19 Restrictive annuloplasty with stringent downsizing of the mitral annulus is associated with reverse LV remodeling; at 2-year follow-up, LV end-systolic, end-diastolic, and left atrial dimensions had decreased with minimal or no residual MR. 20 Due to the increased rate of failure of complex valve repairs in ischemic MR, either prosthetic valve replacement or downsizing of the mitral annulus are recommended at the initial operation to improve outcomes.