
Abstract
We report the case of an eight-month-old boy with tracheomalacia secondary to impingement by the right pulmonary artery, together with congenital agenesis of the left lung and the left kidney. Aortopexy and right pulmonary artery-pexy were successful in improving lung function by more than 100%, and the patient remained free of complications in the long term.
Introduction
Tracheomalacia secondary to vascular compression is uncommonly seen as an adjunct to agenesis of the left lung. Moreover, there is no universally accepted operative procedure for dealing with the tracheo-bronchial compression. 1 Here we report the incidence and management of one such case.
Case Report
An eight-month-old boy, a known case of unilateral pulmonary and renal agenesis, presented to the clinic with complaints of a long-standing stridor and recurrent chest infections. Bronchoscopy showed a narrow lower trachea, which was being compressed by a pulsating mass from above. A diagnosis of ‘tracheomalacia secondary to vascular impingement’ was made and the child was admitted for surgical intervention.
With the concurrent presence of a bronchoscope in the trachea, a median sternotomy was performed and the pericardium was opened. The aorta and the right pulmonary artery (RPA) were completely mobilized and the aorta was lifted off the trachea and stitched to the left chest wall. The anterior wall of the collapsible trachea was lifted and fixed to the posterior portion of the aorta (Figure 1). A pedicle flap of pericardium from the left side was then passed below the aorta and RPA and attached to the anterior wall of the aorta for the purpose of lifting the vascular structures off the trachea (Figure 2). With these maneuvers, the tidal volume improved from 25 mL to 65 mL (an increment of 160%) and on bronchoscopy, the tracheal lumen was seen to have considerably widened. The child had a stable hospital course and was discharged six days later.
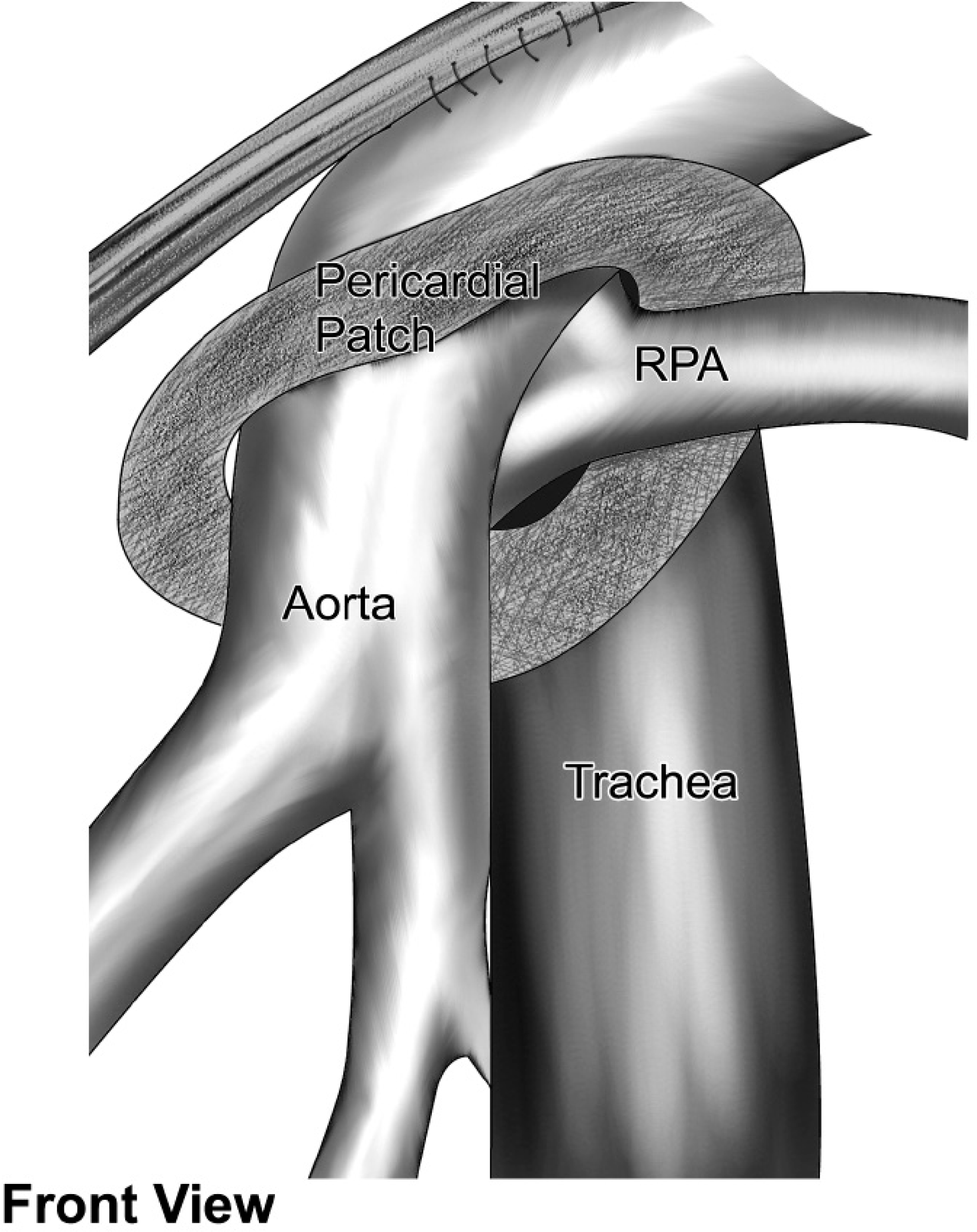
Anterior wall of the trachea was lifted and fixed to the aorta. A pedicle flap of pericardium from the left side was passed below the aorta and RPA and attached to the aorta's anterior wall. RPA = right pulmonary artery.
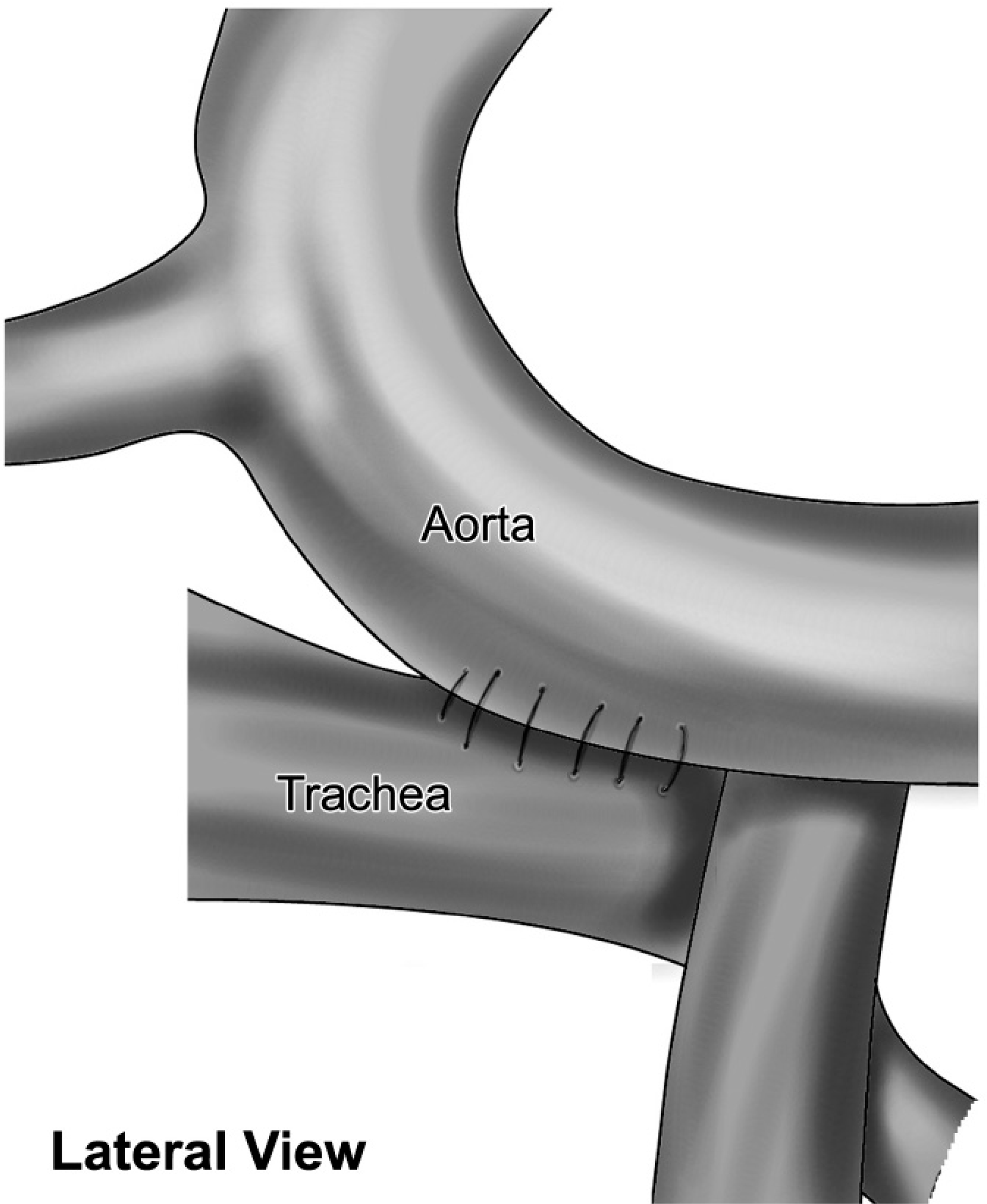
Lateral view showing the trachea fixed to the aorta.
Discussion
Tracheobronchial compression can potentially lead to hypoxic brain injury and can even become life threatening. 2 According to Rimell et al, vascular impingement is the leading cause of tracheobronchial compression. 3 Prompt surgical intervention has a known role in these cases. While it is understood that ensuring patency of the airways under all circumstances is vital, there is a lack of consensus over the various procedures employed by surgeons to treat cases of vascular compression. 1
The various surgical procedures thus far practiced include tracheostomy, 4 open tracheopexy, 5 open aortopexy, 6 thoracoscopic aortopexy, 7 combined tracheopexy, aortopexy 8 and intraluminal tracheal splints. 8 All of these have been seen to yield favorable outcomes. In our case, we opened up the mediastinum and performed pexies of the aorta and RPA using a pedicle flap of pericardium from the left side. The operation was markedly successful in improving lung function, which endured in the long run.
Aortopexy is a simple procedure for the treatment of distal tracheomalacia that is immediately effective and provides long-term relief from obstructive episodes. Fiore and colleagues have reached similar conclusions. 1 The ease and safety of using the pedicle flap of pericardium for vasculo-pexy, demonstrated aptly by our experience, has also been described by Koyluoglu et al. 2 Finally, the improved postoperative outcomes associated with intraoperative bronchoscopy have already been narrated by Abdel-Rahman et al. 6
In view of our experience, as well as review of the literature, we propose our technique of aorto plus RPA-pexy in the management of tracheomalacia. Its advantages include simplicity of procedure, instantaneous and permanent relief, in addition to minimal postoperative complications. We also recommend the use of a pericardial pedicle flap for the vasculo-pexy and support the idea of performing intraoperative bronchoscopy.