
Abstract
Di(2-ethylhexyl) phthalate is an excellent plasticizer for polyvinyl chloride but a known endocrine disrupting chemical. To investigate whether tubing containing no diethylhexyl phthalate reduces the overall extraction of this plasticizer during cardiopulmonary bypass, 16 patients undergoing coronary artery bypass grafting were randomly divided into 2 groups of 8 each. Group A had tubing containing diethylhexyl phthalate in the circuit, and group B had no diethylhexyl phthalate in the tubing. The plasma diethylhexyl phthalate level at the end of cardiopulmonary bypass was significantly increased compared to before anesthesia in both groups (group A: 103 ± 60 to 2,094 ± 1,046 ng·mL−1; group B: 135 ± 60 to 472 ± 141 ng·mL−1), and it was significantly higher in group A than group B. This study demonstrates that using tubing free from diethylhexyl phthalate significantly reduces the release of this agent during cardiopulmonary bypass, which may minimize exposure to diethylhexyl phthalate.
Introduction
Di(2-ethylhexyl) phthalate (DEHP) is widely used in polyvinyl chloride (PVC) disposable medical devices. It is an excellent plasticizer as it makes PVC tubing soft and flexible, but it has been reported to be an environmental endocrine disrupter. Patients undergoing medical interventions such as intravenous therapy, blood transfusion, extracorporeal membrane oxygenation, and cardiopulmonary bypass (CPB) can be exposed to DEHP released from PVC. The reproductive-related toxicity of DEHP and its metabolite mono(2-ethylhexyl) phthalate have been a focus of study in recent years, and are believed to have a great effect on humans. 1 Alternative non-DEHP CPB tubing has been developed to reduce such adverse effects. This study compared DEHP extraction into the blood from these 2 types of CPB tubing.
Patients and Methods
The medical ethics committee of our institution approved the protocol for this study. Informed consent was obtained from all patients. Sixteen men undergoing elective coronary artery bypass grafting under CPB were randomly divided into 2 groups of 8 each. Group A had DEHP-PVC tubing in the circuit; group B had non-DEHP-PVC tubing. The circuits in group A consisted of arterial and venous CPB tubing (Mera Exceline H; Senko Inc., Tokyo, Japan), an oxygenator, a hard-shell venous reservoir, cardiotomy reservoir, an arterial filter and a centrifugal pump; these all contained DEHP. The circuits in group B consisted of non-DEHP arterial and venous CPB tubing (Mera Exceline R) in which tri(2-ethylhexyl) trimellitate was used as a plasticizer, and all other components were the same as those used in group A.
Anesthesia was induced after premedication with midazolam, and maintained with fentanyl, midazolam and vecuronium bromide. The circuits were primed with a mixture of 1,300 mL of lactated Ringer's solution, 250 mL of human serum albumin 250 mg·mL−1, 200 mL of mannitol 200 mg·mL−1 and 100 mL of sodium bicarbonate 84 mg·mL−1. Standard ascending aortic cannulation and right atrial cannulation were performed. Before aortic cannulation, all patients received 300 IU·kg−1 bovine heparin. Activated clotting time was measured using a Hemochron 801 (International Technidyne, Edison, NJ, USA). The activated clotting time was maintained at ≥ 400 sec by administration of heparin as required during CPB. While the patient was fully heparinized, a cardiotomy suction device was used to return pericardial blood. At all other times during the operation, a cell saver (Hemonetics Cell-Saving Device 5 model 2005; Hemonetics, Braintree, MA, USA) was used. Blood samples were obtained before induction of anesthesia and just after the end of CPB (pump off). Plasma was separated from blood cells by centrifugation at 3,000 × g for 10 min, and stored at −80°C until analysis. Quantitative analysis of DEHP was performed by selected ion monitoring gas chromatography, as reported earlier. 2
All data were analyzed using Stat-View 5.0 and Super ANOVA 1.11 (Abacus Concepts, Berkeley, CA, USA). All results are reported as mean ± standard deviation. A p value of less than 0.05 was considered statistically significant.
Results
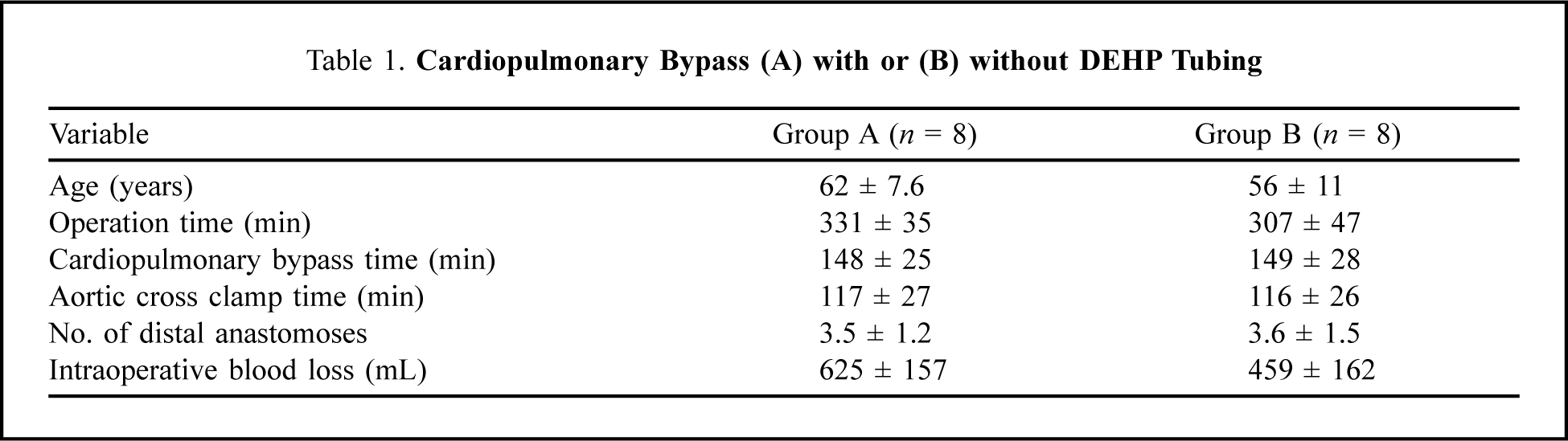
Perioperative patient data are summarized in Table 1. No significant differences between the two groups were observed. There was no incidence of perioperative myocardial infarction, cerebral infarction, thromboembolism or other complication in any patient. The level of DEHP was significantly increased at the end of CPB compared to the preoperative level in both groups (group A: from 103 ± 60 to 2,094 ± 1,046 ng·mL−1, p < 0.001; and group B: from 135 ± 60 to 472 ± 141 ng·mL−1, p < 0.01). At the end of CPB, the level of DEHP in group A was significantly higher than that of group B (Figure 1).
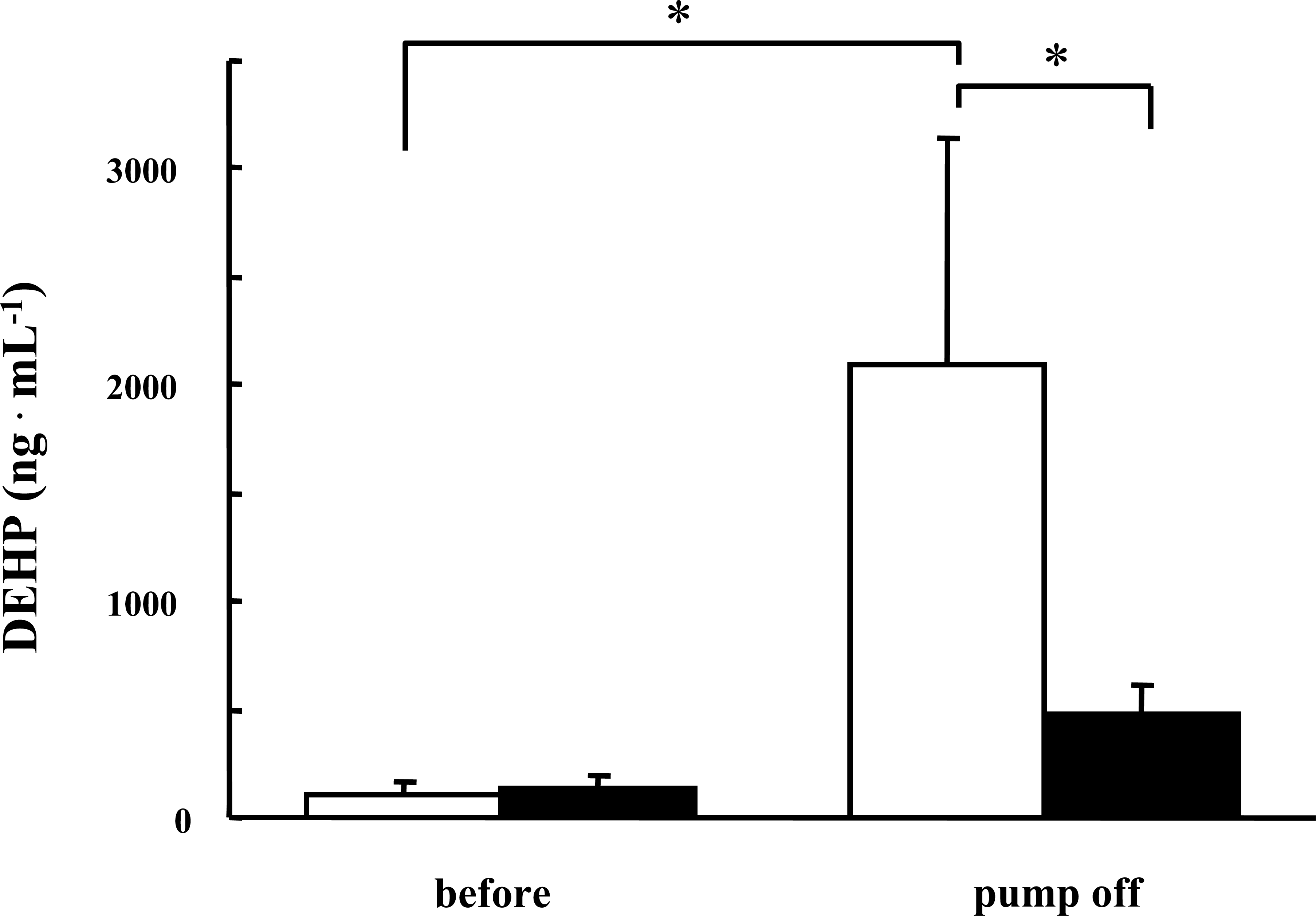
Changes in di(2-ethylhexyl) phthalate (DEHP) levels pre-anesthesia (before) and at the end of cardiopulmonary bypass (pump off) in 2 groups of 8 each. Open bars = group A, with DEHP tubing; closed bars = group B, without DEHP tubing. *p < 0.05.
Cardiopulmonary Bypass (A) with or (B) without DEHP Tubing
Discussion
This study demonstrates that using non-DEHP tubing significantly reduces the release of DEHP during CPB. However, the blood level of DEHP increased after CPB even in group B, because the other circuit components were not made of DEHP-free materials. The effects of acute and chronic exposure to DEHP and its metabolite mono(2-ethylhexyl) phthalate have been studied. High mono(2-ethylhexyl) phthalate levels acutely induced vimentin localization in Sertoli cells, increased caspase 3 activity in the testis, and affected the respiratory tract in mice. 3,4 Chronically high DEHP levels resulted in various biological effects including testicular atrophy in rats, proliferation of peroxisomes in rodents, and liver tumors in rats and mice. 5 –8 Therefore, the Scientific Committee on Toxicity, Ecotoxicity and the Environment of the European Commission established a tolerable daily intake of DEHP. However, there are no safety criteria concerning DEHP exposure during medical interventions.
Although the reproductive toxicities of DEHP are of great concern, there have been few studies on the release of DEHP during medical interventions in humans in vivo. Karla and colleagues 9 reported a plasma concentration of DEHP of 3,500 ng·mL−1 after 1 hour of extracorporeal membrane oxygenation. Kambia and colleagues 10 found plasma DEHP levels of approximately 600 ng·mL−1 after 3 hours of hemodialysis. Several groups have looked at the influence of heparin coating on DEHP release, but the effect of such coating remains controversial. Hildenbrand and colleagues 2 found that the level of DEHP was 42,600 ng·mL−1 in PVC tubes and approximately 15,000 ng·mL−1 in heparin-coated PVC tubes after 90 min of Chandler loop circulation in vitro. Thus heparin-coated PVC tubes reduced the extraction of DEHP, but did not completely prevent leaching. Karla and colleagues 9 reported that heparin-coated PVC tubes significantly reduced the extraction of DEHP after extracorporeal membrane oxygenation in vitro. In contrast, Sakurai and colleagues 11 noted that heparin-coated tubes did not reduce the extraction of DEHP after 30 min circulation in vitro.
Gourlay and colleagues 12 reported that DEHP-plasticized PVC and DEHP itself are pro-inflammatory in blood, and methanol washing of the PVC surface to reduce DEHP attenuated the inflammatory response. So far as we are aware, this is the first study on changes in DEHP levels using non-DEHP tubing during on-pump cardiac surgery. Our results show that DEHP levels increase markedly during CPB using conventional circuits, but DEHP release was significantly reduced when non-DEHP CPB tubing was used for parts of the circuit. Although it is unclear how much damage would result from these levels of DEHP, less risk of potential ill effects would be the likely result if all CPB circuits were made from DEHP-free materials.
There are some limitations to this prospective study. First, we could not demonstrate any evidence of DEHP toxicity during or after CPB. Second, we did not determine how long the elevated concentration of DEHP would remain after CPB. Thus, further study is needed. Considering that there have been no criteria set for safe levels of DEHP exposure in human during medical interventions, it is important that the risk of DEHP exposure be reduced as much as possible. We consider using non-DEHP tubes to be clinically preferable.