
Abstract
A 41-year-old woman underwent successful excision of a leiomyosarcoma of the left atrium. The preferential left atrial location and frequent myxoid appearance of leiomyosarcoma of the heart make it particularly difficult to distinguish preoperatively from atrial myxoma. Early diagnosis and aggressive surgical intervention with chemotherapy may improve the prognosis.
Introduction
Leiomyosarcoma is a rare form of malignant cardiac tumor that occurs predominantly in the left atrium. Early detection and immediate initiation of an aggressive therapeutic strategy are crucial for improving the survival of patients. We report the case of a 41-year-old woman previously treated for knee leiomyosarcoma.
Case Report
A 41-year-old woman was admitted to our hospital with suspected leiomyosarcoma on the left atrial posterior wall, detected by positron-emission tomography (PET; Figure 1). She was on follow-up at an outpatient cancer unit. When diagnosed to have right breast adenocarcinoma 11 years earlier, she had undergone ablation and exenteration of the right axilla. She received 4 cycles of chemotherapy with fiuorouracil (500 mg·m2), doxorubicin (50 mg·m2), and cyclophosphamide (500 mg·m2). This regimen was repeated on a monthly basis. The following year, she was diagnosed with a left knee sarcoma. Histological examination confirmed the diagnosis of leiomyosarcoma. Chemotherapy was initiated with cyclophosphamide 1,000 mg, doxorubicin 100 mg, vincristine 2 mg and dacarbazine 2,400 mg. Five years later, her left leg was amputated because of local recurrence of the knee tumor. In the same year, her left axillary node was extirpated due to metastasis of leiomyosarcoma. Two years later, she had a hysterectomy for leiomyosarcoma. After another 2 years, she underwent excision of 2 subcutaneous metastases of the leiomyosarcoma. The following year, she had a right lung metastasis of the leiomyosarcoma (subpleural location) excised. Subsequently, the suspicion of cardiac neoplasm suggested by PET was confirmed by transesophageal echocardiography (Figure 2) and magnetic resonance imaging, demonstrating an oval expansion on the left atrial inferior wall, measuring 30 × 32 × 33 mm, and involving the whole left atrial wall. There were no signs of valve obstruction; only minor mitral regurgitation was seen. Surgical removal of the tumor was performed using a median sternotomy approach. Cardiopulmonary bypass was instituted with bicaval cannulation and standard aortic cannulation. Upon opening the pericardium, the tumor was seen extending from the left atrium to the left ventricle, and also involving the coronary sinus. The tumor was completely excised, and the coronary sinus was reconstructed using a pericardial patch fixed with glutaraldehyde. The left atrial and ventricular defect, measuring 6 × 5 cm in diameter, was filled with fibrin glue. The left atrial opening was subsequently closed and reconstructed with an autologous pericardial patch. The patient was easily weaned from the pump and returned to the recovery room in good condition. The postoperative course was uneventful and she was discharged on postoperative day 9. Histological examination of the surgical specimen showed a myxoid variant of leiomyosarcoma arising from the left atrium. The finding was identical with that of the tumor in the left leg. Afterwards, the patient received 7 cycles of chemotherapy with ifosfamide at a total dose of 8,350 mg in a 24-hour infusion. This regimen was repeated monthly and stopped after 6 months when follow-up PET indicated no local recurrence or systemic metastasis. Transthoracic echocardiography at 10 months postoperatively showed normal ventricular function with no abnormal masses in the heart chambers.
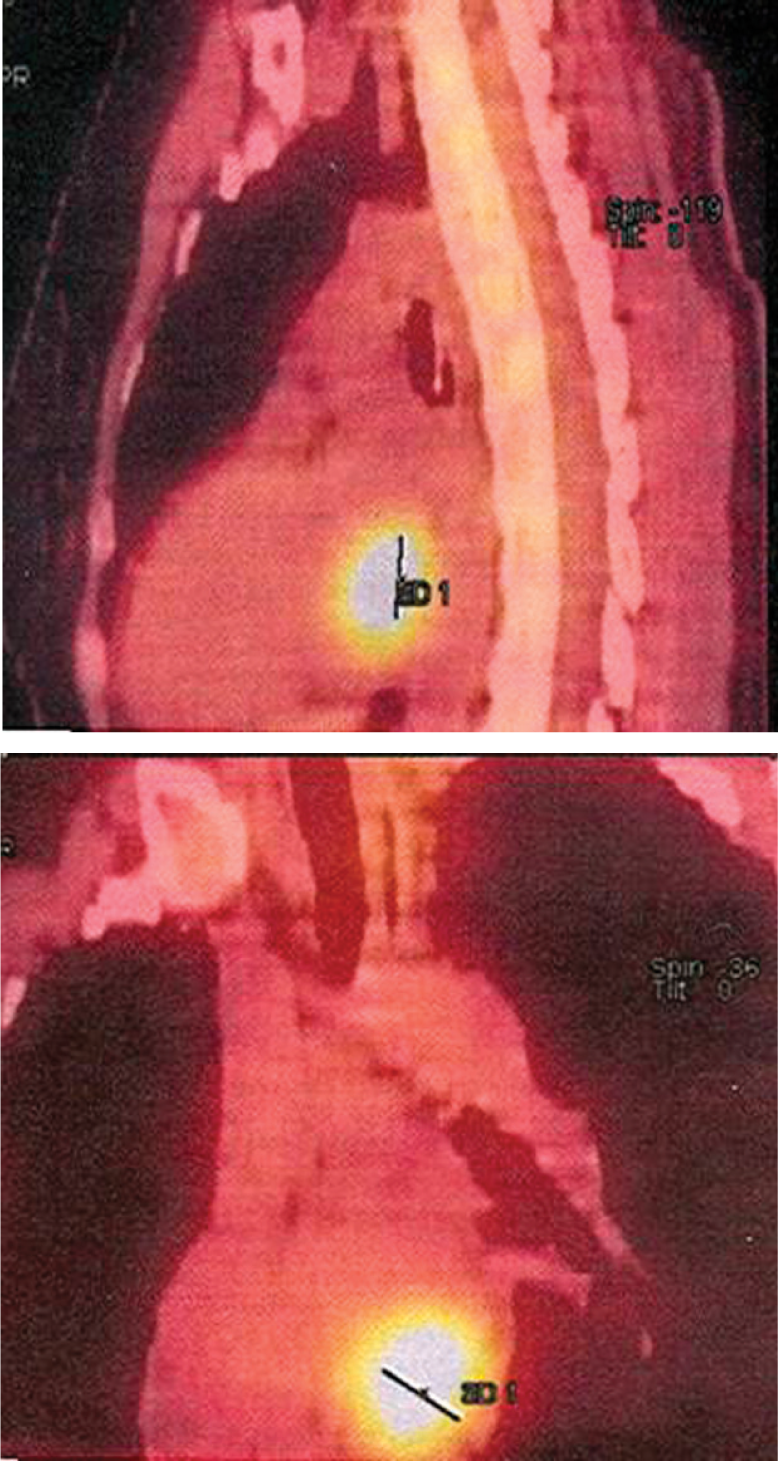
Positron-emission tomography showing the tumor mass in the left atrium.
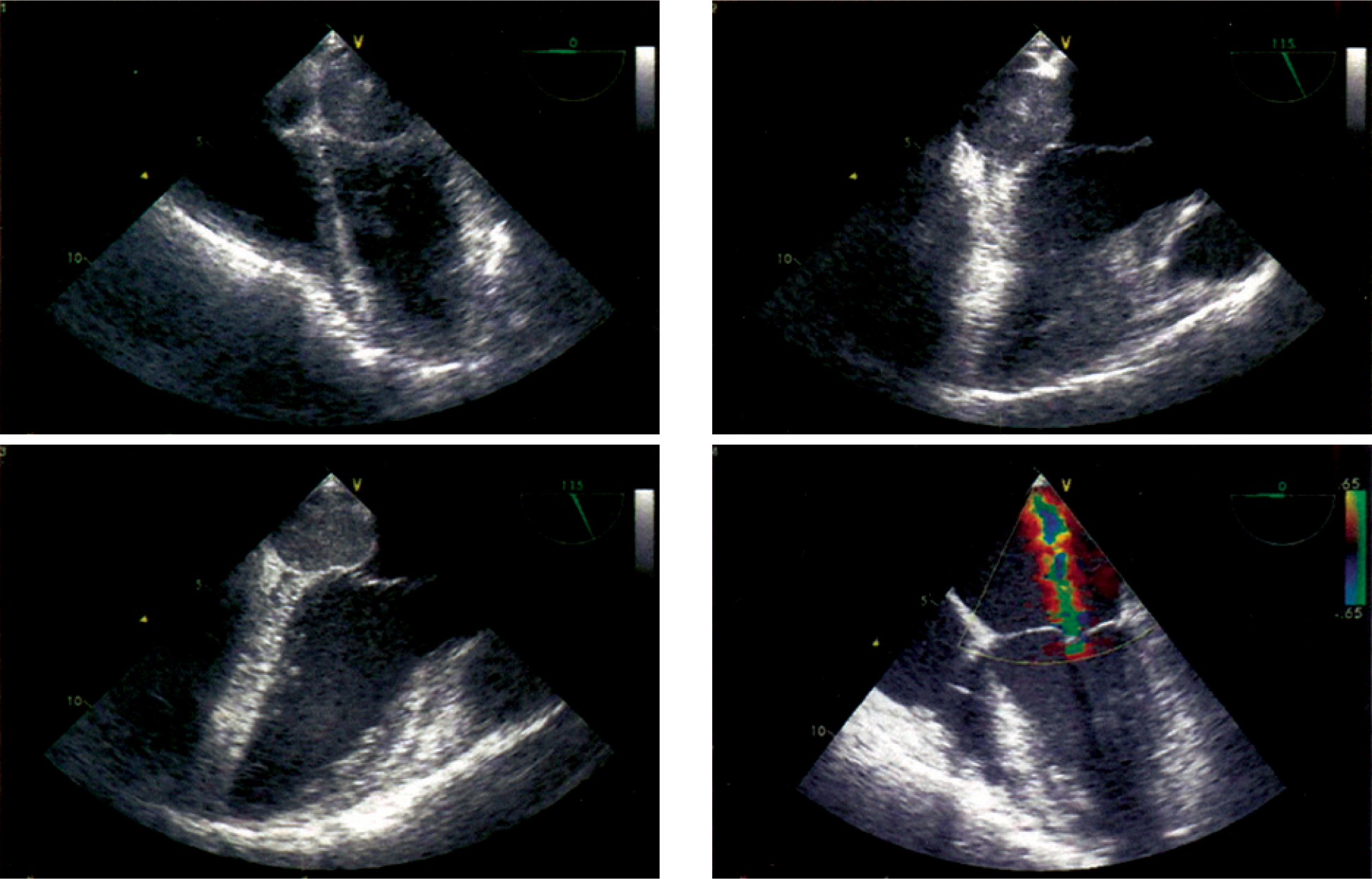
Transesophageal echocardiography in apical 4-chamber view showing the tumor in the left atrium.
Discussion
Like atrial myxomas, leiomyosarcoma occurs predominantly in the left atrium. 1,2 The preferential left atrial location and frequent myxoid appearance of primary leiomyosarcoma of the heart make it particularly difficult to distinguish them preoperatively from atrial myxoma. 1 Because the tumor mass is frequently misdiagnosed as a myxoma during echocardiography, there are often delays in surgical intervention. 2 In our patient, the diagnosis was established using PET screening during follow-up of her previous cancer.
Surgical resection is the treatment of choice for all patients with cardiac neoplasms. 3 It is curative for benign tumors, and may significantly prolong life in patients with malignant lesions. 4,5 Postoperative radiation therapy and chemotherapy may improve survival in patients with malignant intracardiac tumors. 6 This patient was alive and free from symptoms at 15 months after the operation. This case illustrates that early initial diagnosis and aggressive surgical intervention combined with chemotherapy may be life saving and necessary to improve the long-term prognosis.