
Abstract
Extralobar pulmonary sequestration usually occurs between the left lower lobe and the diaphragm; occurrence in the hilum has not been reported previously. An unusual case of extralobar pulmonary sequestration, presenting initially as a hilar bronchogenic cyst in a 43-year-old female, is described.
Introduction
Extralobar pulmonary sequestration is an unusual condition in which separate lung parenchyma forms, supplied by systemic arteries, but lacking normal airway communication. The most common site of occurrence is between the left lower lobe and the diaphragm. 1 Although this anomaly has occasionally been found in the mediastinum, pericardium, or even the abdomen, occurrence in the hilum has not been reported previously. 1 –3
Case Report
A 43-year-old woman with normal development was referred for investigation of dry cough and chest distress over the previous month. Her medical history and physical examination were unremarkable. Fiberoptic bronchoscopy was normal. Posteroanterior and lateral chest radiography showed a well-defined soft-tissue hilar mass. Computed tomography revealed a lobulated cyst at the superior-anterior hilum, sharply delineated and measuring 3.7 cm in diameter. The mass abutted closely to the left pulmonary artery and its main branches, without local compression. No contrast enhancement was observed (Figure 1). A diagnosis of bronchogenic cyst was initially considered. A left thoracotomy was performed for cyst resection. As demonstrated by computed tomography, the cyst had a very thin wall that was easily broken and released its abundant gray mucoid content. After removal of this fluid, the cyst was easily dissected from the adjacent pulmonary tissue and hilar vessels. The most surprising finding was well-nourished bud-like tissue connected to the cyst (Figure 2). This abnormal structure measured 3.5 cm in length, with a thin pliable fibrovascular pedicle and pink prism-shaped body. The macroscopic appearance shared great similarity with adjacent collapsed lung tissue, which led to a diagnosis of solitary undeveloped lung.
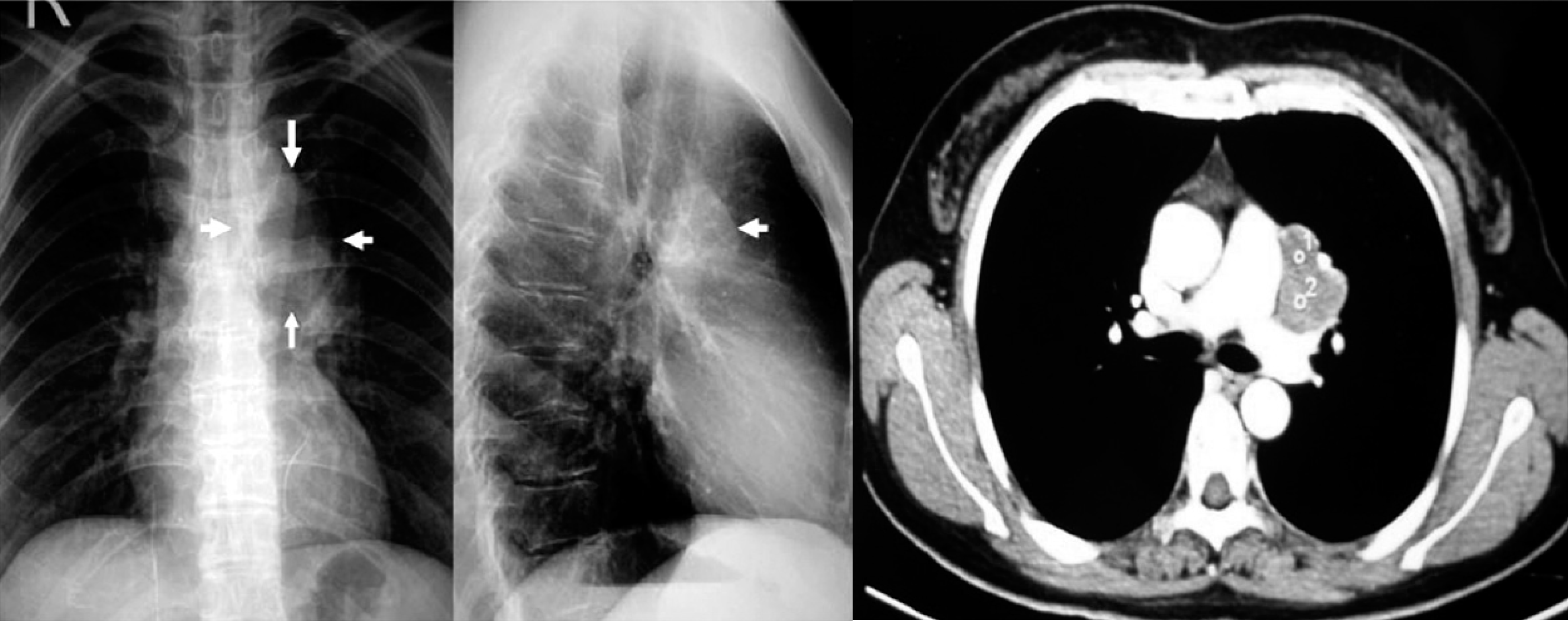
Posteroanterior and lateral radiographs showing a lobulated mass in the hilum; computed tomography suggested a bronchogenic cyst close to the left pulmonary trunk.
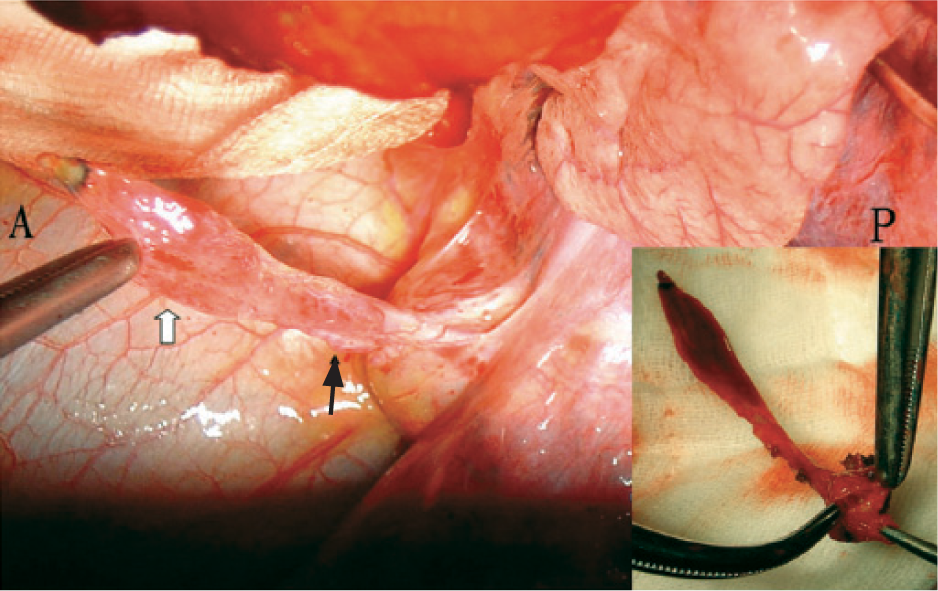
The hilar cyst and connected prism-shaped pulmonary tissue; black arrow points to the fibrovascular pedicle, white arrow indicates the sequestrated lung tissue; occluded bronchi are shown in the inset. A = anterior, P = posterior.
Restoration of left ventilation showed no communication between this accessory lung and normal bronchi. A cut section confirmed that the pedicle was obliterated bronchi (Figure 2). The aberrant systemic arterial supply was a small branch from the phrenic artery, which passed in front of the cyst and the mass. Postoperative recovery was uneventful, and the patient was discharged after 7 days. Histology confirmed extralobar pulmonary sequestration. Microscopy showed a mature bronchogenic cyst and occluded cartilaginous bronchi lined by typical ciliated pseudo-stratified columnar epithelium, solid lung parenchyma filled with a large amount of amorphous mucin, and 2 supplying arterial branches derived from the main aberrant artery (Figure 3).
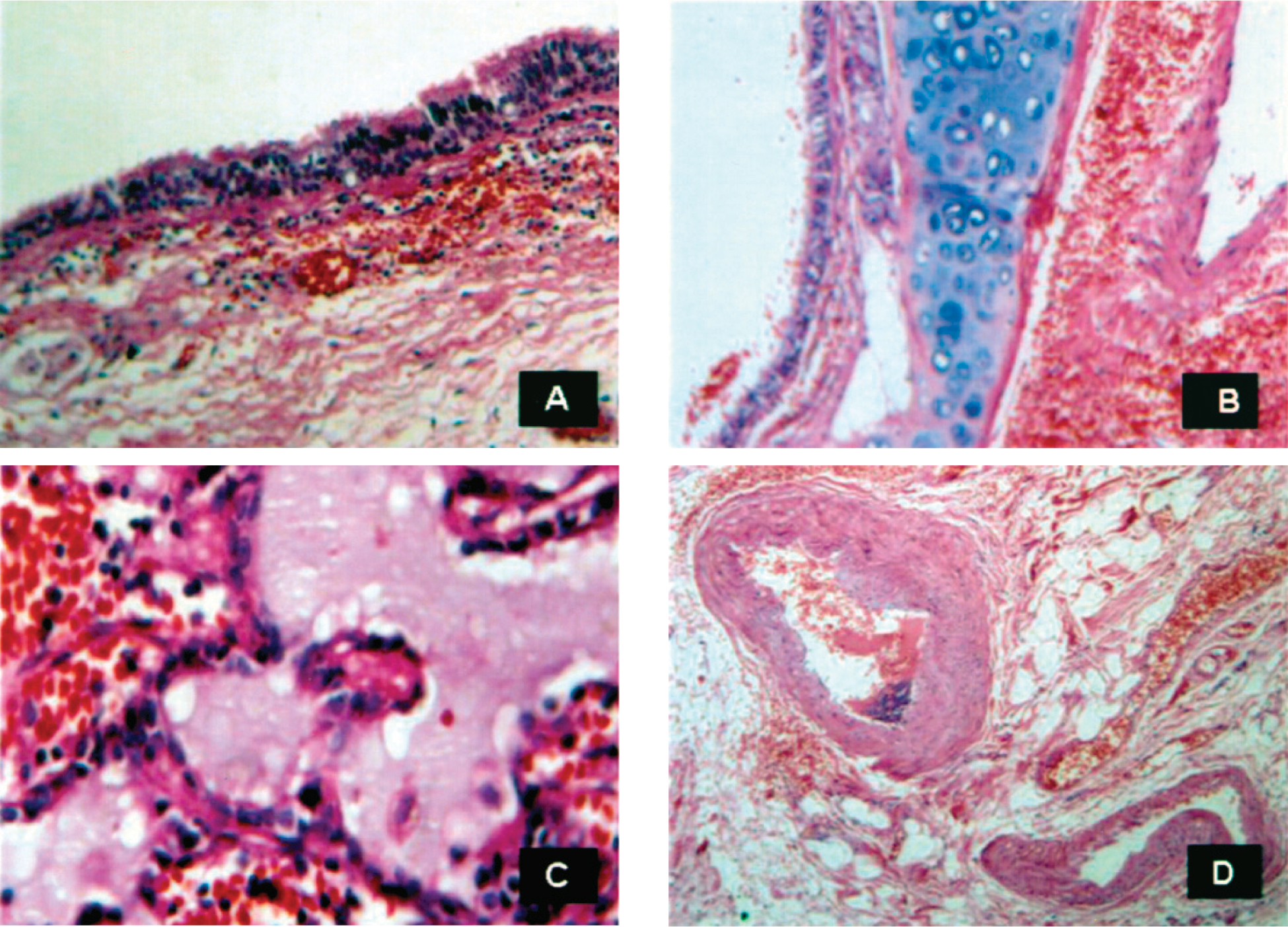
Histology showed (A & B) mature bronchogenic cyst and cartilaginous bronchi lined by typical ciliated pseudo-stratified columnar epithelium, (C) solid lung parenchyma filled with amorphous mucin, and (D) the supplying arteries.
Discussion
The anatomic characteristics of extralobar pulmonary sequestration are aberrant systemic blood supply and an integrated pleural envelope separating the sequestrated portion from normal lung. The majority occur in the left lower chest cavity; it is seldom seen as a mediastinal or pericardial abnormality. 1 This case had several distinct features. First, extralobar pulmonary sequestration is rarely found in the hilum. At the hilum or adjacent mediastinal region, it mimics cystic changes in most cases. Porte and colleagues 4 described a case of bronchogenic cyst of the esophageal wall, which was associated with dextroisomerism and agenesia of the left pericardium. Their systematic review mentioned 3 other reports of bronchogenic cyst. Second, it is rare for extralobar pulmonary sequestration to occur in an adult. There is a higher incidence in children, and the defect is usually noticed during assessment for associated congenital anomalies. 3,5 Such coexisting anomalies may be seen in 50%–60% of patients, and include diaphragmatic hernia, cardiovascular malformation, bronchogenic cyst and pulmonary anomalies; whereas in adults, extralobar pulmonary sequestration is often asymptomatic and discovered incidentally. 2 Furthermore, it is rare for the phrenic vessel to provide the aberrant blood supply. Blood supply most often arises from the thoracic aorta. 6 Minor origins are the intercostals and subclavian arteries. Selective angiography or magnetic resonance angiography is usually emphasized for accurate preoperative diagnosis. However, such decision-making was difficult in this case because radiographs did not suggest the existence of small aberrant vessels.