
Abstract
Cardiac troponin levels are frequently elevated in patients with chronic renal failure, hence diagnosis of myocardial necrosis is difficult. The prevalence of elevated serum troponin T was determined and its diagnostic value in acute coronary syndrome was assessed in patients with chronic renal insufficiency. A retrospective cross-sectional analysis was performed in 227 patients with chronic renal insufficiency and a diagnosis of unstable angina, non-ST or ST-segment elevation myocardial infarction. All patients had baseline serum troponin T levels measured at previous visits; the baseline troponin T level was raised in 53.3%. Cardiac troponin T levels did not correlate with creatinine levels, and were not affected by dialysis. Mortality after an acute coronary event was high (46.3%). Because of the elevated baseline cardiac troponin T levels, detection of acute coronary syndrome in patients with chronic renal failure requires evaluation of serial cardiac enzyme measurements and serial 12-lead electrocardiograms. Early and definitive cardiac interventions may contribute towards decreasing the mortality rate in this group of patients.
Introduction
The troponins (Tn) are regulatory proteins found in both skeletal and cardiac muscle. Three subunits have been identified: TnI, TnT, and TnC. The genes encoding both skeletal and cardiac isoform are identical for TnC, in contrast to TnI and TnT which have distinct cardiac and skeletal forms. This accounts for the unique cardiac specificity of cardiac troponin (cTn), and the development of immunoassays to differentiate the troponins. Patients with underlying chronic renal failure, especially those on hemodialysis, are often at increased risk of coronary artery disease. Studies have shown a high prevalence of elevated serum cTn in patients with chronic renal failure, even in the absence of acute coronary syndrome. Small group analysis has shown elevated cTnT (≥0.1 ng·mL−1) in 17%–23.8% of patients on chronic dialysis. The diagnosis of myocardial necrosis in patients with renal failure is often difficult because the biochemical markers of cardiac damage, such as creatine kinase-MB and cTn, may be spuriously elevated. Many large-scale trials demonstrating the value of serum troponin levels in predicting adverse events and in guiding therapy and intervention in acute coronary syndrome have excluded patients with renal failure. No evaluation of baseline serum TnT has been performed locally in these patients. The primary aims of this study were to determine the prevalence of elevated serum cTnT and assess its diagnostic value in acute coronary syndrome in patients with chronic renal insufficiency. The secondary objectives were to evaluate the characteristics of the study population, investigate a correlation between serum cTnT and creatinine levels, and carry out subgroup analysis of cTnT levels in patients with chronic renal failure or endstage renal failure requiring dialysis
Patients and Methods
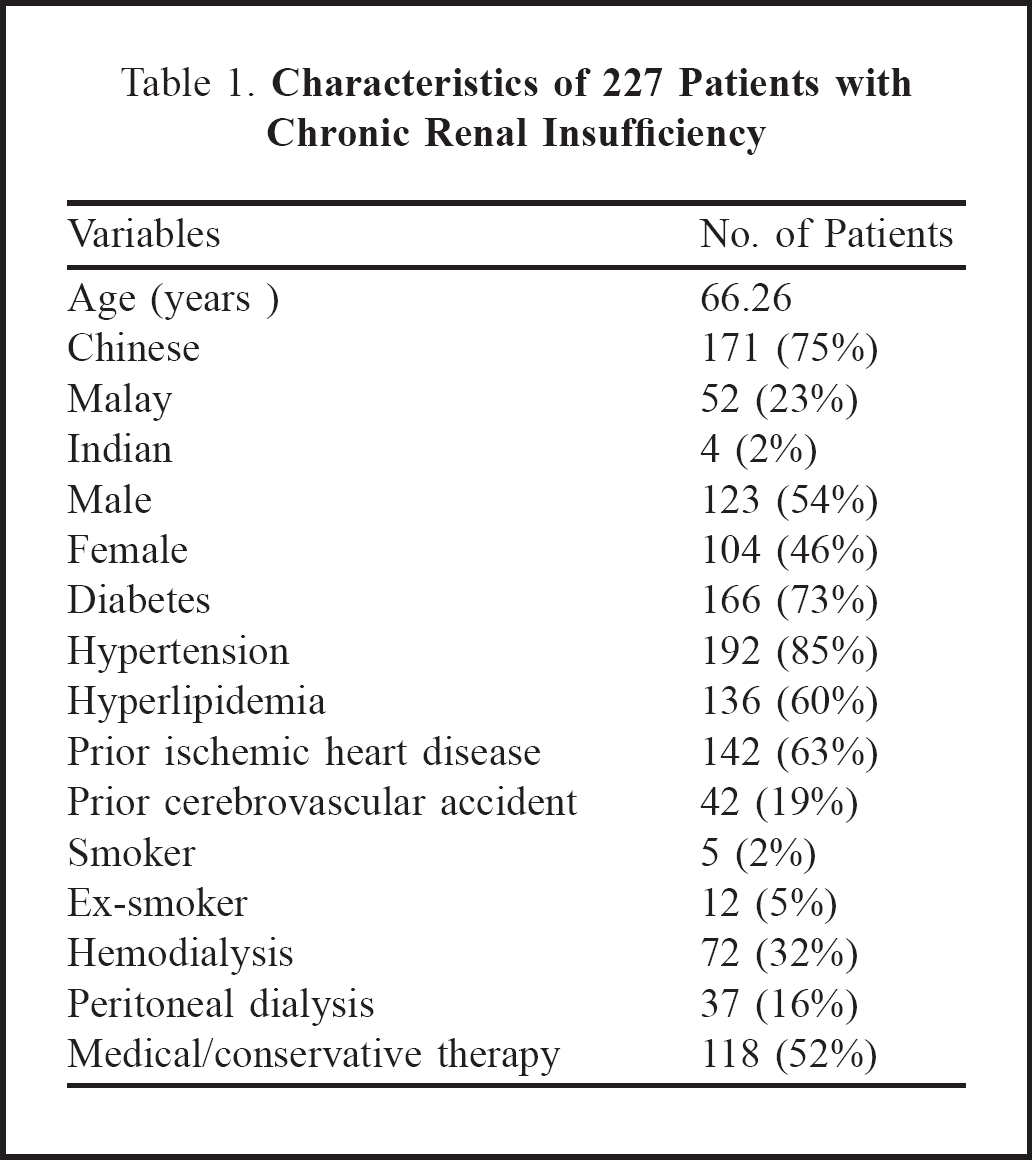
A retrospective cross-sectional analysis was performed on data of patients admitted to Singapore General Hospital from May 2002 to August 2005 with chronic renal insufficiency and unstable angina pectoris, non-ST-segment-elevation myocardial infarction (MI), or ST-segment-elevation MI. Patients were recruited on the basis of their hospital discharge summary diagnosis, including the combination of either chronic renal failure (ICD-9 585), endstage renal failure (ICD-9 5851), or renal impairment (ICD-9 5859), and unstable angina (ICD-9) or acute MI (ICD-9 40170/40171/41072/41091/41011/41041/41061). There were 227 patients identified using these search parameters. Their baseline creatinine levels ranged from 200 to 1,000 μg·mL−1, giving calculated creatinine clearance rates of 5 to 23 mL·min−1 (assuming a weight of 60 kg per person). All surveyed patients had baseline serial serum cTnT levels measured to exclude acute coronary syndromes prior to onset of the cardiac event. There were 123 men and 104 women, aged 30 to 94 years. Patient characteristics are listed in Table 1. Data are given as frequency and %, except for age which is reported as the mean. Of these patients, 213 (93.8%) had non-ST-segment-elevation MI, 5 (2.2%) had ST-segment elevation MI, and 9 (4%) had unstable angina. This was independently confirmed by a cardiologist and the primary treating physician, based on the clinical picture, serial electrocardiograms, and cardiac enzymes, as well as cardiac catheterization or noninvasive cardiac imaging.
Characteristics of 227 Patients with Chronic Renal Insufficiency
Results
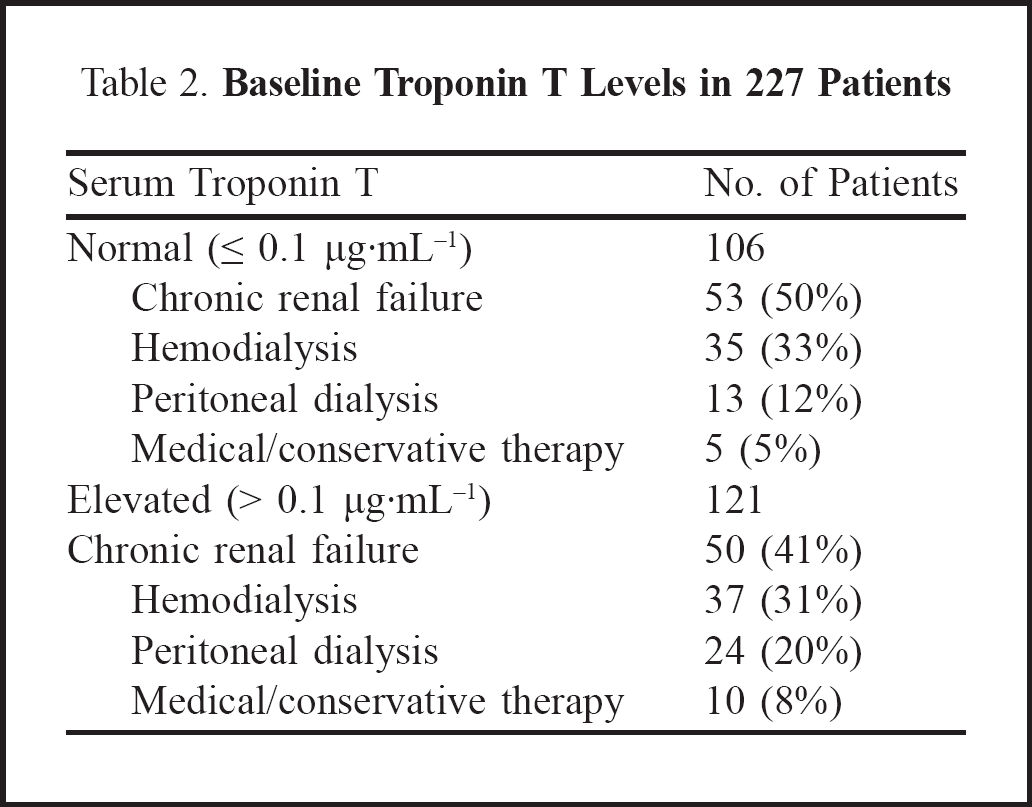
Using a normal level of cTnT ≤ 0.1 μg·mL−1, we found 106 (46.7%) patients in our cohort had normal baseline cTnT levels, and 121 (53.3%) had raised baseline cTnT levels. These patients were further analyzed according to dialysis subgroups (Table 2). This showed no difference in baseline cTnT levels between dialyzed and non-dialyzed patients. However, those on peritoneal dialysis were more likely to have an elevated baseline cTnT. There was no correlation between elevated baseline cTnT and creatinine levels (Pearson's correlation coefficient, −0.062). The overall mortality rate in patients with renal dysfunction who had an acute coronary event was high at 46.3% (105/227 patients). There was no significant difference between mortality rates in patients with acute coronary syndrome and elevated or normal baseline TnT levels (chi-square test, p = 0.614). The treatment of renal failure (hemodialysis, peritoneal dialysis, or medical therapy) did not give rise to any difference in mortality rates (p = 0.616).
Baseline Troponin T Levels in 227 Patients
Discussion
Despite the use of cardiac troponins as the current biochemical diagnostic markers of choice in acute coronary syndromes, they are not early markers of myocardial necrosis. 1,2 The first appearance of cTn in plasma occurs 4–8 hours after the onset of symptoms. This is similar to the release of creatine kinase-MB. 3 Cardiac troponin levels remain elevated for 7–10 days after MI. 4,5 In addition to the diagnostic value of cTn in patients with an acute coronary syndrome, other trials have shown further applications including a correlation with mortality in patients with acute coronary syndrome undergoing thrombolysis. 7 Cardiac troponin levels are also regarded as independent predictors of mortality in patients with acute coronary syndromes, and such data can help in risk stratification to identify those at high risk of adverse cardiac events (death, acute MI) up to 6 months after the initial event. 4,7,9 –12
The increase in serum troponin originates from the myocardium (not a false-positive result), and is not related to the myopathy associated with renal failure. Troponin T is elevated more frequently than TnI, and the levels of both are unaffected by dialysis. 13 Troponin I has a higher specificity, but is not conclusive for MI. 14 Diabetic patients are more likely to have elevated cTnT and cTnI than those without diabetes. 15,16 Elevated baseline cTn levels have been associated with cardiovascular risk factors, history of ischemic heart disease, and left ventricular hypertrophy in asymptomatic patients on chronic hemodialysis. 15 The mechanism underlying such a rise in troponin in diseases of noncardiac origin is unknown, and the clinical significance is still currently being debated, although it has been shown to be an important independent prognostic indicator in patients on hemodialysis for chronic renal failure. 16
Several theories regarding this elevation of cTn have been postulated: the patients might have ischemic heart disease as a co-morbidity, and severe stress caused by an acute noncardiac clinical event may result in minor leakage of myocardial markers; 17 –20 the patients might have sustained subclinical myocardial injury; 16 raised cTn levels might be caused by an inflammatory response to chronic renal failure; 16,19 or they might result from chronic volume-overload. 16 In our study, 53.3% of patients with renal dysfunction had an elevated baseline cTnT level. This did not correspond to the extent of renal failure, nor was it affected by dialysis. An elevated baseline TnT level did not imply increased likelihood of MI, and it did not translate into higher mortality rates in those who suffered MI. However, the mortality rate following an acute coronary event was high in patients with renal dysfunction. This is likely to be due partly to delayed diagnosis, and hence delayed initiation of therapy.
We acknowledge some limitations of this study. A search for all patients with renal dysfunction, instead of targeting only those with a diagnosis of acute coronary syndrome, would have given a clearer picture of the baseline variations in cTnT levels in this population. In addition, calculation of the baseline creatinine clearance rates would have given a better idea of renal function, rather than relying solely on creatinine levels to reflect this. There is no gold standard for the diagnosis of non-ST-segment elevation MI and unstable angina in this group of patients. Instead, we relied on independent agreement between the treating physician and cardiologist, as well as serial cardiac enzymes and electrocardiograms, to establish the diagnosis. Troponin I has been thought to have higher specificity than TnT for diagnosing MI. However, the institution in which these patients were managed did not have provision for TnI analysis.
Our results show that a high proportion of patients with chronic renal dysfunction had elevated baseline cTnT levels. The rise in cTnT did not correlate with creatinine levels, and was not affected by dialysis. Mortality after an acute coronary event is high in such patients. Because of their elevated baseline cTnT levels, determination of possible acute coronary syndrome requires serial cardiac enzyme measurements and serial 12-lead electrocardiograms. Early and definitive cardiac intervention may contribute towards decreasing the mortality rate in this group of patients.