
Abstract
An unusual systemic venous drainage pattern was found in a 30-year-old man with ostium secundum atrial septal defect and pulmonary stenosis. He had the rare association of absent right superior vena cava, persistent left superior vena cava draining into the coronary sinus, and a left-sided inferior vena cava draining into a left superior vena cava through the hemiazygous vein.
Introduction
Absent right superior vena cava (RSVC) with persistent left superior vena cava (LSVC) and visceroatrial situs solitus is very rare. 1 Of all the anomalies involving the inferior vena cava (IVC), a left-sided IVC communicating with a persistent LSVC through the hemiazygous vein is the least common. 2 These unusual venous anomalies involving both venae cavae occurred in a patient with ostium secundum atrial septal defect (ASD) and pulmonary stenosis.
Case Report
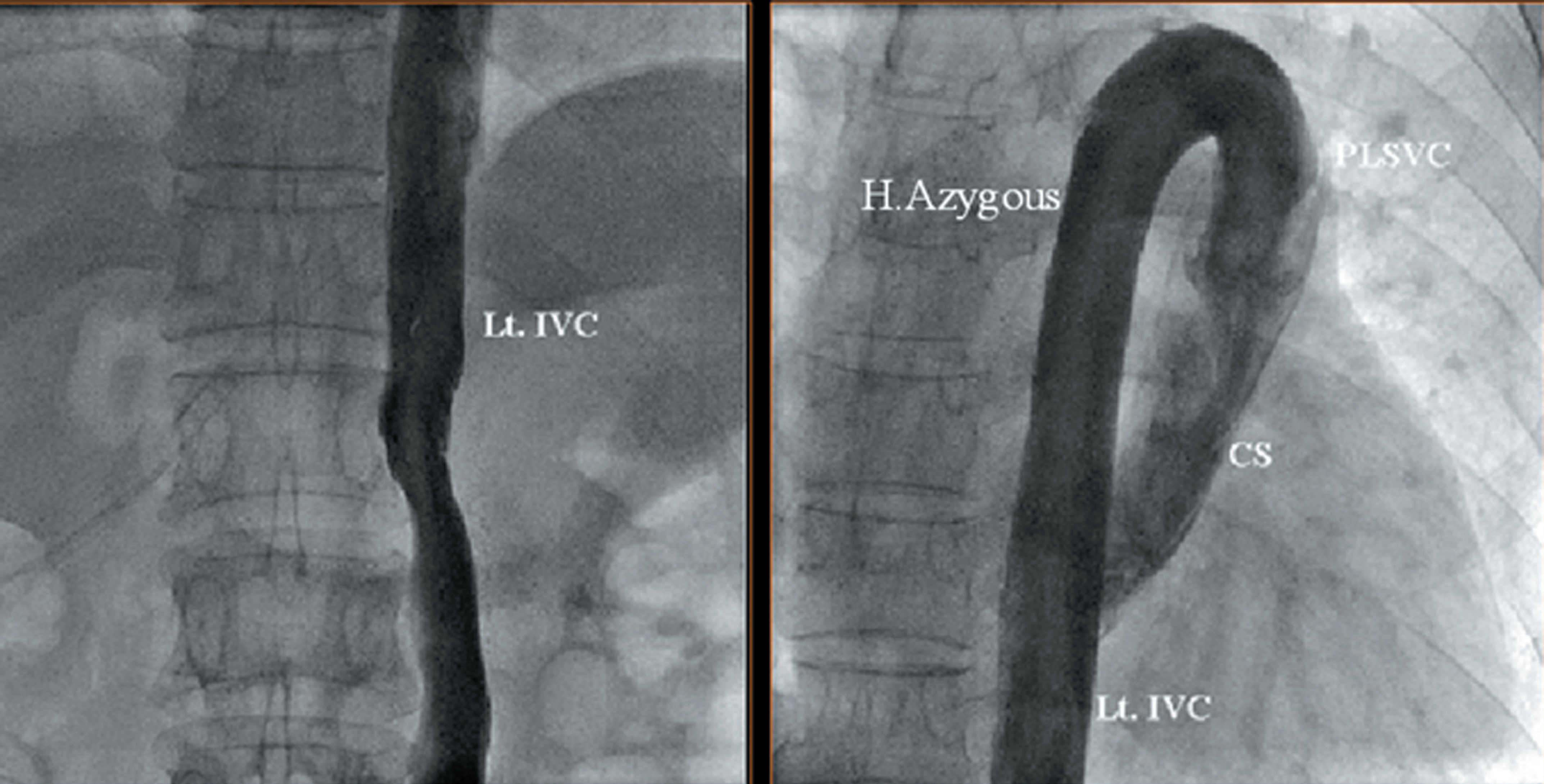
A 30-year-old man presented with breathlessness on exertion (New York Heart Association functional class II) for 1 year. The physical examination was unremarkable. Cardiovascular examination revealed right ventricular enlargement with a normal 1st heart sound and a wide and fixed split 2nd heart sound. There was a constant ejection click and an ejection systolic murmur grade IV/VI in the pulmonary area. Electrocardiogram showed heart rate of 90 beats/min, with P-wave positive in leads I and II, biphasic in lead III, flat in lead aVF with an axis of −30°, and right ventricular hypertrophy (Figure 1). There was no RSVC shadow and an extra structure in the area of the aortic knob and upper mediastinum on chest radiography (Figure 2). Ultrasonography of the abdomen showed normal visceral organ position and anatomy suggesting situs solitus. A 2-dimensional echocardiogram revealed ostium secundum ASD and pulmonary valve stenosis with a Doppler gradient of 60 mm Hg. The coronary sinus was grossly dilated with an LSVC draining into it. Cardiac catheterization was performed through the right femoral and internal jugular veins. A venogram via the femoral vein demonstrated a left-sided IVC draining into the LSVC via the hemiazygous vein (Figure 3). A venogram via the internal jugular vein showed absent RSVC and the brachiocephalic vein communicating with the LSVC that drained into the right atrium through the grossly dilated coronary sinus (Figure 4). All the pulmonary veins drained into the left atrium. There was a 15% step-up of oxygen saturation from the coronary sinus to the right atrium. The calculated pulmonary-systemic shunt flow ratio was 1.8:1. The patient underwent surgical closure of his ASD. Operative findings confirmed the venacaval anomalies and also revealed hepatic veins draining directly into the right atrium. Cardiopulmonary bypass was established by cannulating the aorta, the LSVC (extra-pericardial portion), and 2 hepatic veins. Myocardial protection was accomplished using antegrade blood cardioplegia. The ASD was closed with a Dacron patch, and pulmonary valve commissurotomy was performed through the pulmonary artery. Postoperative recovery was uneventful.
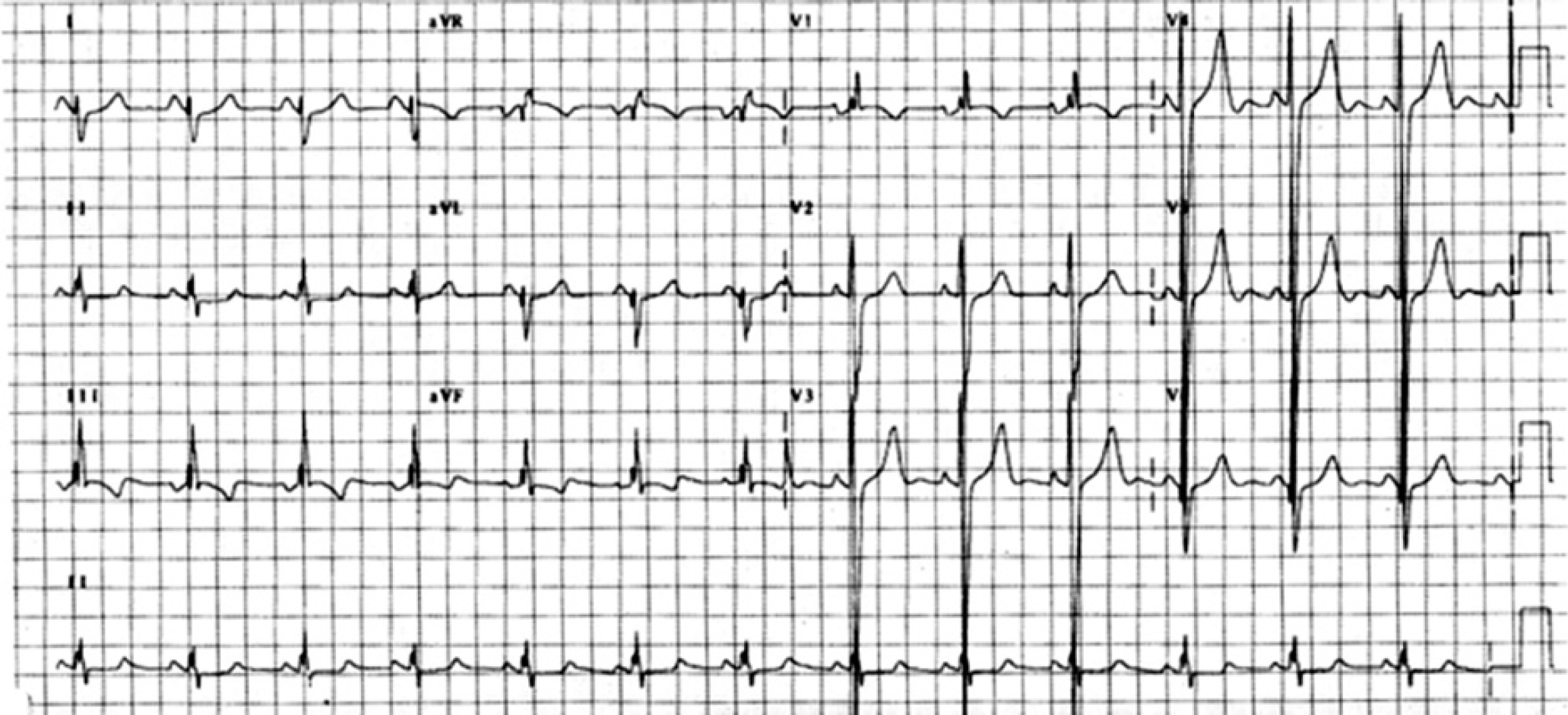
Twelve-lead electrocardiogram showing right ventricular enlargement with ectopic atrial rhythm.
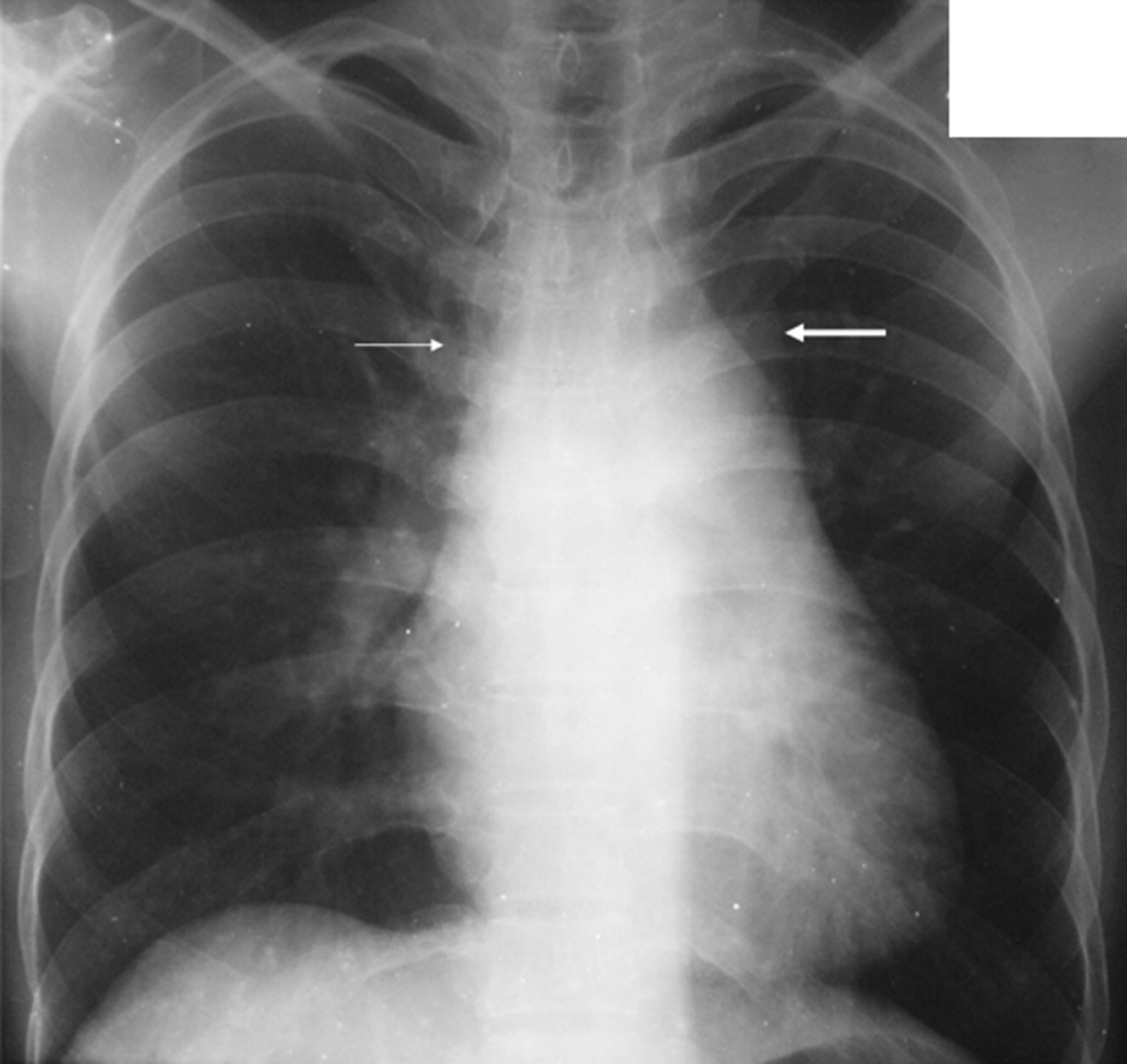
Chest radiograph showing absent right superior vena caval shadow (thin arrow) and a left superior vena cava shadow (thick arrow).
(
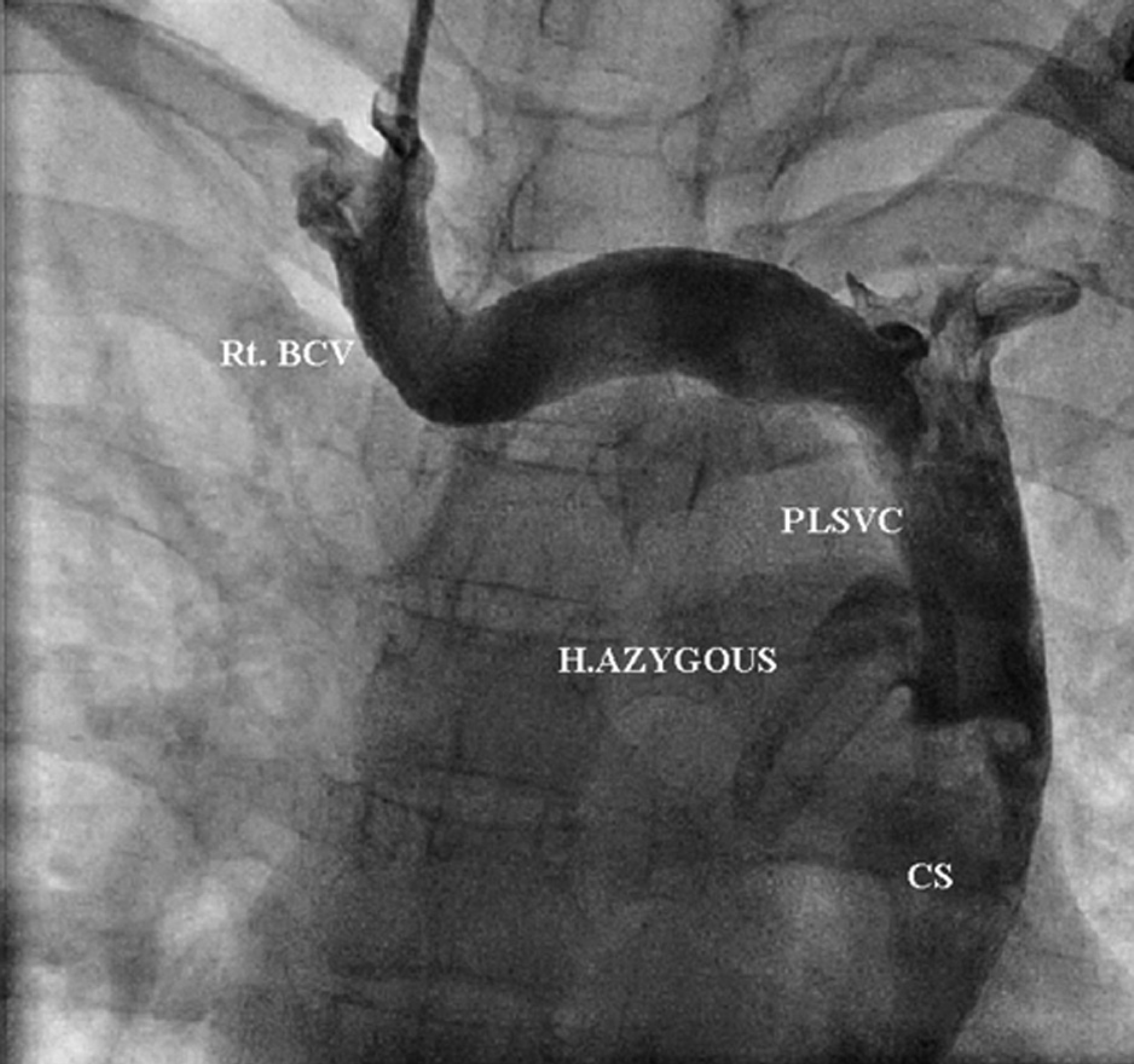
Right jugular venogram showing the right brachiocephalic vein (Rt. BCV) draining into the persistent left superior vena cava (PLSVC) which in turn drains into the coronary sinus (CS). H. Azygous = hemiazygous vein.
Discussion
In persistent LSVC, the fetal anterior cardinal vein does not regress. Absent RSVC with persistent LSVC may be seen in cases of heterotaxy, mirror image dextrocardia, situs inversus and visceral transposition. 3 However, persistent LSVC with absent RSVC and visceroatrial situs solitus is very rare and accounts for only 1% of cases of persistent LSVC and 0.09% of autopsied cases of congenital heart disease. 1,4 Bartram and colleagues 1 found cardiac malformations in 46% of patients in an analysis of 121 with LSVC and absent RSVC; ASD was noted in 16%. Our patient also had severe pulmonary valve stenosis. To our knowledge, this combination of cardiac malformations has not been described previously.
Sinoatrial node dysfunction with normal sinus rhythm or ectopic atrial rhythm has been observed in patients with LSVC, absent RSVC, and situs solitus. 4 Histology shows hypoplastic sinoatrial node and, rarely, atrioventricular node. 1 Our patient also had predominantly ectopic atrial rhythm, probably secondary to sinoatrial node dysfunction. IVC anomalies are not uncommon, and there are several variations. Left-sided IVC results from persistence of the left supracardiac vein; it usually crosses back to the right side after receiving the renal veins, to enter the right atrium in the normal manner. 5 Alternatively, a left-sided IVC may communicate with the azygous vein and drain into the SVC. Rarely, a left IVC communicates with a persistent LSVC through the hemiazygous vein, as in our patient. 2
Venacaval anomalies may have serious implications for procedures on the right side of the heart. Technical difficulties in temporary and permanent pacing in patients with a left IVC draining to an LSVC with absent RSVC have been emphasized in several case studies. 6,7 During cardiac surgery, LSVC is a relative contraindication to retrograde cardioplegia. 3 The coronary sinus catheter balloon may not completely occlude the dilated coronary sinus, resulting in failure to ensure retrograde flow to the myocardium, or flow may be largely distributed to the left internal jugular and left subclavian veins. Antegrade cardioplegia was used in our patient. For cardiopulmonary bypass, it is advisable to cannulate the LSVC at its extrapericardial portion to avoid trauma to the coronary sinus and its ostium which are close to the atrial pacemaker for coronary sinus rhythm. In patients with LSVC, diagnosis of absent RSVC is important for placement of a pulmonary wedge catheter (usually carried out without fluoroscopy), in systemic venous cannulation for extracorporeal membrane oxygenation, in partial or total cavopulmonary anastomoses where preoperative knowledge of venous anatomy is essential, and for orthotopic heart transplantation that needs repeated endomyocardial biopsies via the right internal jugular or femoral vein. 1