
Abstract
Composite replacement is the standard approach for repair of acute type A aortic dissection involving the aortic root. Reimplantation or remodeling procedures have become valve-sparing alternatives. We developed a new and simple technique to stabilize the aortic root. A Dacron graft is attached outside the native aortic cylinder, and incised twice vertically to create openings corresponding to the right and left coronary ostia. Thus the entire graft covers the native aortic root cylinder from the outside, and the native aortic valve and coronary ostia do not need to be reimplanted. From 2002 to 2007, this technique was applied in 14 patients (8 male) with a mean age of 71 years (range, 34-83 years). Four patients died within 30 days; 3 had been hemodynamically unstable with ventilator and inotropic support preoperatively. Echocardiography showed normal function of the preserved aortic valve, without regurgitation, in all patients. This technique is an alternative valve-sparing method for stabilization of the aortic root in patients with acute type A aortic dissection.
Keywords
Introduction
The standard approach for repair of acute aortic dissection type A (AADA) involving the aortic root is replacement of the aortic valve, root, and ascending aorta with a composite graft carrying a mechanical or biological prosthesis. 1 In the case of a nonpathologic aortic valve, reimplantation or remodeling procedures have become valve-sparing alternatives; 2,3 however, both techniques are more demanding than the standard composite replacement method. Supra-commisural replacement of the ascending aorta with repair of the dissected root is another alternative, but it bears the risk of root aneurysm formation or late necrosis, especially when surgical glue is used. 4 –7 We report the early results of an alternative valve-sparing aortic root stabilizing technique for AADA involving the aortic root. 8
Patients and Methods
Between December 2002 and October 2007, 14 patients were operated on using the procedure described herein. This technique was not specifically approved by our institutional review board because no standard of care has been defined in guidelines for this difficult patient population treated under emergency conditions. Patient demographics and clinical data are listed in Table 1. Diagnosis of AADA was established by computed tomography and/or transesophageal echocardiography. Most patients were diagnosed in other hospitals and transferred to our institution for emergency surgery.
Profile of 14 patients undergoing aortic root stabilization
Including the patient with a hybrid prosthesis.
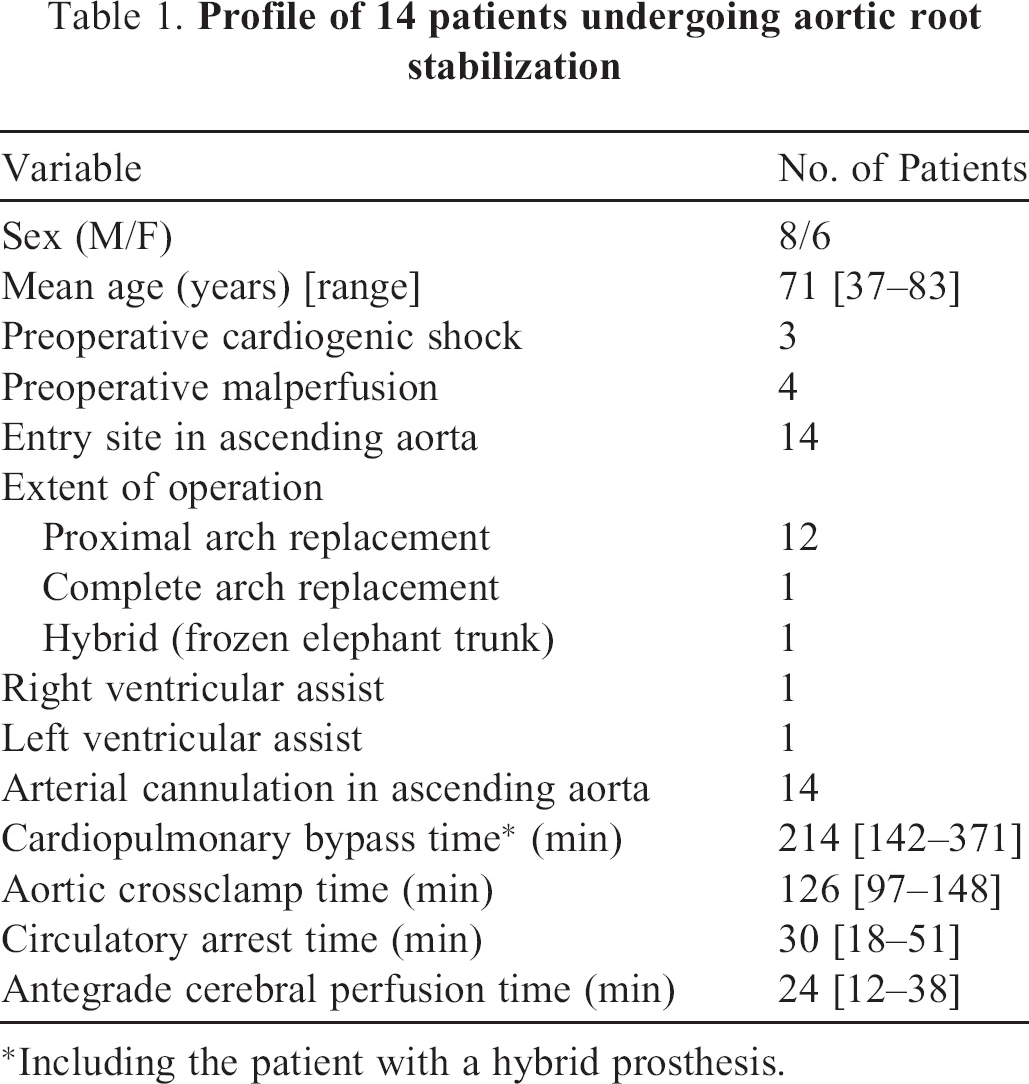
The surgical approach was always via a median sternotomy. The protocol for myocardial and cerebral protection has been published recently by our group. 9 The ascending aorta was used for arterial cannulation. The patients were cooled to a rectal temperature of approximately 26°C. Myocardial protection was achieved with repeated doses of antegrade cold blood cardioplegia. The extent of surgery depended on the pathology. A valve-sparing operation was applied whenever possible. If the aortic root was involved, the decision regarding any further procedure was taken after careful inspection. If the aortic valve was structurally abnormal or calcified, replacement with a biological or mechanical composite was undertaken. If the valve itself was normal but the aortic sinus and annulus were dilated, a valve-sparing reimplantation (David) or remodeling (Yacoub) technique was performed. 2,3 If the aortic valve was normal and the aortic root not dilated, our new technique was used. The aorta was transected just above the valve commissures. The entire base of the aortic root was dissected below the level of the aortic annulus, and measured with a commercially available mechanical valve sizer. The graft was implanted outside the native aortic cylinder, using 12 braided 2/0 polyester mattress sutures (Ethibond, Ethicon, Inc., Hamburg, Germany) placed in the left ventricular outflow tract in a horizontal plane 2–3 mm below the lowest level of the valve leaflets. These sutures later corresponded to the size of the graft. The Dacron graft was incised twice vertically to create openings corresponding to the right and left coronary ostia (Figure 1A). Thus the entire graft covered the native aortic root cylinder from the outside (Figure 1B). The 2 incisions in the graft for the coronary ostia were closed proximally by the corresponding sutures of the proximal suture line. The graft skirt for the coronary arteries was not sutured to the sinuses. The native aortic valve and the coronary ostia do not need to be reimplanted. Distal aortic reconstruction was undertaken under moderate hypothermic circulatory arrest and selective antegrade cerebral perfusion. Weaning from extracorporeal circulation and completion of the operation were conducted in the routine fashion. Aortic valve function was evaluated echocardiographically intraoperatively and before discharge in all patients. Computed tomography was carried out before discharge and during follow-up.
Results
In all 14 patients, the entry site of the dissection was found in the ascending aorta (Table 1). Four patients died within 30 days: one suffered a preoperative iatrogenic AADA during rescue percutaneous transluminal coronary angioplasty after myocardial infarction, and died later due to right heart failure; another was admitted under resuscitation due to pericardial tamponade and could not be weaned from cardiopulmonary bypass; the 3rd died intraoperatively due to left heart failure; and the 4th developed multiorgan failure with sepsis in the intensive care unit. The mean duration of follow-up was 17 months (range, 1–48 months). Echocardiography showed aortic valve insufficiency ≤ grade I, and all patients were in New York Heart Association functional class I or II. Computed tomography revealed normal dimensions of the aortic root (Figure 2), and the natural aortic sinuses and sinotubular shape appeared to be preserved.

Angio-computed tomography of the aortic root at follow-up.
Discussion
Surgical repair of the aortic root in AADA is still a challenge for cardiothoracic surgeons. Recently, the David reimplantation or Yacoub remodeling approach have become alternatives to the gold standard of composite replacement. 2,3 These are elegant techniques in hemodynamically stable patients, but require extended cardiopulmonary bypass times. Therefore, some surgeons still perform aortic valve-sparing supra-commisural aortic replacement with a tube graft, just gluing or suturing the dissected wall of the aorta. This may offer a simple and quick alternative, but leaves the diseased aortic tissue in place, and may result in repeat dissection or aneurysm formation, leading to reoperation. Furthermore, necrosis due to the use of glue has been reported. 4 –7
Graeter and colleagues 10 compared composite and supra-commisural replacement, remodeling, and reimplantation, with regard to aortic regurgitation and proximal aortic reoperation 2 years postoperatively. Despite limited numbers of patients, both valve-sparing techniques showed good results, while supra-commisural replacement was associated with more reoperations for secondary aortic insufficiency. Kallenbach and colleagues 11 described our experience with 284 patients undergoing reimplantation techniques, including 53 with AADA, confirming that it is a reliable method. Despite this, reimplantation of the coronary ostia can be challenging in AADA, so we developed this alternative valve-sparing aortic root stabilization technique to simplify the procedure and avoid the use of glue. Our department policy forbids refusal of surgery to any patient presenting with AADA because of age, unknown neurological status, or hemodynamic instability. This is reflected in the relatively high mortality rate.
The technique described here is suitable for patients with a dissected aortic root but normal aortic valve. This procedure avoids time-consuming reimplantation of the coronary ostia, and it is especially useful when the coronaries are involved in the dissection. Although the dissected wall of the aortic sinus is retained, we have not seen any dilatation of the aortic sinus or the root during follow-up. Despite the small number of patients in this study, it seems that the technique is a feasible alternative valve-sparing method in selected patients with AADA and a morphologically intact aortic valve. It is much simpler than either the remodeling and reimplantation technique.
Footnotes
Presented at the 15th Annual meeting of the Asian Society of Cardiovascular Surgery, Beijing, China, May 17–20, 2007.