
Abstract
A simple reliable maneuver to optimize exposure of the left atrium for mitral valve operations is described. It offers more space to mobilize the valvular structure, facilitating complicated reconstruction in the posteromedial commisural area.
Introduction
Excellent and consistent exposure of the mitral valve is the key to successful valve repair or replacement. A right lateral incision between the confluence of the right pulmonary veins and the interatrial groove is the standard approach for mitral operations. 1,2 However; this approach usually gives limited operative vision towards the posteromedial commissural area because of plication of the left atrium. A simple method to optimize mitral valve exposure is described.
Technique
After a median sternotomy and aortic bicaval or single 2-stage atrial cannulation, standard cardiopulmonary bypass is initiated. The heart is arrested with cold crystalloid cardioplegia. A standard lateral left atriotomy is made after dissecting the interatrial groove. The incision is extended behind the superior vena cava and posteriorly below the inferior vena cava, as far as necessary to sure the atriotomy is of adequate size. To expose the left atrium, 2 retractor blades are fixed to the bar of a standard self-retaining retractor. After this maneuver, plication of the left atrium usually hinders the view towards the posterior annulus at P2-P3 and the posteromedial commissural area (Figure 1A). A pledgeted 4/0 Prolene suture is attached at the upper or middle part of the plication (Figure 1B), and traction is gently applied. The end of the suture is fixed with a clamp (Figure 2A). More space is now provided and mitral valve repair or replacement can be performed comfortably (Figure 2B). After removal, the 4/0 Prolene suture can be used for closure of the left atriotomy.
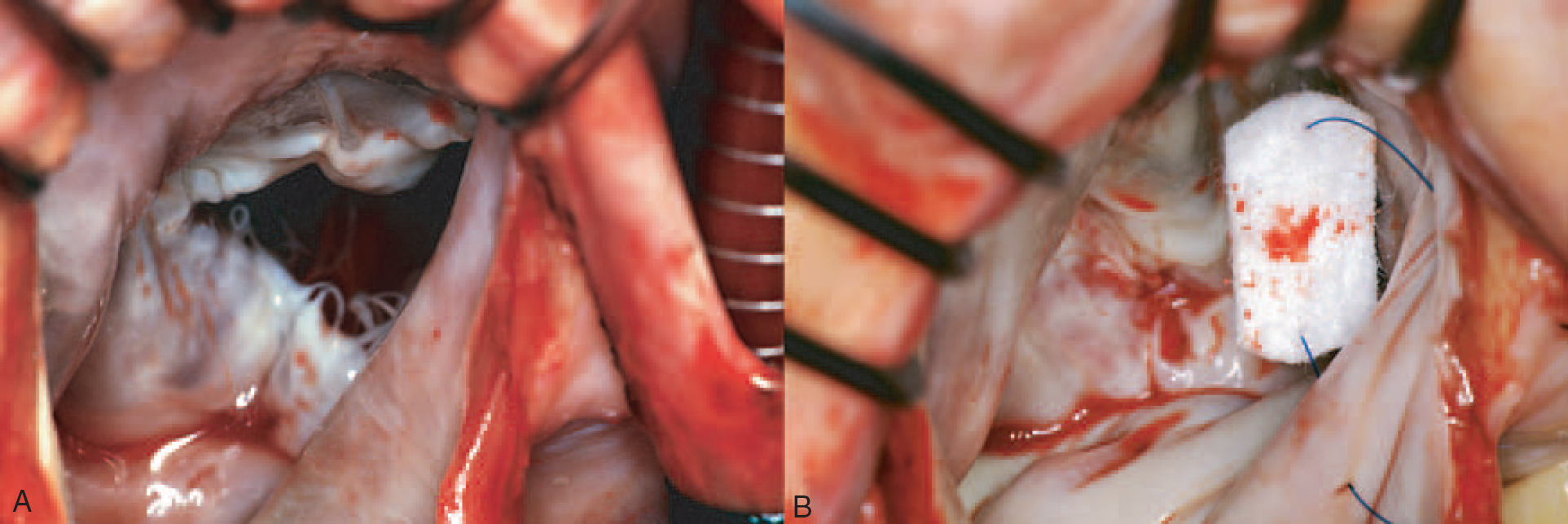
(A) Conventional exposure of the mitral valve, with clearly visible plication of the left atrial wall towards the posterior annulus at P2-P3 and the posteromedial commissural area. (B) The pledgeted suture is placed.
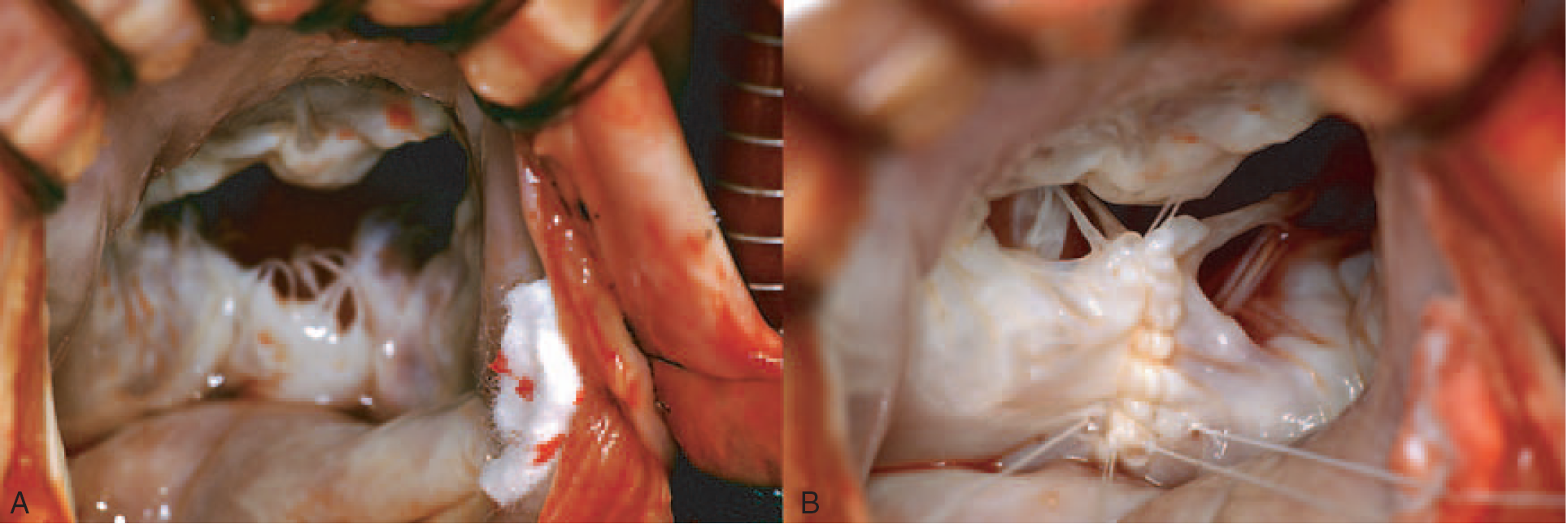
(A) Tightening the suture gives excellent exposure of the posteromedial commissural area; (B) After successful mitral valve repair.
Discussion
We have applied this technique routinely in 715 patients undergoing mitral valve procedures in the past 10 years; 93 were treated using a single venous cannula and a ministernotomy in the last 2 years. Successful mitral valve repair was achieved in 95%, with no complications such as bleeding, tissue tearing, ischemic damage, or arrhythmias.
Although the conventional left atriotomy is safe, with a low risk of losing sinus rhythm, the posteromedial commissural area is poorly exposed because of plication of the left atrial wall. 3 To overcome this problem, an angled rectractor is inserted by an additional assistant, or a 3rd self-retaining retractor blade is used; both of these methods limit the surgeon's maneuverability. Inconsistent traction with an angled retractor may tear the tissue and complicate the surgery. The technique described here gives excellent exposure by stretching the left atrium with the posterior annulus area. This enables precise placement of annuloplasty sutures, avoids iatrogenic injury of the underlying circumflex artery, and makes accurate annuloplasty ring implantation easier. Furthermore, the mitral valve plane is brought towards the surgeon, and the repair architecture is stabilized, which allows more space and easier surgery, with significant time-saving. Because the right pulmonary veins are accessible, ablation can also be performed for atrial fibrillation. The limitation of this technique is extensive left atrial dilatation where the tissue is fragile. To prevent tearing or bleeding, we recommend using 5/0 Prolene with a small needle. Caution is needed to avoid pulling the suture too tight.
It is worth mentioning that surgeons who frequently practice this technique acknowledge the ease is affords. The improved vision offers teaching opportunities during the operation, and a 2nd surgical assistant is not required, which is especially helpful in emergency situations where extra manpower is not always available. The suture is not wasted as it can be used for atrial closure. We consider that this suture technique can simplify all mitral valve procedures and contribute to improved results.