
Abstract
Bronchogenic cysts are usually discovered only incidentally in the adult. A giant bronchogenic cyst in a 19-year-old woman presenting with pain and shortness of breath was mistaken for tension pneumothorax and initially treated with tube thoracostomy. Giant bullae were diagnosed by computed tomography. Bullae resection was undertaken, but the remaining lung tissue required pneumonectomy. Pathologic examination of the specimen confirmed bronchogenic cyst.
Keywords
Introduction
Bronchogenic cysts with tracheobronchial involvement very rarely present as tension pneumothorax. 1 Unnecessary chest tube drainage is common. We describe such a case of mistaken tension pneumothorax, which was treated as such in the emergency room.
Case Report
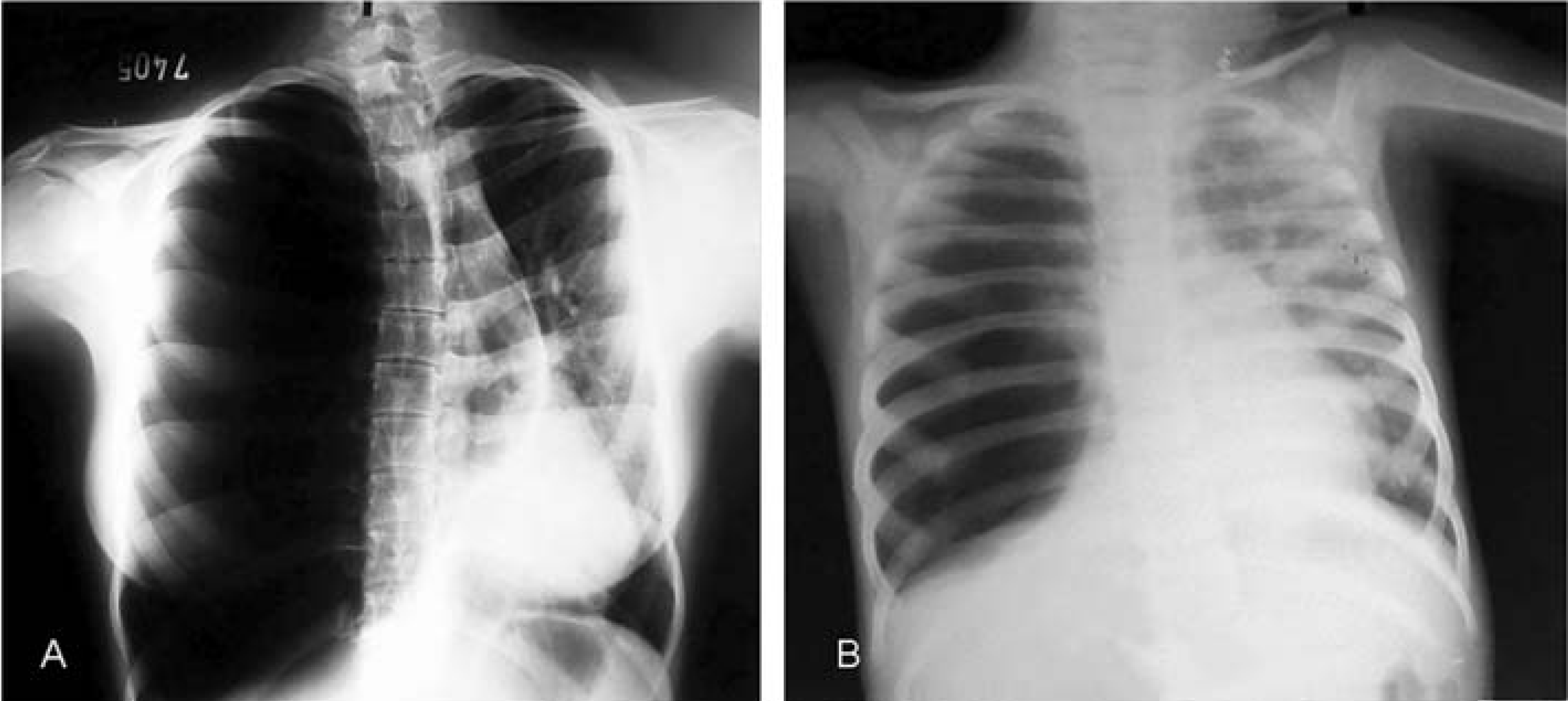
A 19-year-old woman was referred to the emergency department of our hospital with shortness of breath and sudden pain in the right hemithorax. No breath sounds could be heard on her right side. Chest radiography revealed hyperaeration in the right hemithorax with a mediastinal shift to the contralateral side, leading to a diagnosis of tension pneumothorax (Figure 1A). Chest tube drainage was performed using a 32F thoracic drain. Subsequent chest radiography did not show any improvement. Further questioning of the family revealed an untreated respiratory disease in childhood, and a chest radiograph taken at that time was found (Figure 1B). The patient had subsequently displayed reduced physical activity. Computed tomography of the thorax revealed huge air-filled cysts with septa (Figure 2). A right thoracotomy was performed, and the bullous parts of the right lung were resected. As the remaining lung tissue was immature and did not respond to forced ventilation, pneumonectomy was carried out (Figure 3). Histopathological examination of the specimen revealed a cyst lined with normal ciliated respiratory epithelium, which was diagnosed as a bronchogenic cyst. After 5 years of follow-up, the patient was well and had given birth to a healthy baby girl. During follow-up, she needed only physical therapy and pain killers for dorsal pain and a slight scoliosis in the vertebral column, probably due to postoperative pain.
(
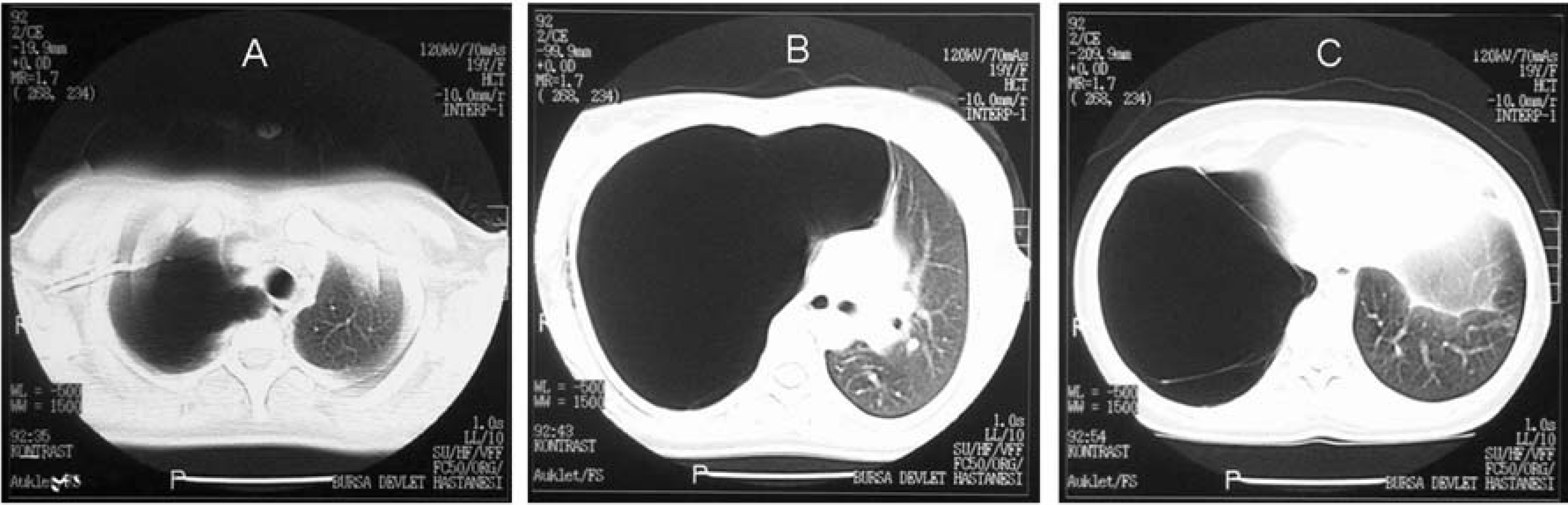
Thoracic computed tomography revealing a huge air space with interlobular fibrous septa.
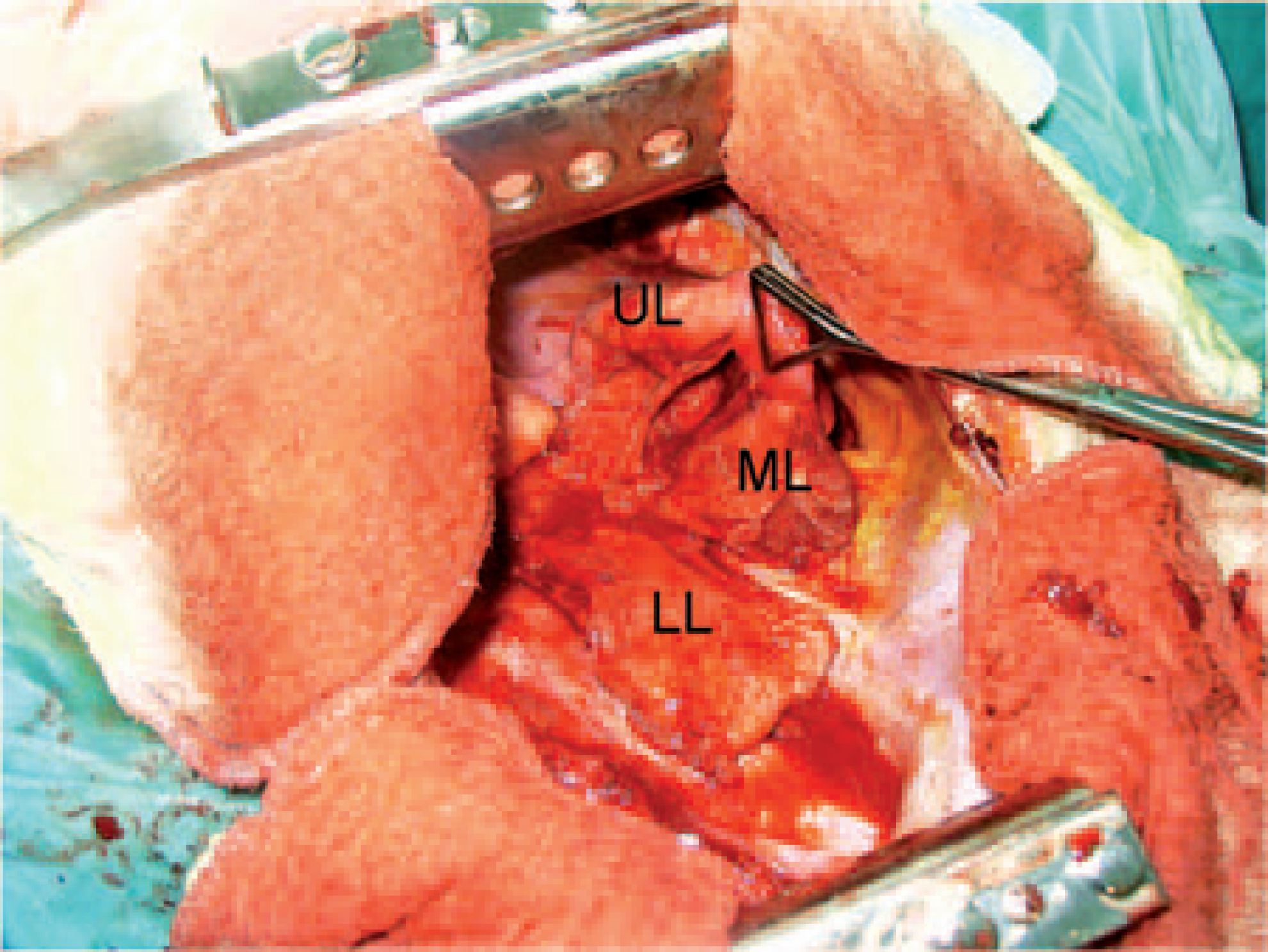
Intraoperative photograph showing the lung remnant which was unable to expand following cyst resection, leading to pneumonectomy. LL = lower lobe, ML = middle lobe, UL = upper lobe.
Discussion
Encountering a developmental lung anomaly in an adult can be a challenge because the abnormality may be mistaken for something more sinister. The common anomalies encountered are classified into 3 broad categories: bronchopulmonary (lung bud), vascular, and combined lung and vascular anomalies. Lung bud anomalies include agenesis, congenital bronchial atresia, congenital lobar emphysema, congenital cystic adenomatoid malformation, pulmonary bronchogenic cysts, tracheal or pig bronchus, and accessory cardiac bronchus. 2 Congenital lung cysts such as congenital cystic adenomatoid malformation, pulmonary sequestration, congenital lobar emphysema, and bronchogenic cysts are rare but fascinating anomalies of lung development. 3 Congenital cystic adenomatoid malformation, pulmonary sequestration, congenital lobar emphysema, and bronchogenic cysts are detected in imaging studies as abnormal air-, air/fluid-, or fluid-filled cysts. Computed tomography has proved to be an extremely useful tool in the differential diagnosis of these lesions. 4
In a report on the clinical spectrum of such cases, all patients <1-year old showed respiratory distress with mediastinal shift but no episodes of infection, whereas 13 of 19 patients >1-year old had symptoms of recurrent infection without respiratory distress; 5 were entirely asymptomatic from birth. 5 Our patient suffered from respiratory distress at 1.5-years old and had no further symptoms until she was 19-years old. Basic resection of the cyst is usually effective treatment. Coran and colleagues 6 studied 44 consecutive cases treated for cystic pulmonary diseases; all patients with congenital cystic adenomatoid malformation, congenital lobar emphysema, and intralobar pulmonary cysts were treated by lobectomy; no segmentectomy was performed. Extralobar pulmonary cysts and bronchogenic cysts were managed by resection of the cyst alone. 6 Evrard and colleagues 7 performed lobectomy in 22/48 cases, whereas more lung-preserving surgery, such as enucleation or sequestrectomy, was undertaken in the others. Takeda and colleagues 5 performed lobectomy in 21 patients, excision in 3, segmentectomy in one, and exploration alone in one. Surgical excision by segmentectomy or lobectomy for intrapulmonary lesions and simple excision for extralobar sequestrations and bronchogenic cysts are safe and have a low incidence of complications. 4
Recently, pneumothorax and a cystic formation in the right hemithorax were found on chest radiography in an 18-month-old girl with high fever and vomiting, who was treated by simple wedge resection. 1 Had our patient been diagnosed when she was 1.5-years old, simple resection of the bronchogenic cyst might have been sufficient. Unfortunately, she required pneumonectomy. We believe that early recognition of these relatively rare congenital cystic lung lesions would lead to immediate proper surgical intervention. In adult cases like ours however, lobectomy or even pneumonectomy might be necessary.