
Abstract
We retrospectively reviewed 128 consecutive patients who underwent quadrangular resection of a prolapsed posterior mitral leaflet and local suture annuloplasty. The median age was 68.1 ± 10.0 years (range, 30–84 years) and 63.3% were male. Mean left ventricular ejection fraction was 63.8% ± 10.2% (range, 25%–80%). The etiology of mitral regurgitation was fibroelastic degeneration in 94 (73.4%) patients, myxomatous degeneration in 26 (20.3%), myxomatous infective endocarditis in 7 (5.5%), and post-infarction papillary rupture in one. There was 1 (0.8%) hospital death. The median follow-up was 4.7 ± 4.7 years (range, 0.01–18.29 years). The freedom from reoperation was 98%, 94%, 87%, and 79% at 1, 5, 10, and 15 years, respectively, improving for the most recent 107 patients, subsequent to technical modification, to: 100%, 96%, 94%, and 90% at 1, 5, 10, and 14 years, respectively. Ten- and 15-year freedom from severe mitral regurgitation was 91%, and 88%, respectively. The overall actuarial 1-, 5-, 10-, and 15-year survival rates were 98%, 90%, 70%, and 52%, respectively, similar to that of the age- and sex-matched United Kingdom population. The long-term results of this technique in selected patients with prolapsed posterior leaflet were considered acceptable.
Keywords
Introduction
Mitral valve repair is the preferred treatment for mitral regurgitation (MR). Current operative techniques incorporate an annuloplasty ring for stability and durability. However, the ring has drawbacks and potential hazards: flattening of the normal annular saddle shape (affecting transmitral flow), posterior leaflet immobilization, systolic anterior motion obstructing the left ventricular (LV) outflow tract, hemolysis, and structural injury to the atrioventricular node and the circumflex artery. Early restoration of mitral competency, allowing preservation of LV function, should obviate the need for mechanical fixation of the mitral annulus. Alternatively, local annular suture plication may reduce and stabilize the annulus. This raises the possibility of mitral valve repair without an annuloplasty ring in selected patients with specific lesional profiles. We reviewed the 18-year experience of a single surgeon (RP) performing posterior mitral leaflet repair using local suture annuloplasty.
Patients and methods
Profile of 128 patients undergoing mitral suture annuloplasty
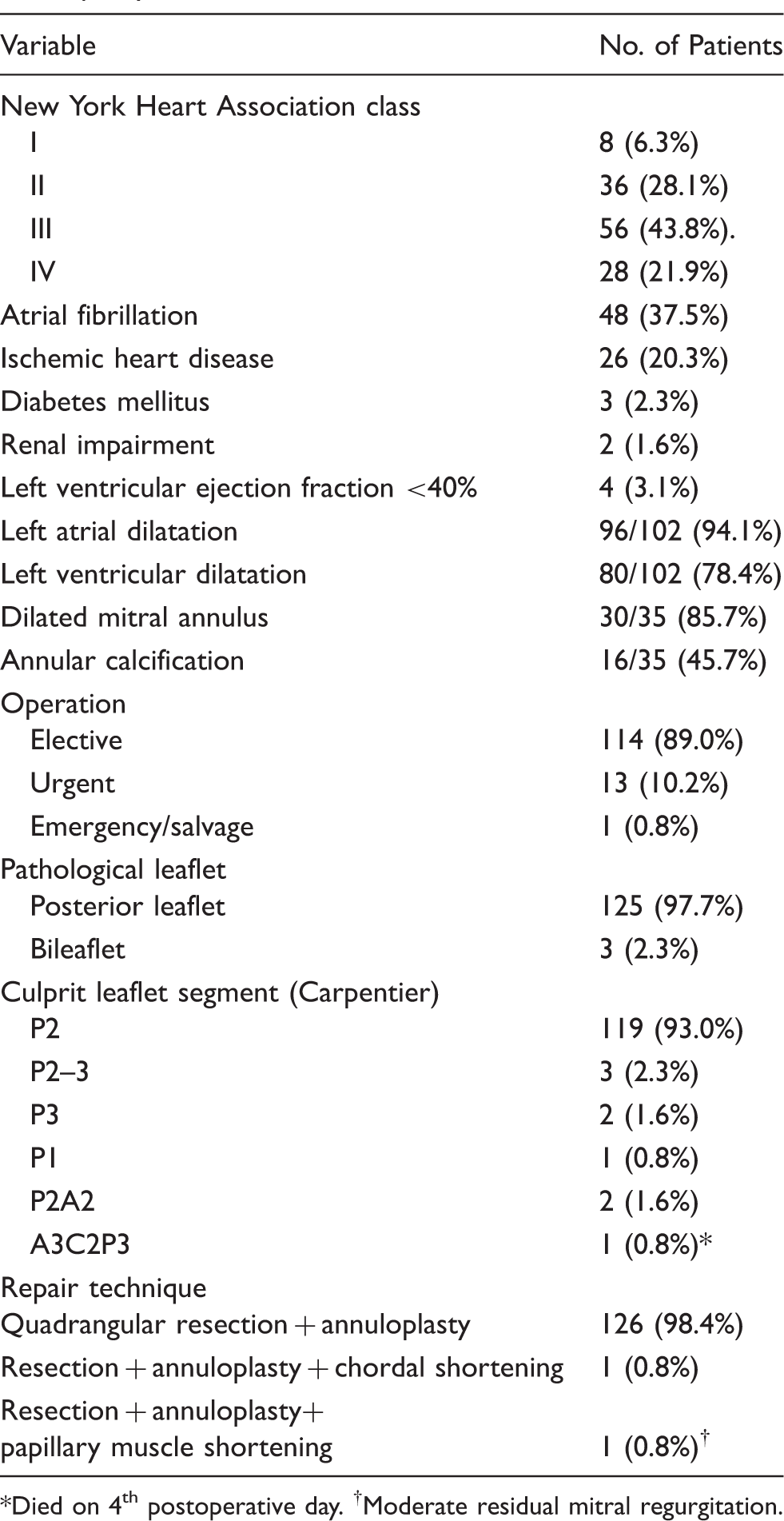
* Died on 4th postoperative day. †Moderate residual mitral regurgitation.
All patients underwent a median sternotomy. Cardiopulmonary bypass was established with standard aortic and bicaval cannulation. Myocardial protection was achieved with antegrade cold crystalloid cardioplegia and mild hypothermia. The LV apex was vented. The left atrial approach, posterior to the Sondergaard groove, was used. Bulb syringe water testing of the mitral valve confirmed the prolapsing segment, and probing with a nerve hook identified the unsupported segment and delineated the boundaries of leaflet resection. Quadrangular resection of the culprit segment was followed by local suture annuloplasty using multiple horizontal mattress 2/0 Ethibond sutures, aiming to slide and reduce the posterior annular diameter at the site of leaflet resection alone (Figure 1). The smaller annular gap was subsequently closed en mass, using interrupted 2/0 Ethibond sutures. The residual infolded annular defect was closed using figure-of-eight 2/0 Ethibond sutures biting into the left atrial wall only. The remnant medial leaflet edges were re-approximated with a continuous 5/0 Prolene suture. Water testing confirmed valve competency before the atriotomy was repaired. Intraoperative transesophageal echocardiography was routinely used from 2000.
Mitral repair technique.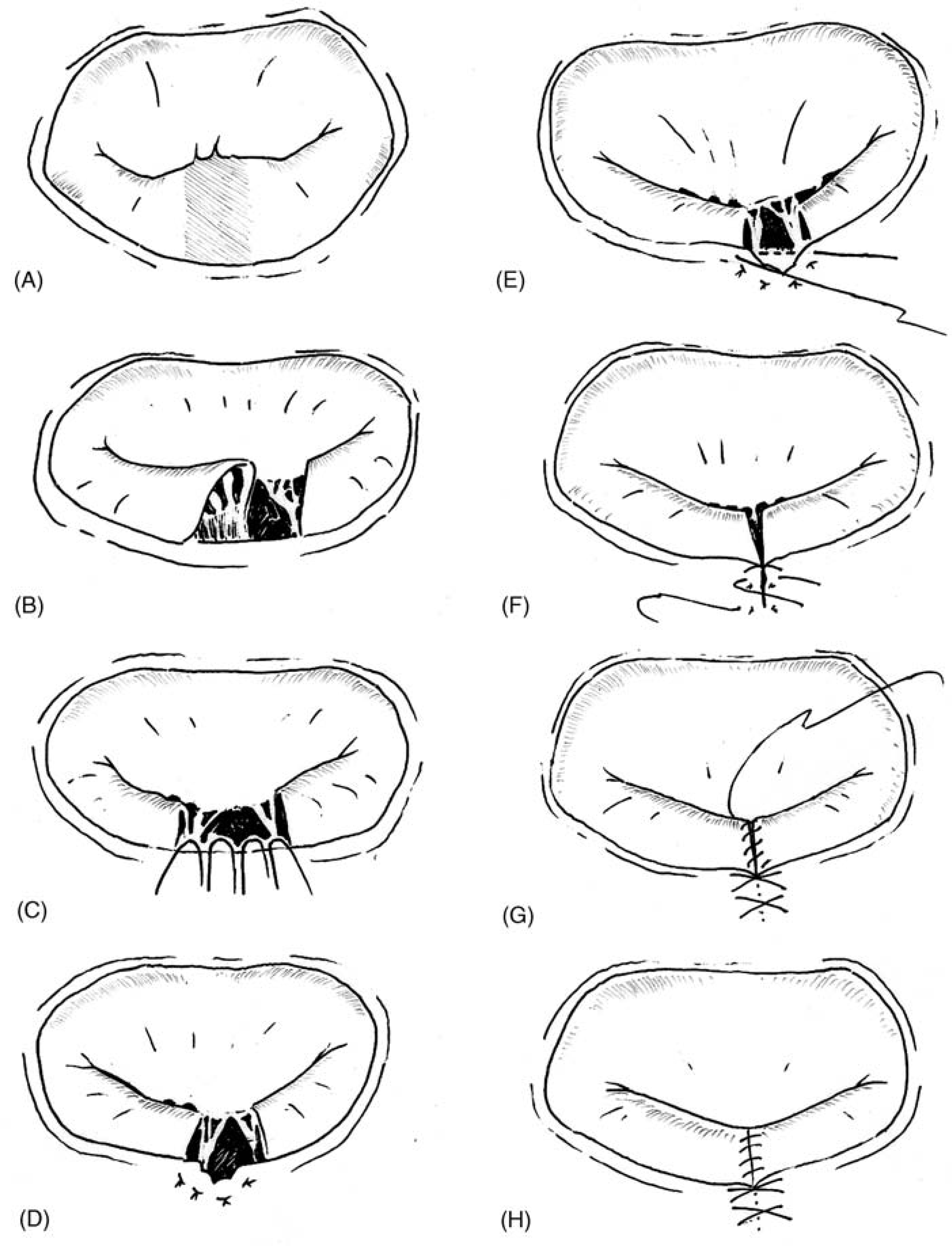
Warfarin was administered postoperatively only to patients with atrial fibrillation or a mechanical aortic prosthesis. This modified technique was performed in 107 consecutive patients from 1994, whereas a single mass annular stitch was used for earlier cases (Figure 2). Both methods were tailored to avoid the use of a supportive annuloplasty ring. Incorporation of the sliding technique with plication reduces the size of the annulus and decreases tension on the leaflet repair.
Technical modification of suture annuloplasty (lower panel).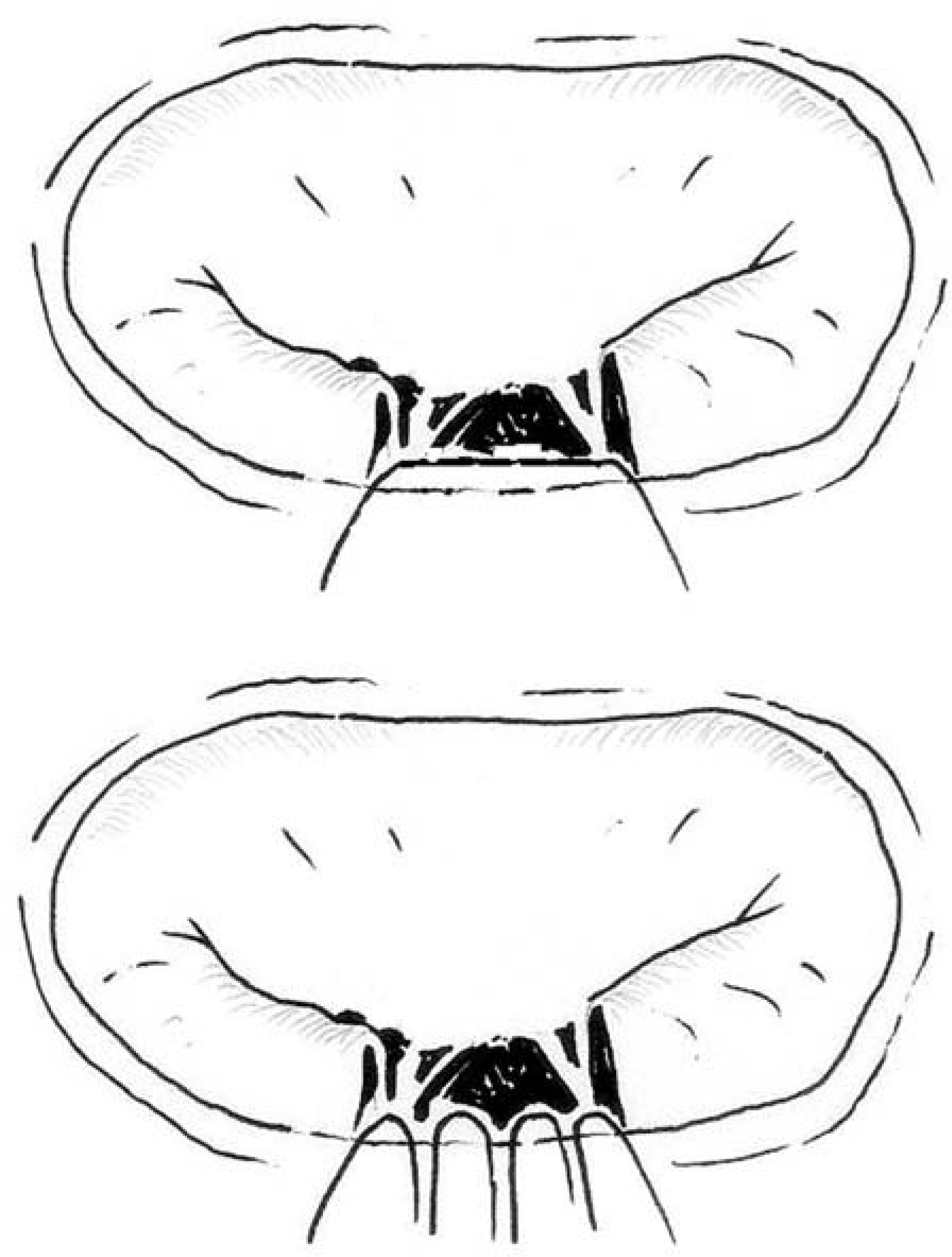
Three patients were lost to follow-up, the others were followed up at our outpatient clinic for 6.2 ± 4.7 years (range, 0.01–18.29 years). Outpatient transthoracic echocardiography was performed at the discretion of the referring cardiologist. The mean echocardiographic follow-up was 4.8 ± 4.7 years (range, 0–17.2 years). Echocardiographic data included mean mitral transvalvular gradient, the degree of residual MR (none, trivial, mild, moderate, severe), left atrial and LV dimensions, and LV ejection fraction.
Statistical analysis was carried out using SPSS version 16.0 for Windows (SPSS, Chicago, IL, USA). Student’s t test was used to analyze normally distributed continuous data. Values are expressed as mean ± standard deviation. Fishers exact test or the chi-squared test was used for categorical variables that are expressed as percentages. A p value < 0.05 was considered significant. The Kaplan-Meier method was used for survival analysis, freedom from reoperation, and freedom from residual moderate MR. The age- and sex-matched survival rate of the general UK population was obtained from the Office for National Statistics website (http://www.statistics.gov.uk/STATBASE/ssdataset.asp?vlnk = 9552).
Results
There was one (0.8%) hospital (30-day) death. There was no intraoperative conversion to mitral valve replacement. Reoperation was required in 13 (10.2%) patients: for replacement with a mechanical prosthesis in 11, to insert a biological prosthesis in 1, and repeat repair in 1. The mean period to reoperation was 5.1 ± 4.4 years (range, 0.1–13.8 years), with 3 patients undergoing redo surgery within the 1st postoperative year. Overall freedom from reoperation was 98%, 94%, 87% (n = 45), and 79% (n = 11) at 1, 5, 10, and 15 years. Female patients were older at the time of reoperation: 69.1 ± 7.9 years (n = 47) vs. 64.3 ± 10.6 years (n = 81) in males (p = 0.008). Freedom from severe MR was 99%, 95%, 91%, 88%, and 88% at 1, 5, 10, 15, and 17 years, respectively. In the most recent 107 patients, the reoperation rate was reduced to 4.7% following the technical modification (5 cases, including the single repeat repair), and the freedom from reoperation was superior: 100%, 96%, 94%, and 90% at 1, 5, 10, and 14 years. Postoperatively, atrial fibrillation occurred in 26 (20.3%) patients. Four (3.1%) patients suffered a stroke, with a single case of hemorrhagic stroke; 2 of these patients had atrial fibrillation. Two (1.6%) other patients had transient ischemic attacks after surgery.
During follow-up in 125 patients, 34 late deaths occurred. The overall actuarial survival at 1, 5, 10, 15, and 18 years was 98%, 80%, 70%, 52%, and 52%, respectively (Figure 3). NYHA status in the survivors was obtained from the referring cardiologist or the patient’s general practitioner. The NYHA functional class improved significantly from 2.4 ± 0.9 preoperatively to 1.4 ± 0.7 at the most recent examination in patients without subsequent mitral valve replacement (n = 104; p < 0.001 by paired t test). Four cardiac deaths at 5.7, 7.4, 8.3, and 12.1 years post-repair were unrelated to the mitral valve. There were 4 valve-related deaths: a 74-year-old lady with bileaflet (A3C2P3) prolapse, who underwent coronary artery bypass grafting and local suture annuloplasty, succumbed to heart failure with severe MR on the 4th postoperative day; an 82-year-old man post-P2 local suture annuloplasty with severe MR 11 months post-repair from anterior leaflet prolapse, died at 1.4 years post-repair; a 69-year-old lady who suffered a stroke (left hemiplegia), atrial fibrillation, and pneumonia after coronary artery bypass with P2 local suture annuloplasty, was found to have severe MR at 2.5 years post-repair and died 1.2 years later; and a 70-year-old lady, who was treated conservatively for recurrent severe MR 5-years post-P2 local suture annuloplasty repair, in view of her dementia, died 6.1 years post-repair at the age of 76 years. The remaining late deaths were unrelated to the mitral valve, although the cause of death was undetermined in 9 patients. The actuarial survival for the most recent 107 patients at 1, 5, 10, and 14 years was 97%, 89%, 68%, and 52%, respectively.
Kaplan-Meier survival of all patients undergoing mitral valve repair with local suture annuloplasty. The solid line represents survival of the normal UK population, the dashed lines mark the 95% confidence interval limits. *Cumulative deaths.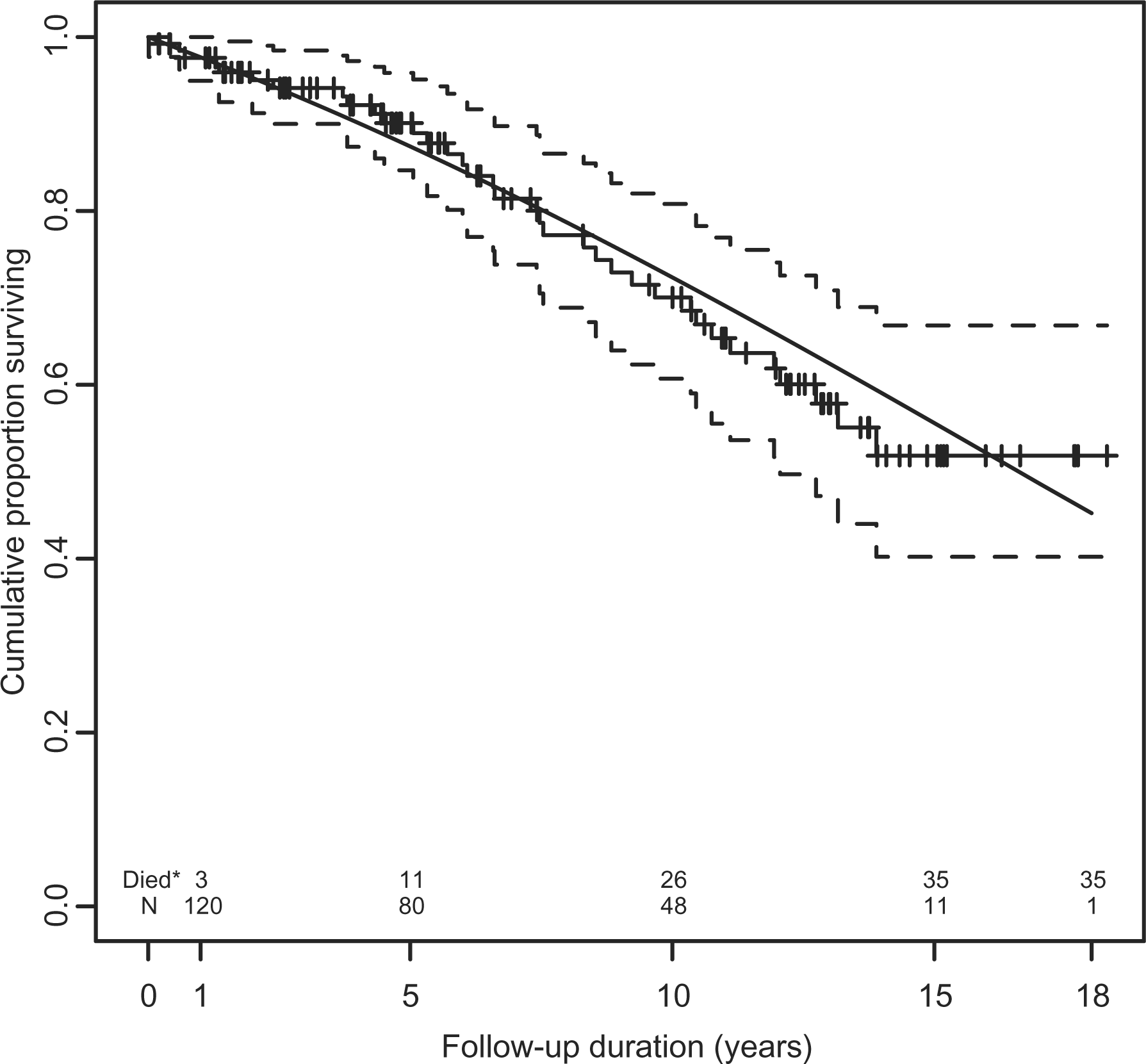
Pre- and postoperative echocardiographic and clinical data (excluding redo cases)
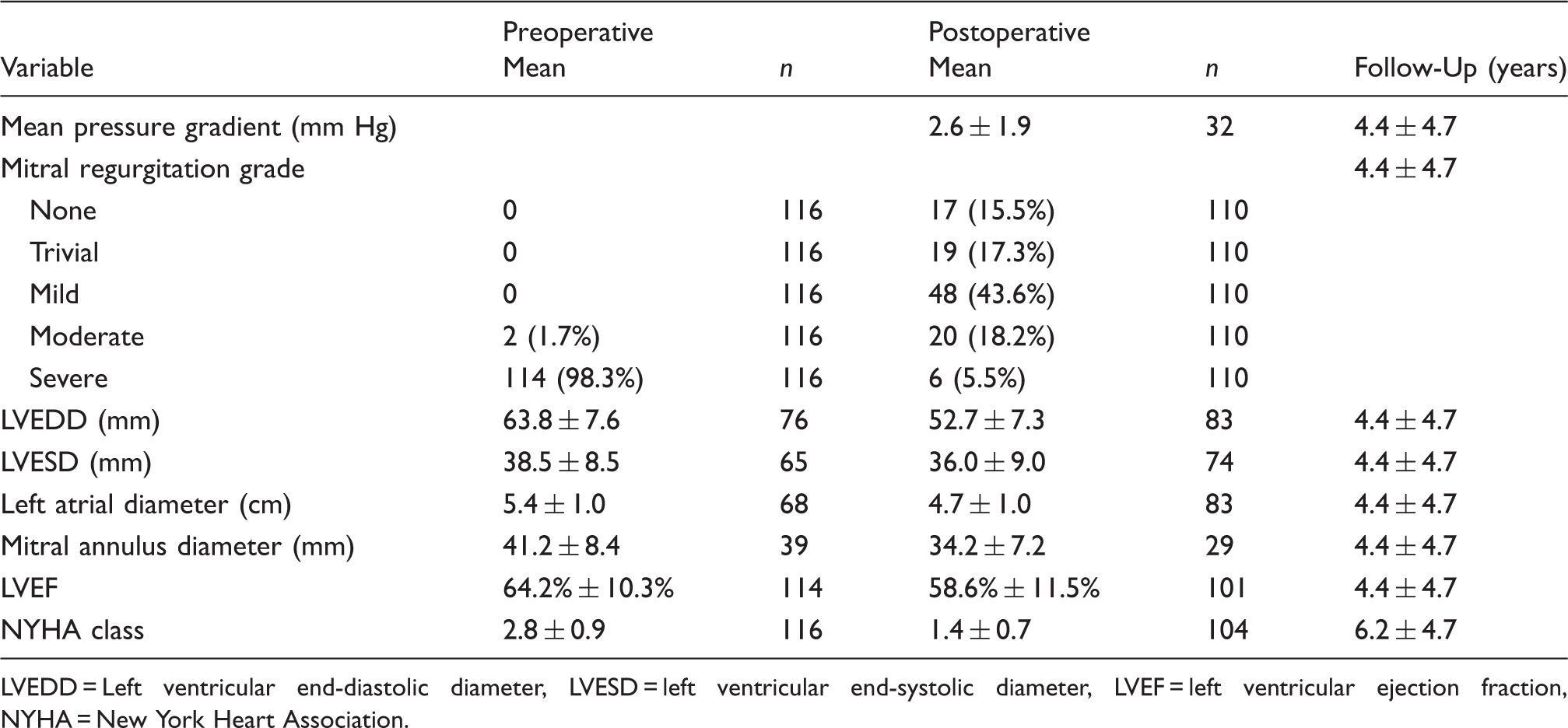
LVEDD = Left ventricular end-diastolic diameter, LVESD = left ventricular end-systolic diameter, LVEF = left ventricular ejection fraction, NYHA = New York Heart Association.
Discussion
Mitral valve repair is associated with low perioperative mortality and improved survival. 1–6 Repair with concomitant ring annuloplasty has been recommended to attenuate mechanical stress on the repair suture lines. Freedom from reoperation after repair for degenerative mitral disease incorporating annuloplasty was reported to be 93% at 10 years; 1 95% for the posterior leaflet and 90% for the anterior leaflet at 10 years (USA); 2 96% for the posterior leaflet, 88% for the anterior leaflet, and 94% for bileaflet prolapse at 12 years (Canada); 3 and 97% (posterior leaflet), 86% (anterior leaflet), and 83% (bileaflet) at 20 years (France). 4 David and colleagues 3 reported 12-year overall survival of 75%. Baumberger and colleagues 4 found 20-year actuarial survival of 48%, similar to the age-matched normal population, after non-rheumatic mitral valve repairs.
Our results agree with the previous findings. The initial recurrences of MR requiring reoperation were mainly due to limited disruption of the leaflet repair at the base. This was rectified by the subsequent technical modification, and the most recent 107 patients had a lower reoperation rate, with only one incidence of limited basal disruption of the repaired leaflet; the other cases were due to further chordal rupture. Unfortunately, routine long-term echocardiographic follow-up was constrained by resources, particularly in our early experience. However, the long-term clinical follow-up gave important criteria for assessment of this technique in a specific lesion, avoiding the cost of rings, and preventing fixation of the posterior part of the annulus. Interestingly, the actuarial survival for the most recent 107 patients was similar to the UK age- and sex-matched survival rates at 1, 5, 10, and 14 years. Although the technical modification reduced the reoperation rate, freedom from severe MR was similar in both groups. Assuming that the residual or recurrent moderate MR did not significantly improved despite the technical modification, the clinical result still suggests that this did not adversely impact on survival. This agrees with recent findings of Gillinov and colleagues 5 that patients tolerate residual MR well; they compared propensity-matched patients undergoing MV repair with and without ring annuloplasty and found similar risk-adjusted 10-year survival, despite accelerated return of MR in the latter cohort. The unadjusted 10-year survival was 84% (with annuloplasty) vs. 81% (without annuloplasty). Freedom from reoperation was not significantly different in matched groups: 97% (with annuloplasty) and 96% (without annuloplasty) at 10 years post-repair.
Some surgeons routinely omit prosthetic annuloplasty, preferring suture annuloplasty to avoid complications associated with the ring, and preserving annular flexibility. Duebener and colleagues 6 reported excellent results for repair of anterior and posterior leaflet defects, using chordal replacement with posterior suture annuloplasty: 2-year freedom from reoperation of 92.6% (anterior leaflet) and 95.0% (posterior leaflet); 2-year freedom from ≥ grade 2 MR was 94.9% (anterior leaflet) and 95.8% (posterior leaflet). David and colleagues 7 found no difference between repairs with and without ring annuloplasty in a long-term review of artificial chords for myxomatous MR repair. The mural annulus shortening suture annuloplasty technique was reported by Aybek and colleagues 8 to have satisfactory hemodynamic performance with clinical improvement at 7 years, despite progressive annular dilatation: 82.3% freedom from > trivial residual MR, 95.1% freedom from reoperation, and 87.2% actuarial survival at 77 months.
Suture annuloplasty is inexpensive and may have some advantages. A recent review found mitral suture annuloplasty to be safe, but demonstrated a trend toward recurrent annular dilatation over time. 9 Encouraging midterm clinical results were seen in degenerative MR with segmental posterior leaflet involvement and limited annular dilatation. Perioperative mortality was lower in degenerative disease using segmental plication and a semicircular reduction technique, compared to ischemic primary dilated cardiomyopathy or mixed etiology. Series using purely segmental suture plication noted 2.1%–3.5% reoperation rates, and 10%–28% residual MR > mild at follow-up of 3.1 to 5.2 years. 10–12 Alvarez and colleagues 11 reviewed 155 patients with degenerative MR and reported 7.1% moderate residual MR at discharge post-repair, a 3.5% reoperation rate (50% due to recurrent annular dilatation), and 80.4% 10-year survival. The mean transmitral gradient was lower, and the valve area was larger in patients with posterior semicircular or segmental suture annuloplasty, compared to those with a prosthetic annuloplasty ring.
Frater 13 suggested that if organic leaflet or chordal causes of MR have been corrected, the MR load removed, and the patient operated on early enough for LV function to be normal or able to return to normal after the procedure, then mechanical fixation of the annulus in the systolic dimension may not be necessary. Our series comprised 80/102 (78.4%) patients with LV dilatation on echocardiography, although the extent of dilatation was not documented. Preoperative LV end-systolic diameter available in 65 patients was 38.5 ± 8.5 mm. Only 35 patients had their mitral annulus measured preoperatively, which makes interpretation of our data on LV size difficult. However, with only 4 patients having poor LV ejection fractions (<40%), and the overall mean LV ejection fraction of 63.8% ± 10.2%, this cohort of patients were deemed to have essentially normal LV function pre-repair. The slight drop in LV ejection fraction from 63.8% to 58.6% despite other parameters showing improving trends, may be related to the relative overestimation of the preoperative ejection fraction, due to a large volume of ejection retrograde into the left atrium. We were unable to draw any further conclusions because ejection fraction was assessed at variable times after surgery. We did not experience clinically significant kinking of the circumflex artery with myocardial ischemia in the postoperative period. The mean duration of MR pre-repair was 3.0 ± 3.6 years (range, 0–18 years). For patients referred early for surgical repair, including asymptomatic cases, local suture annuloplasty may be an acceptable alternative for repair of type II posterior mitral leaflet prolapse.
We acknowledge the various limitations inherent in a retrospective study. This was a selected subset of patients undergoing mitral valve repair. Specifically, our database does not allow identification of the various types of mitral valve repair; a manual search of the operating room logbooks was performed to identify mitral repairs without an annuloplasty ring. This was subsequently verified by examination of the patients’ notes. We chose to study the clinical result of this uncommon and controversial technique because survival is the most robust data that can be collected in a retrospective study. Intraoperative transesophageal echocardiography was not routinely performed in the early years, and variables measured on echocardiography were not standardized. This is reflected in the significant data attrition when attempting to compare preoperative and postoperative objective variables. A significant number of these patients were elderly and preferred not to make a long journey back for follow-up echocardiography. However, this study showed that MR severity and NYHA status improved postoperatively, with significant reductions in LV and left atrial dimensions. Mean pressure gradient was acceptable post-repair, and progressive annular dilatation was not seen in the limited number of patients with annular dimensions measured at follow-up. Survival was similar to that of the age- and sex-matched UK population. We found that with the technical modification, the reoperation rate reduced, and although the rate of residual or recurrent severe MR remained significant, the long-term survival post-modification was not adversely affected. This technique may be relevant for older patients with normal LV function operated on early via minimally invasive approaches.
Footnotes
Acknowledgment
We would like to thank Dr Harald Becher, Dr Amina Khalil, and Ms Samantha Pearce for their assistance.
Presented at the Australasian Society of Cardiac and Thoracic Surgeons 2009 Annual Scientific Meeting, Noosa, Queensland, Australia, November 5–8, 2009.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.