
Abstract
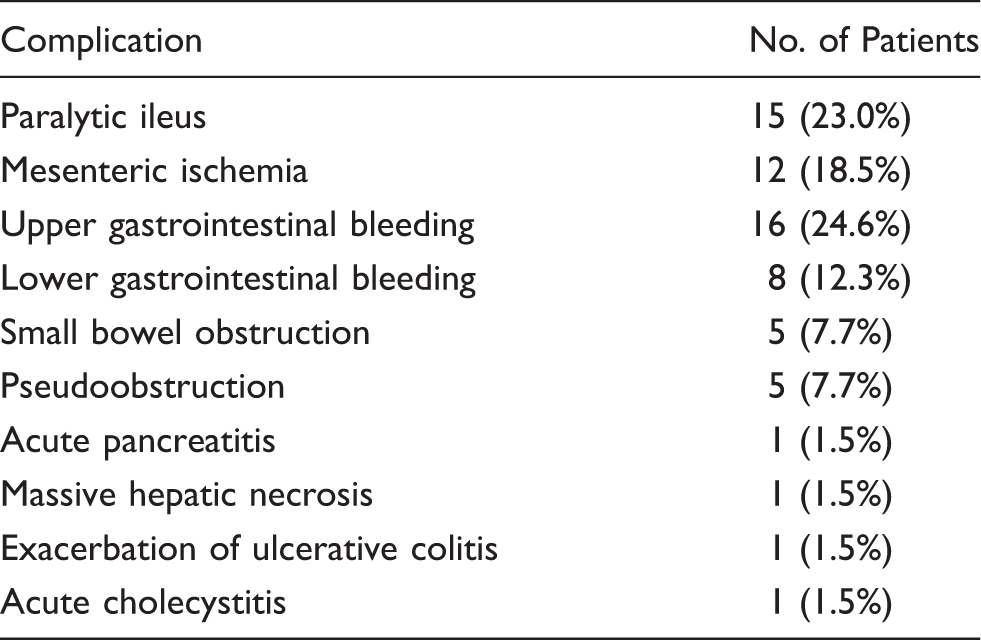
Between April 2001 and December 2005, data were collected prospectively from 2,320 consecutive patients who underwent first-time coronary artery bypass. Logistic multiple regression analyses were carried out to determine the independent predictors of gastrointestinal complications and death. There were 65 major gastrointestinal complications identified in 65 (2.8%) patients: paralytic ileus in 15, mesenteric ischemia in 12, upper gastrointestinal hemorrhage in 16, lower gastrointestinal hemorrhage in 8, small bowel obstruction in 5, pseudoobstruction in 5, and others in 4. The 30-day mortality was 21.5% (14 patients). Female sex, preoperative creatinine >200 µmol·L−1, previous gastrointestinal pathology, low cardiac output, readmission to the intensive care unit, postoperative pulmonary complications, arrhythmias, hemofiltration, and reoperation were independent predictors of major gastrointestinal complications. Independent risk factors for death were readmission to the intensive care unit, the need for hemofiltration, reoperation, and ischemic bowel. Careful hemodynamic control and optimization of perioperative organ perfusion are important to minimize the mortality associated with major gastrointestinal complications after coronary artery bypass.
Keywords
Introduction
Gastrointestinal (GI) complications are difficult to diagnose early after coronary artery bypass grafting (CABG) because symptoms may not be evident due to sedation, mechanical ventilation with or without muscle paralysis, and analgesia. The ability to identify patients who are at greater risk of developing GI complications may allow earlier detection and treatment, thereby increasing the probability of a successful outcome. These complications are rare (0.4%–2%), but result in high mortality. 1 Although many retrospective reviews have reported various GI complications after CABG, including GI bleeding, mesenteric ischemia, pancreatitis, cholecystitis, perforated ulcers, and ileus, very few studies have assessed the risk factors for developing GI complications and the associated mortality, using multivariate analysis in the same series of patients. 2 We aimed to determine the risk factors for developing GI complications and the associated mortality in patients undergoing first-time CABG.
Patients and methods
Between April 2001 and December 2005, data were collected prospectively from 2,320 consecutive patients who underwent first-time CABG at our tertiary referral center. Collating of the data commenced in January 2006, and progressed up to August 2006, mainly to determine the survival data. Information for the study was obtained from our cardiac surgical Patients Analysis and Tracking System database and hospital records. Patients who had a myocardial infarction within 4 weeks, those requiring concomitant valve or other surgery, and patients on inotropic infusions or in shock preoperatively were excluded from the study. Stepwise logistic multiple regression analyses were carried out to determine the independent predictors of GI complications and subsequent death. Two analyses were performed: the patients with GI complications were compared with those without GI complications; and the predictors of survival were determined in 51 patients who survived and 14 who died after GI complications. The definitions of GI complications were derived from the Society of Thoracic Surgeons’ database. 3 Upper and lower GI bleeding were determined on the basis of endoscopy findings.
Descriptive statistics were obtained using the SPSS software package version 15 for Windows (SPSS, Inc., Chicago, IL, USA). To generate the unadjusted risk of each factor, continuous variables were compared between groups using the Student t test, and categorical data were compared using Fisher’s exact test and the chi-squared test. To determine the influence of various factors on the incidence of GI complications and subsequent mortality, patient variables that might influence outcome were analyzed using automated forward multiple regression analysis. A value of p < 0.05 was considered significant in all statistical analyses.
Results
Gastrointestinal complications after first-time coronary artery bypass in 65 patients
Preoperative characteristics of patients with and without GI complications
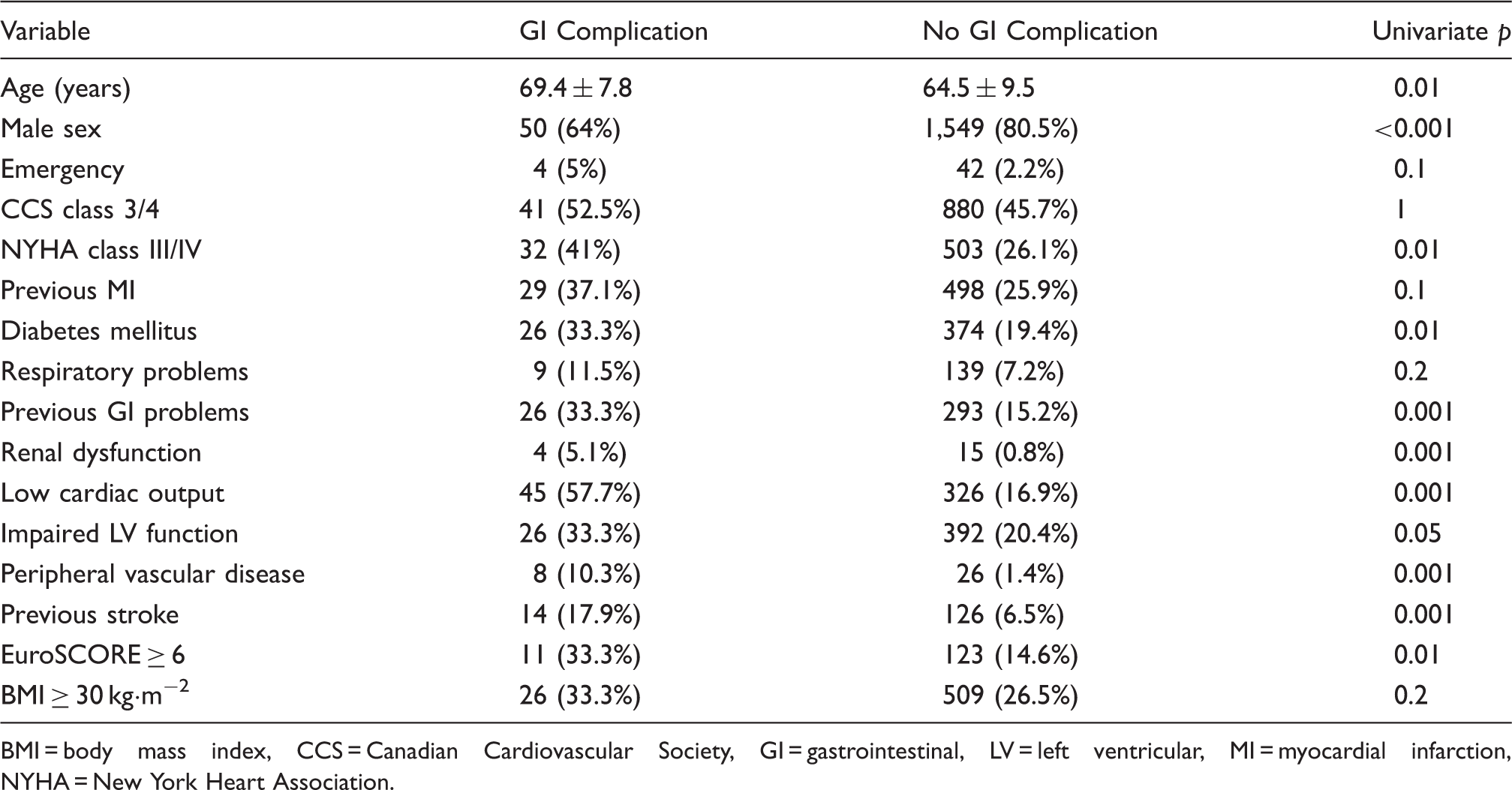
BMI = body mass index, CCS = Canadian Cardiovascular Society, GI = gastrointestinal, LV = left ventricular, MI = myocardial infarction, NYHA = New York Heart Association.
Postoperative characteristics of patients with and without GI complications
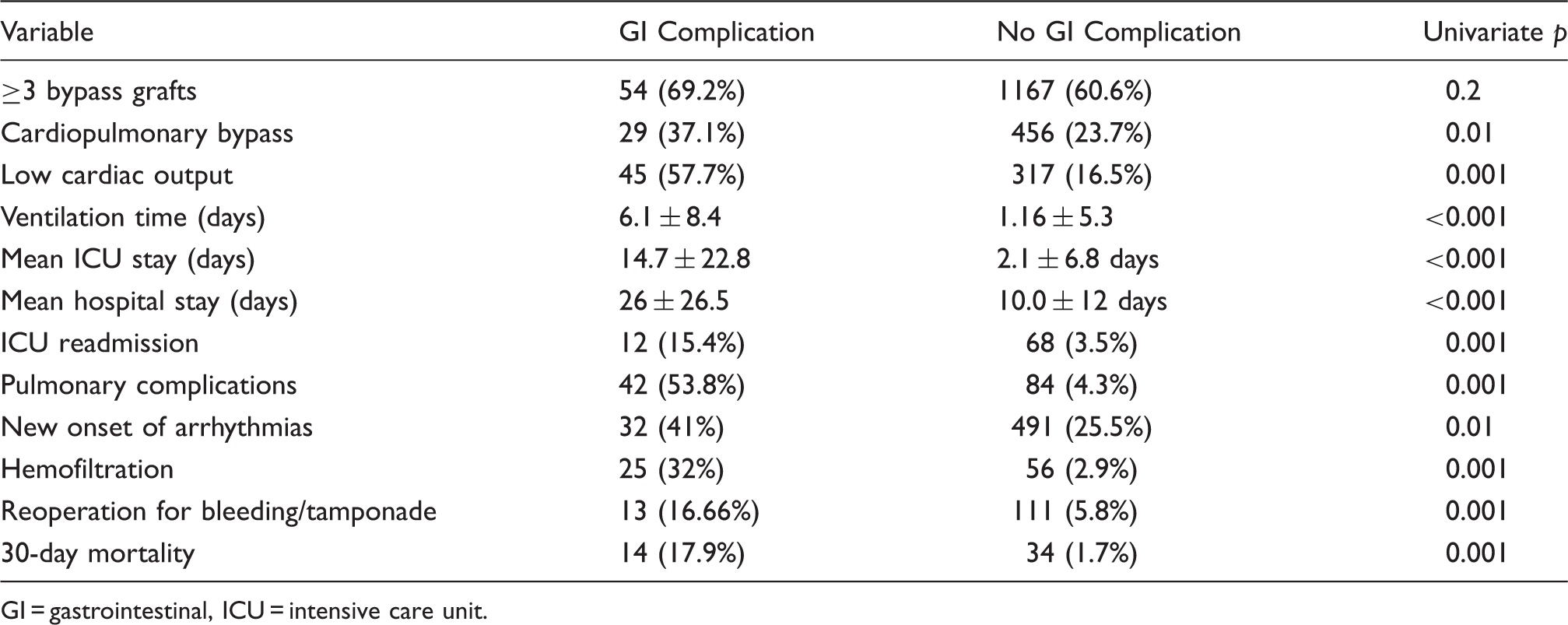
GI = gastrointestinal, ICU = intensive care unit.
Multivariate analysis of predictors of GI complications
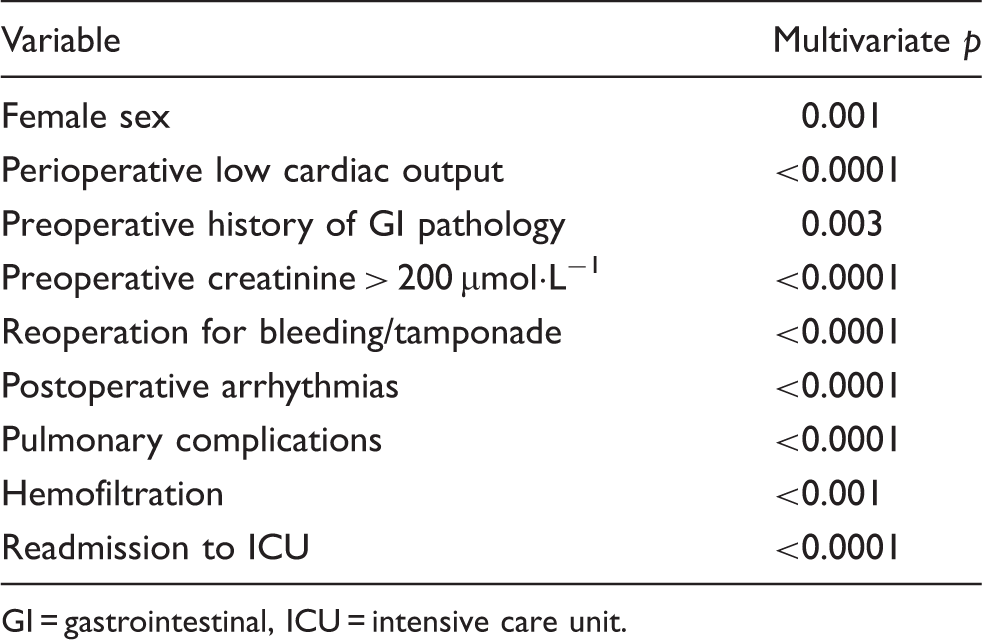
GI = gastrointestinal, ICU = intensive care unit.
Variables affecting mortality in patients with GI complications
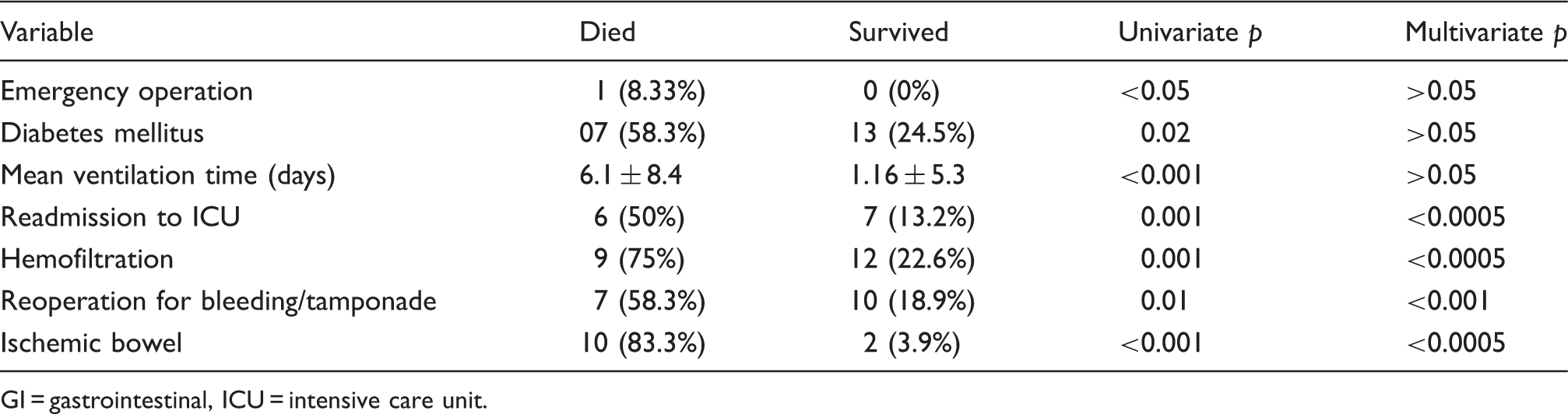
GI = gastrointestinal, ICU = intensive care unit.
Discussion
Previous studies have demonstrated that advanced age (≥65 years), history of ulcer, low cardiac output syndrome, prolonged mechanical ventilation, and reexploration for hemorrhage are risk factors for GI complications after cardiac surgery. 4,5 The literature on this subject emphasizes the interplay of multiple factors leading to splanchnic hypoperfusion and consequent GI complications after CABG. 2 Published mortality rates vary from 11% to 59%. 1–4,6 The 2.8% incidence of GI complications and 21.5% mortality rate in our series are consistent with those of previous reports. All patients were routinely started on proton-pump inhibitors postoperatively; those who were already taking antacids, H2 blockers, or proton pump inhibitors had their medication continued up to the day of surgery.
The need for postoperative hemofiltration increases the incidence of GI complications after CABG. Acute renal failure after cardiac surgery is associated with high morbidity and mortality rates, and results from organ hypoperfusion during CPB and in the postoperative phase. 7 Moderate renal failure in animals alters duodenal-jejunal motility, decreases colonic transit time, and may contribute to GI injury. 8 A direct relationship between acute renal failure and GI complications after cardiac surgery has previously been determined by multivariate analyses. 2,7,9 History of GI disease increases the likelihood of GI complications after CABG. 2 Specifically, history of peptic ulcer is an independent risk factor. GI bleeding usually results from stress ulceration and is more common in the elderly and those with preexisting ulcer disease. Previous GI pathology was present in 26 of our patients (peptic ulcer, cholecystitis, pancreatitis, and previous laparotomy). Separately, each of these diagnoses was not significant, but when grouped together, they became significant. Patients with universal arteriosclerosis are at higher risk of mesenteric ischemia postoperatively. None of our patients had preoperative symptoms suggestive of mesenteric ischemia, such as abdominal angina.
Any suspicion of a GI complication was addressed by a GI surgeon or gastroenterologist. Paralytic ileus was diagnosed by a consultant general surgeon on the basis of clinical features (painless abdominal distension) and grossly distended bowel loops on plain abdominal radiographs. This is clearly different from the normal more or less paralytic condition of the bowel postoperatively. Several patients suffered small bowel obstruction or pseudoobstruction. The cause of bowel obstruction or pseudoobstruction was previous laparotomy resulting in subacute obstruction due to adhesions. Once a complication was identified, a specialist referral was made immediately, and appropriate measures were taken. For upper and lower GI bleeding, both esophagogastroduodenoscopy and colonoscopy were performed. Sclerotherapy ± adrenaline injection was carried out in appropriate cases. No patient required a laparotomy for GI bleeding. In suspected ischemic bowel, the on-call general surgeon reviewed the patient, and if felt appropriate, a laparotomy was performed. Paralytic ileus was treated conservatively.
It is important to identify patients at increased risk of GI complications, but it is equally important to examine the outcomes of those who suffer such complications. There was a significant correlation between GI complications and postoperative cardiac rhythm, pulmonary, and renal complications. The factors associated with increased mortality after GI complications in our series were readmission to the ICU, need for hemofiltration, reoperation, and ischemic bowel. GI complications are among the causes of ICU readmission after cardiac surgery. 10 We found that readmission to the ICU was associated with increased mortality in patients with GI complications after CABG. However, it is difficult to establish the cause-effect association between different complications after CABG. It is worth noting that these patients frequently have multiple complications. Significant associations between GI complications and the length of ICU stay, hospitalization, and the period of mechanical ventilation were found in our study and that of Recht and colleagues. 9 This has important economic implications in these times of over-stretched health resources and the risk of acquiring nosocomial infections.
Prolonged CPB time has been suggested as a risk factor for the development of GI complications. 5,11,12 Off-pump CABG has been reported to reduce the inflammatory response after conventional CABG. 13 Based on this argument, there is a belief that off-pump CABG can reduce end-organ damage, but the BHACAS study, the Octopus group study, and another recent study from Canada did not reveal any difference between the 2 approaches in terms of GI complications. 14–16 In our study, CPB was not found to be a significant risk factor for GI complications; 37% of patients with GI complications and 23.7% of those without GI complications underwent CABG with CPB. Multivariate analysis did not identify CPB as a significant factor. Hospital mortality among those who developed GI complications was also similar for the 2 surgical approaches. This study was unable to address the difference in pathogenesis of GI complications between conventional and off-pump CABG. However, a study of markers of gut injury (gastric intramucosal pH, tumor necrosis factor-α, interleukin-6, endotoxin) may identify factors involved in gut damage during and after CABG with and without CPB. This may improve our overall understanding of gut physiology during CABG.
Although the pathogenesis of GI complications after CABG is complex, the key factor implicated is reduced systemic blood flow with end-organ hypoperfusion, leading to anaerobic metabolism at the cellular level. 17 The reasons for the increased susceptibility to hypoxia of the GI tract include its inability to autoregulate during periods of hypotension or persistent vasoconstriction during normotension. This is why low ejection fraction, peripheral vascular disease, and postoperative arrhythmias (noted in our study) predispose to mesenteric ischemia. 6 Furthermore, low cardiac output requiring inotropic or balloon pump support is a predictor of mesenteric ischemia. The pathogenesis of ischemic and bleeding complications is different, and also of upper and lower GI bleeding, but the low incidence of GI hemorrhage in our series means that a much larger study is needed for a meaningful analysis.
This report included only patients who underwent CABG since 2001, with a relatively large sample size from a center with a complex case mix, but it was not randomized. On the basis of this study and previous reports, patients with identified risk factors should be alerted to the possibility of GI complications and the associated mortality, to ensure that informed consent has been obtained. Specific clinical measures tailored to individual patients at risk of developing GI complications should be implemented to optimize their hemodynamic status. The implementation of improved risk stratification with risk models, and the application of goal-directed hemodynamic therapy should be considered. 18,19 The early opinion of a GI surgeon regarding early intervention should be sought. A diagnostic laparoscopy for quick inspection carries less morbidity than an exploratory laparotomy. GI complications after CABG may occur at a higher rate than previously described. 20 With CABG being performed in older and sicker patients, a higher level of vigilance is mandatory to ensure swift referral of suspected cases to specialists for early diagnosis and rapid treatment of GI complications.
Footnotes
Acknowledgments
We would like to thank Michael Roughton, statistician at the Royal Brompton Hospital, London, and Joy Spanner who maintains the Patients Analysis and Tracking System database.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.