
Abstract
Long-term survival has become achievable after bone-marrow transplantation, but various pulmonary diseases due to chronic graft-vs.-host disease have been recognized. Particularly, bronchiolitis obliterans is a life-threatening complication with no effective remedy. Bilateral pneumothorax associated with bronchiolitis obliterans is rare, but it requires careful attention. In a 42-year old man with intractable pneumothorax after bone marrow transplantation and surgical procedures, extensive thoracolysis was effective as an acute treatment for this disease.
Introduction
Recently, long-term survival has become achievable for many patients undergoing hematopoietic stem cell transplantation (HSCT). However, pulmonary complications develop in 40%–60% of recipients, which can become life-threatening and account for 10%–40% of transplant-related deaths. 1,2 Bronchiolitis obliterans (BO) and idiopathic pneumonia have been frequently reported as important respiratory complications. Air-leak syndromes, including pneumothorax, pneumomediastinum, pulmonary interstitial emphysema, and subcutaneous emphysema, are rare complications in HSCT recipients with chronic BO related to graft-vs.-host disease. 3 Pneumothorax requires special attention because it can lead to sudden death if it occurs coincidentally in both lungs, but due to its rarity, no standard treatment has been established.
Case Report
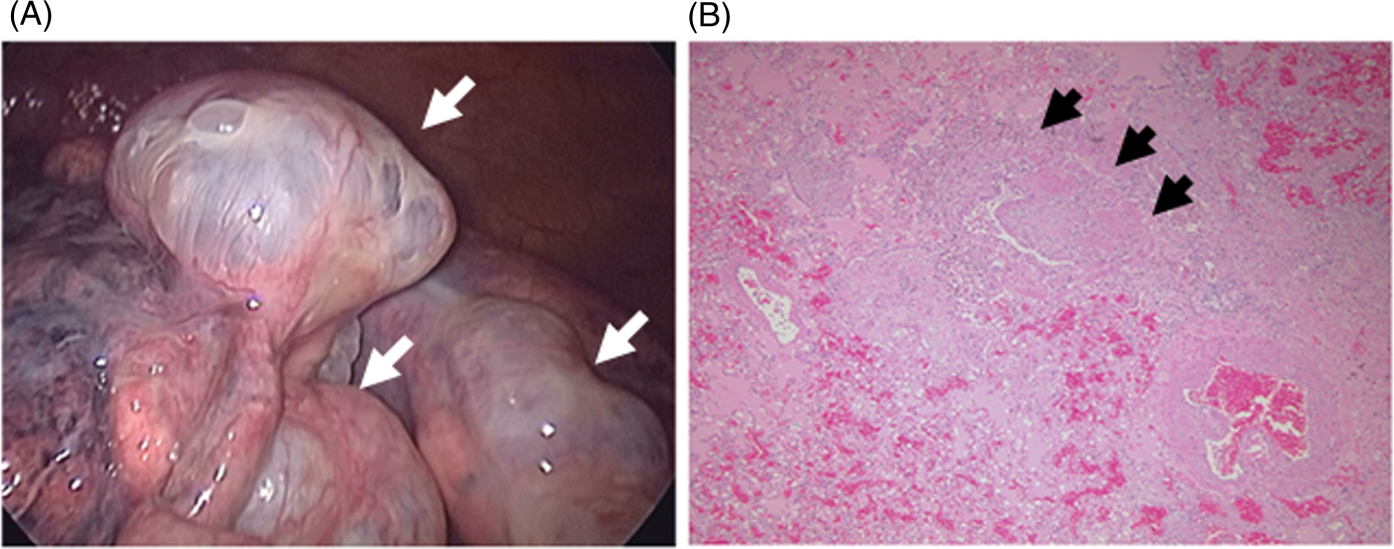
A 42-year-old man with recurrent pneumothorax was hospitalized with dyspnea and chest pain. He was a nonsmoker with no other history of lung disease (Figure 1A). Five years earlier, he had been diagnosed with acute myeloid leukemia and underwent HSCT from his compatible sister. Two years later, pneumothorax recurred and partial lung resection by thoracoscopy was performed once on the left side and twice on the right side. Bullous changes progressed in both lungs after each operation. In these operations, the only partial resection and reinforcement with a polyglycolic acid sheet was undertaken because the diagnosis at this time was spontaneous pneumothorax. The latest chest computed tomography showed exacerbation of the lung lesion, with bullous change on the pleura and patchy areas of increased attenuation (Figure 1B). Chest radiography on admission demonstrated a left-sided tension pneumothorax. Arterial blood gas analysis revealed hypercapnia (PaCO2 74.8 Torr) and hypoxemia (PaO2 62.7 Torr). Intercostal tube drainage was performed immediately. After 9 days of persistent air leakage, partial lung resection with thoracoscopy was carried out, and the ruptured bulla located on the left S3 was resected. In addition, there were multiple bullae at various sites (Figure 2A). A progressive disease accompanied by chronic graft-vs.-host disease was suspected on the basis of his clinical course and the bullae existing in an extremely wide sphere, so complete resection was very difficult. In addition, neogenesis of bullae after the operation was anticipated. Therefore, after resection of the culprit lesion, we reinforced the entire lung apex, including the staple line, with a polyglycolic acid sheet and fibrin glue, and performed extensive thoracolysis of the chest wall. Histologically, a patchy distribution of plugs of granulation tissue filled the lumen of the distal airways, and there were no leukemic cells (Figure 2B). These findings were compatible with HSCT-related BO. Ten days after the operation, the patient complained of abdominal discomfort without dyspnea and chest pain. Chest radiography showed a left-sided pneumothorax that was exclusively over the diaphragm (Figure 1C), and a 12 F chest drain was inserted. After 7 days of persistent air leakage, pleurodesis was attempted using autologous blood, and tetracycline was instilled via the chest drain. Despite these treatments, subtle minor air leaks persisted, thus reoperation was performed via thoracoscopy. Extensive pleural adhesion to the chest wall was apparent, except for the mediastinal side and the diaphragm, but there was no obvious air leak site, even with a water seal test at 20 cm H2O. The instilled blood coagulated on the dorsal side and did not appear to achieve pleural adhesion. Further thoracolysis on the mediastinal side and diaphragm was performed to achieve the larger pleural adhesion. At 4 days postoperatively, the patient remained stable and symptom-free (Figure 1D), so the chest drain was removed and he was discharged the following day. Immunosuppression therapy was started. The lung lesion has been stable for the past year.
(A) Chest computed tomography before stem cell transplantation, showing no lesion in either lung field, and (B) on admission when the left lung had completely collapsed and the heart was pushed to the right side. (C) Chest radiograph 10 days after the operation, indicating that the left pneumothorax had relapsed but it was localized over the diaphragm. (D) Chest radiograph on discharge, showing the left pneumothorax had improved. (A) Intraoperatively there were many bullae occurring in various places (arrows). (B) Pathology revealed that a fibrous tissue mass reduced the lumen of the bronchiole to a slitlike space (arrows). Hematoxylin and eosin stain, original magnification ×40.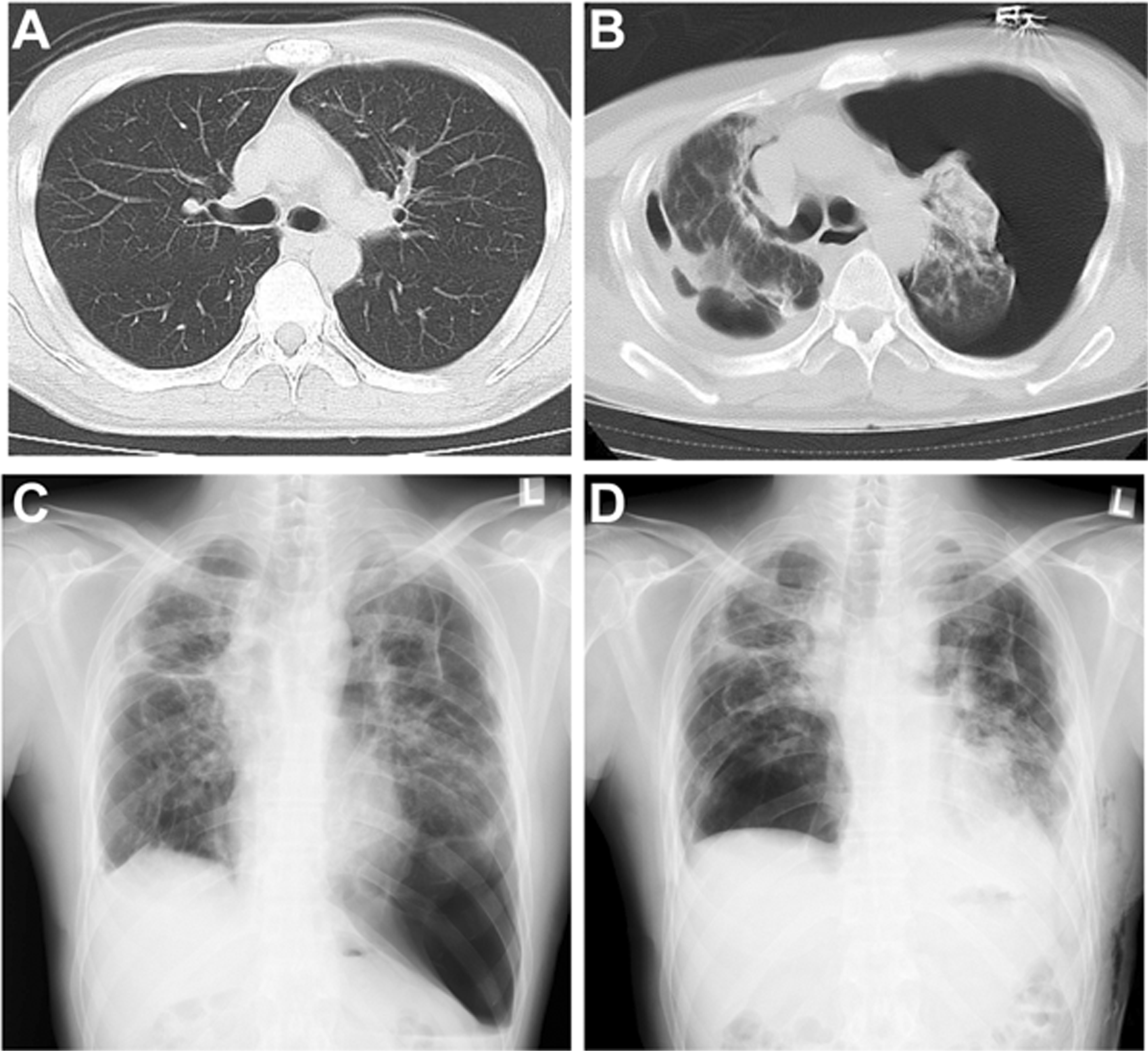
Discussion
No prospective clinical trial has addressed the management of BO. Based on anecdotal reports, corticosteroids and augmented immunosuppression can be used for treatment, but only a minority of patients improve. 4,5 The reported incidence of BO is 1.7%–8.3%, and the median time to onset is 431 days after HSCT. 1,4 The factors associated with increased risk of BO are peripheral blood-derived stem cells and a sex match of female donor to male recipient. 1 On the other hand, bilateral pneumothorax after HSCT is a much rarer complication, with only 8 reported cases to date. 2,6,7 One possible mechanism of production of multiple bullae in BO was suggested to be the check-valve mechanism, secondary to obliterated bronchioles, leading to neogenesis of multiple bullae and recurrent pneumothorax. 3 There is no definitive treatment for pneumothorax-related BO. In rare cases, lung transplantation can be attempted, but even after transplantation for other lung diseases, BO eventually develops in 50% of recipients. 1
In this case, the patient developed acute respiratory failure from tension pneumothorax. Given the lack of a definitive treatment for this bothersome disease, our goal in this case was to prevent sudden death and dyspnea due to bilateral pneumothorax. Pleurodesis with blood or tetracycline was unsuccessful, but extensive thoracolysis proved satisfactory. Talc is recommended for intractable pneumothorax, but it infrequently causes acute respiratory distress syndrome, and to our knowledge, there has been no report of the use of talc in bilateral pneumothorax due to HSCT-related BO. 8 Moreover, talc is not approved in Japan for injection into the chest cavity. Repeat surgery has the potential to exacerbate the lung lesion, because the application of positive-pressure ventilation could cause new bulla formation in the opposite lung via the check-valve mechanism of BO. It is important to diagnose BO at an early stage, and extensive thoracolysis to obtain pleural adhesion should be considered to prevent pneumothorax before the lung lesion progresses.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.