
Abstract
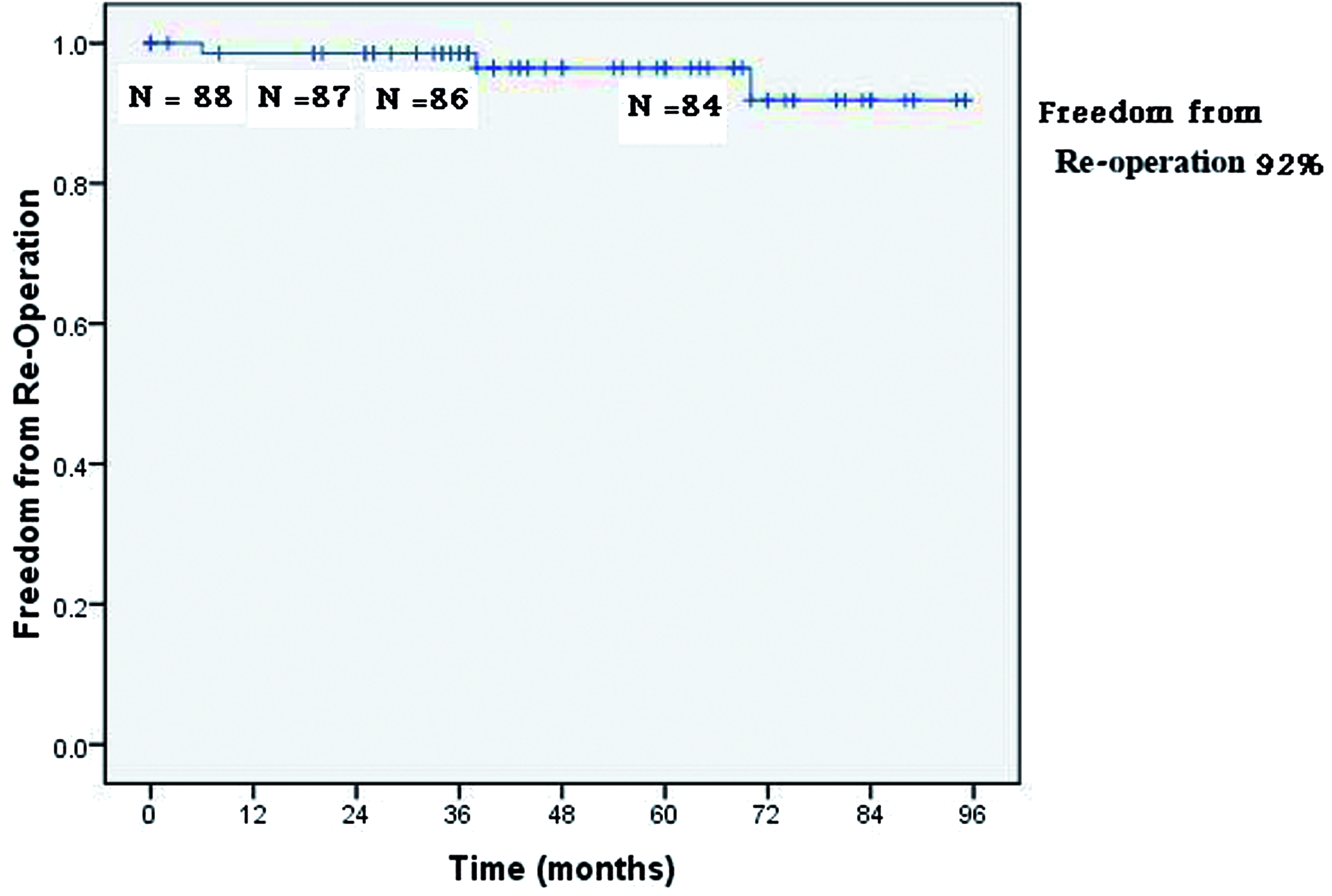
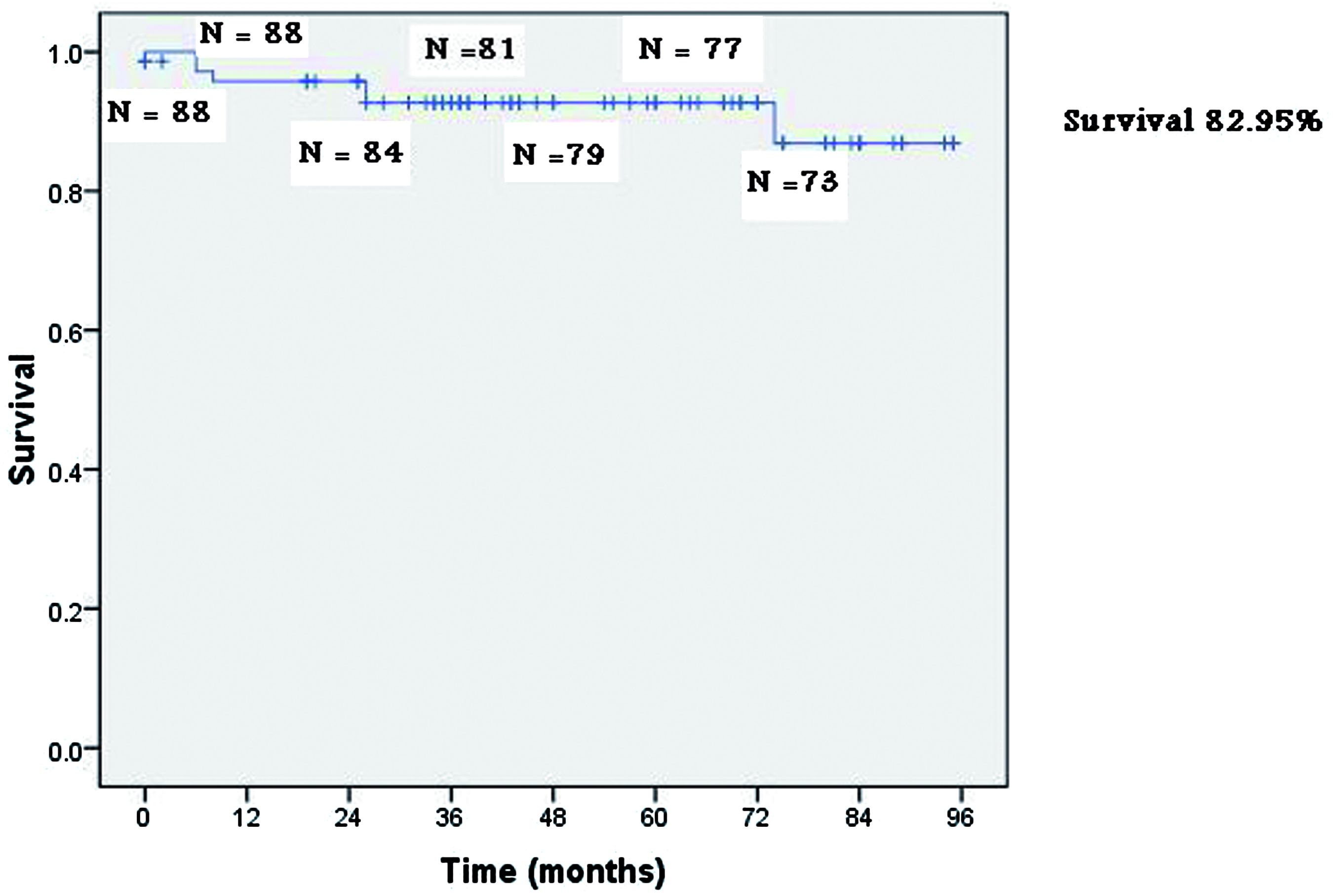
Between July 1997 and August 2004, 92 patients with irreparable mitral valves underwent replacement with a pulmonary autograft. This report brings the follow-up data of these patients up to date. Eighty-eight patients had a successful Ross II operation; 4 were lost to follow-up. The mean follow-up period was 94 months. Transesophageal echocardiography revealed a successful outcome in all 88 patients immediately after the operation. Operative mortality was 4.6%, and late mortality definitely related to the operation was 12.5%. At a mean follow-up of 94 months, freedom from structural valve deterioration (significant mitral stenosis and/or regurgitation) was 93.4%, freedom from reoperation was 92.0%, and freedom from all causes of death was 82.9%. Two autografts were explanted because of endocarditis. Two patients developed significant pulmonary stenosis, one of whom underwent operative repair. These data compare favorably with those of mitral valve replacement using modern bioprostheses. This procedure remains an option for the relatively young patient when life-long anticoagulation is contraindicated or impractical. It is also an option to consider in infants with complex irreparable mitral valve disease.
Keywords
Introduction
We have been involved in reviving the Ross concept of replacing irreparable mitral valves (MV) with pulmonary autografts since 1997. 1 – 7 We postulated that the pulmonary autograft would prove to be superior to standard mechanical prostheses, because life-long anticoagulation is impractical in our region, and that it would be more durable than stented bioprostheses in our relatively young patients, because it is autogenous tissue. 8 Our last analysis of the first 92 patients who underwent this operation covered a mean follow-up period of 60.0 months. 7 This report carries the analysis further to a mean follow-up of 93.9 months.
Patients and Methods
Four patients required repeat MV replacement after the initial operation due to inadvertent stenosis of the Dacron conduit used to stabilize the pulmonary autograft when we changed the old-fashioned Dacron tubings to the new pretreated soft variety. 3,7 Of the remaining 88 patients, 62 were female, and the mean age was 39.2 ± 11.2 years. All patients had rheumatic MV disease, except 2 whose mitral pathology was congenital. The profile of the 88 patients who were successfully operated on as well as exclusion criteria were reported previously. 7
The operative technique evolved through a number of stages, and has been described in full in previous reports.
5,7
Briefly, when it is decided that the MV cannot be repaired, our current technique entails excising a flap of pericardium, taking down the pulmonary artery, and suturing a proper sized homograft or xenograft in its place. Our preference is to use a pulmonary homograft whenever possible. When this is not available, we use alternative substitutes. In this series, we used 29 pulmonary homografts, 56 pulmonary xenografts, and 3 aortic homografts. Meanwhile, the co-surgeon cuts off a 1-inch section of Dacron tubing, slightly larger than the estimated size of the autograft (usually 30 mm), marks it with 6 equidistant longitudinal lines, and wraps the pericardial sleeve around it after placing approximately 2 ml of surgical glue (BioGlue; Cryolife, Inc., Kennesaw, GA, USA) between the pericardium and Dacron cloth (Figure 1). The pulmonary autograft is placed inside the Dacron or pericardial tubing, and the proximal and distal ends are sutured to those of the tubing, aided by the pre-marked lines for orientation (Figures 2 and 3). The pulmonary sinuses, in contrast to aortic sinuses, are symmetrical, therefore, care is taken to distribute them symmetrically inside the Dacron tubing. Finally, the surgeon secures the distal (pulmonary commissural) end of the conduit to the mitral annulus. Intraoperative transesophageal echocardiography is carried out before decannulation to ensure that the results are acceptable.
Actuarial curve of freedom from structural valve deterioration. Actuarial curve of freedom from reoperation. Actuarial curve of freedom from death from all causes.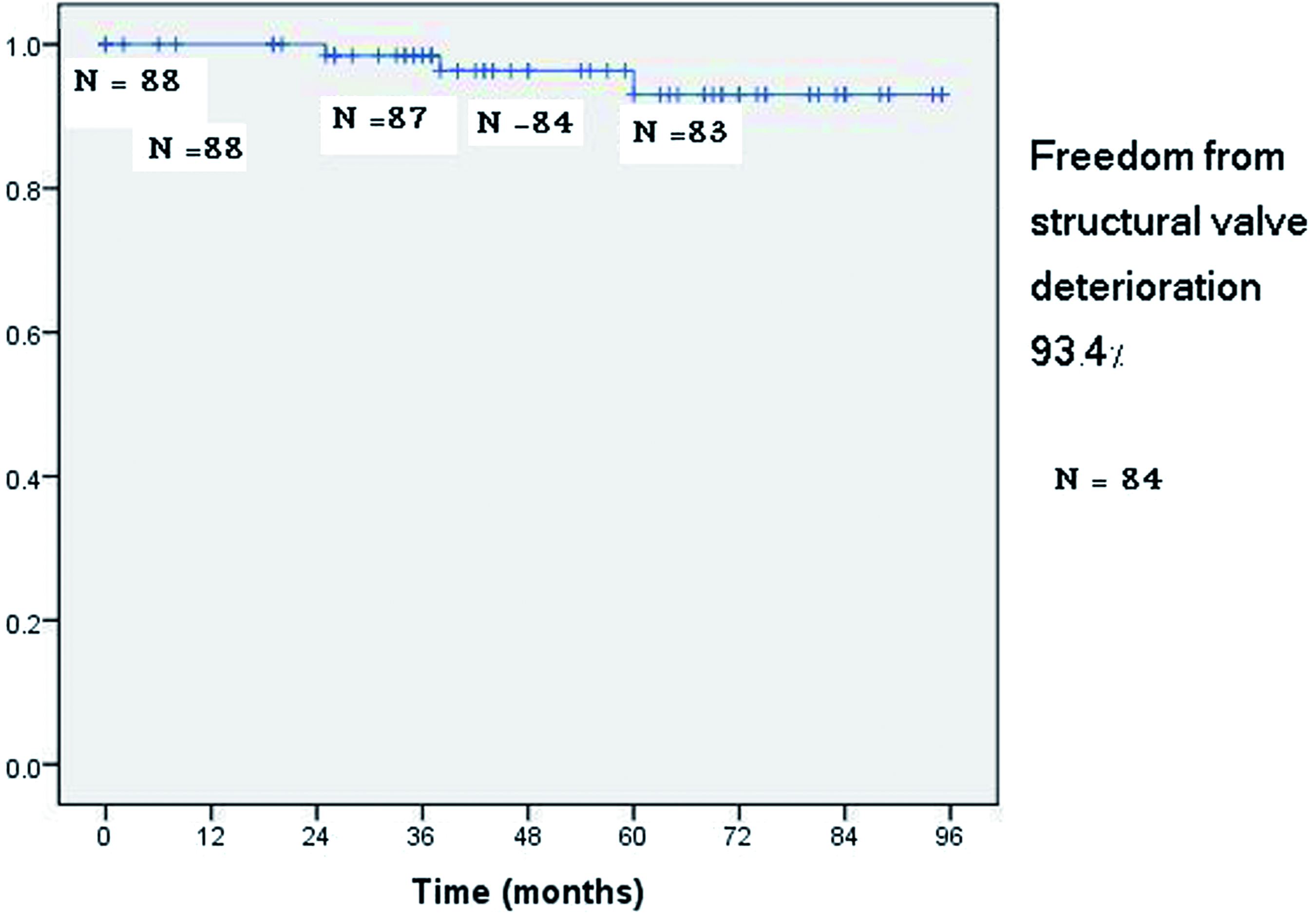
Follow-up with clinical examination and echocardiography, initially scheduled at 1, 3, and 6 months after the operation, was continued on a yearly basis thereafter. When it was impossible to get first-hand information, we relied on reports from the patient’s local physician. Anticoagulation was discontinued 3 months after the procedure in patients in sinus rhythm. Those who remained in atrial fibrillation were continued on anticoagulants to maintain an international normalized ratio of 2–2.5. Three patients in atrial fibrillation could not be anticoagulated and were placed on antiplatelet therapy. Penicillin prophylaxis was prescribed for life in all patients. 7
Statistical analyses were performed using Statistical Package for the Social Sciences, version 17 software (SPSS Inc, Chicago, IL, USA). Actuarial curves were constructed using the Kaplan-Meier method. Autograft structural valve deterioration was defined as MV area < 1.5 cm2 and/or regurgitation > grade 1.5/4 (1.5 = mild regurgitation). Mitral regurgitation was estimated by jet size and mental 3-dimenstional jet reconstruction.
Results
Outcome of mitral valve replacement with a pulmonary autograft in 92 patients
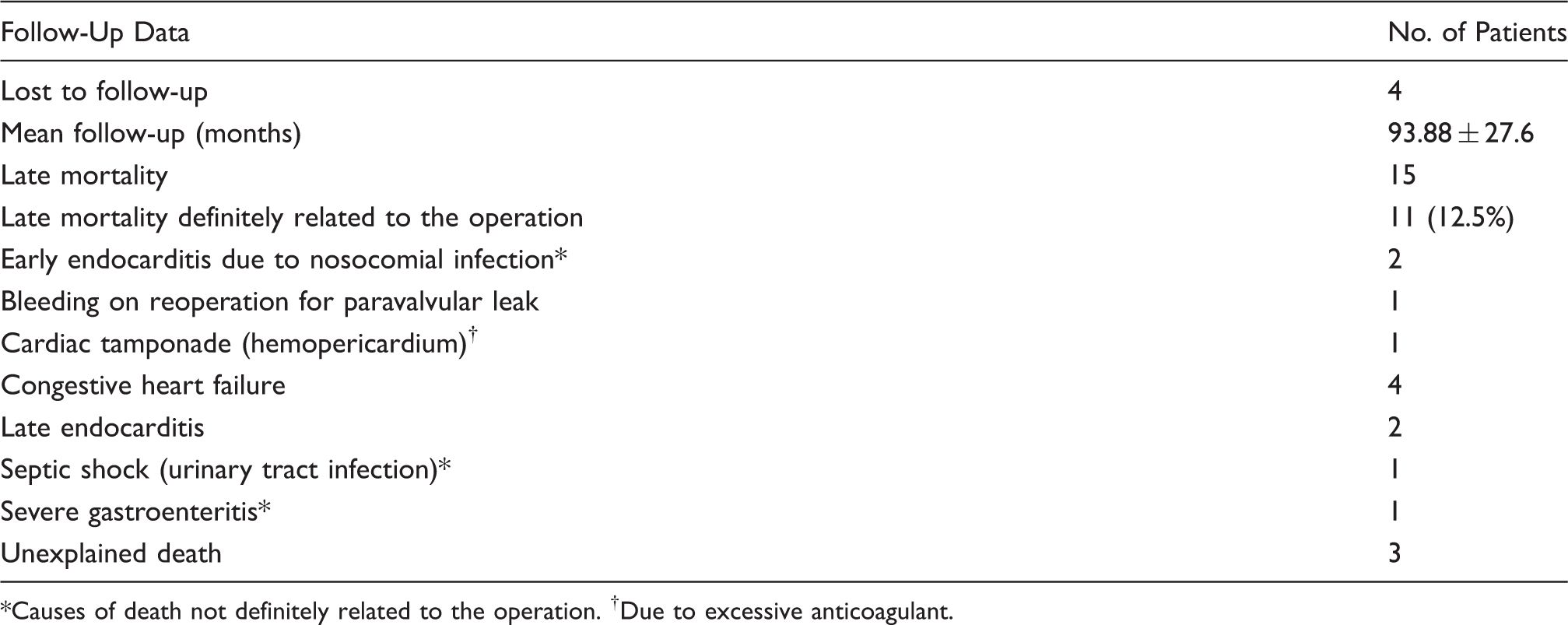
Causes of death not definitely related to the operation. †Due to excessive anticoagulant.
Discussion
Rheumatic heart disease is still endemic in most developing countries, propagated by persistent poverty and over-crowding. 9 The mitral valve is the chief victim of rheumatic carditis, and when it cannot be repaired, it is usually replaced with a mechanical prosthesis. Limited economic means and poor standards of health education, combine to make life-long anticoagulation, mandated by mechanical prostheses, inapplicable in developing countries. 8 An ideal tissue MV substitute for the relatively young rheumatic patient has so far eluded cardiac surgeons and biomedical engineers. 10 Mitral homografts, although offering perfect hemodynamics, have proved to be of limited durability, and the quadrileaflet bovine valve never became commercially available. 11,12 Stented bioprostheses, which might be the best available alternative for elderly patients, are not suitable for the young, even in their newer generations. 13
At Damascus University, we have preformed the Ross II operation since 1997. We hoped that our results would match those of the classic Ross procedure for the aortic valve, especially as some patients from the earliest small Ross II series survived for 11–14 years with their mitral autografts before being lost to follow-up. 14,15 Initially, we used the “top-hat” configuration described by Yacoub and Kittle 16 for implanting aortic homografts in the mitral position, to construct the autograft/Dacron conduit. Because securing the pericardial collar to the left atrial wall prolonged an already long operation, and required going back on cardiopulmonary bypass to repair a flail pericardial segment in a few patients, we changed after the first 36 cases to using pericardium only to wrap the Dacron tubing. After 10 patients, we abandoned the use of pericardium altogether to simplify the operation even further. When it was obvious that a definitive solution had to be found to prevent kinking of the soft varieties of pre-treated Dacron (which are the only types of Dacron presently available), we returned to wrapping the Dacron tubing with pericardium, but this time after inserting surgical glue between the pericardium and Dacron material to give the conduit the resilience needed to prevent bending in diastole. Surprisingly, we have had no problems with sizing, even when there was some discrepancy between the constructed conduit and mitral annulus. The autograft, which is circular, seems to function well when secured to the oval-shaped mitral annulus, and provides acceptable hemodynamics. To our knowledge, the physiology of semilunar valves of aortic homografts and pulmonary autografts on the in-flow side of the left heart has not been studied so far, neither have the stresses to which their cusps are exposed; this may be an interesting subject for a future investigation.
Our last report revealed good medium-term performance of the pulmonary autograft in the mitral position after 60.0 months of follow-up.
7
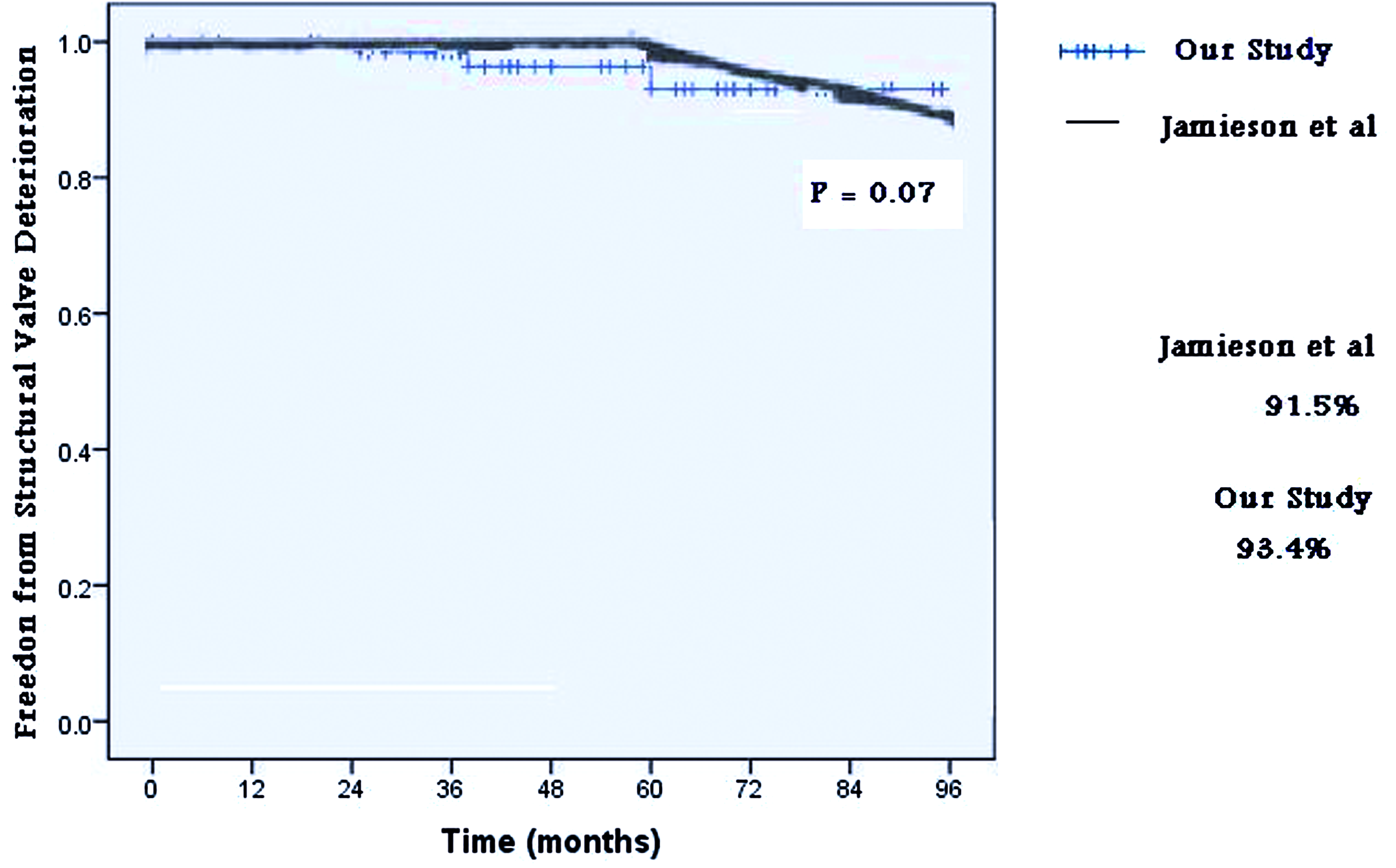
With the follow-up extended to a mean period of 93.9 months, the results show an advantage over second-generation bioprostheses in terms of structural valve deterioration. Notwithstanding differences in patient populations, the current study’s structural valve deterioration curve was compared with a major study on mitral bioprostheses.
17
Because the comparative curve for the 21–40 year age group in the study by Jamieson and colleagues
17
was available in chart form only, it was necessary to read the untransformed values off the chart. With enlarged copies of the chart, the precise point of crossing of the curve was identified at the required studied time; thereafter, values (percentages) were recorded and compared with our study curve. There was a slight statistical advantage in our structural valve deterioration rate compared to that in Jamieson’s study, (p = 0.07; Figure 4), which we expect will show statistical significance on longer follow-up. We do not have a clear explanation for the gross and microscopic findings in the 5 explanted valves so far. Possible explanations are subclinical rheumatic carditis, foreign-body reaction to the Dacron material (many of the changes were close to the autograft-Dacron suture line), and a wear-and-tear phenomenon. The last cause could be theoretically related to the abnormal forces to which the pulmonary cusps are subjugated.
Structural valve deterioration rate in our study and that of Jamieson and colleagues.
17
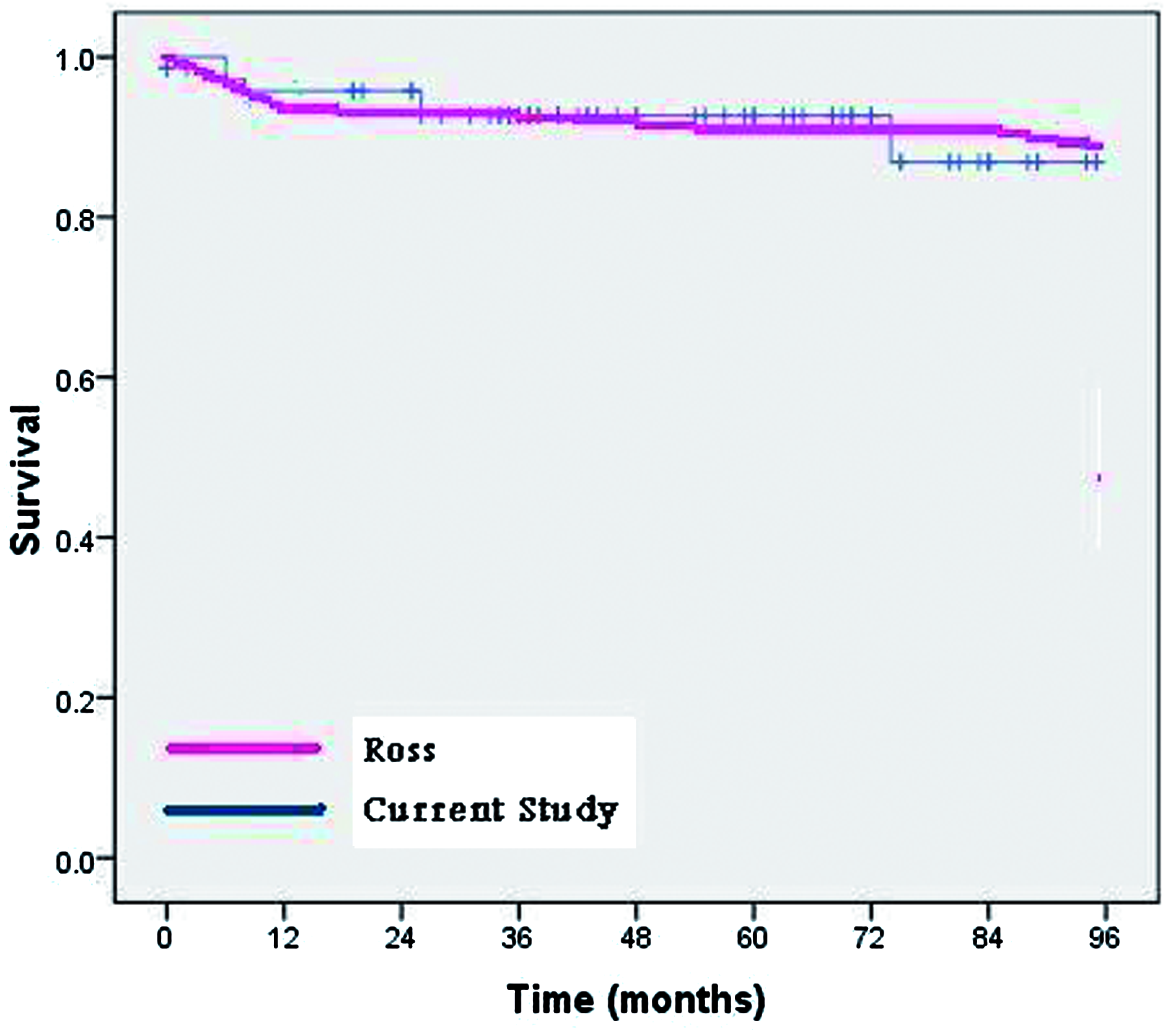
We were able to access the Ross registry on the April 28, 2006, using the following link: http://rossregistry.com/index.html. The website seems to be closed now, possibly due to problems with the domain, but we still have a copy of all the data on hand. Comparison of our reoperation (Figure 5) and survival (Figure 6) actuarial curves with the Ross registry for aortic valve replacement revealed no statistically significant difference in either case. Although the aortic and mitral Ross techniques are different, to us, this finding implies that the pulmonary autograft has generally done as well so far in the mitral position as it has in the aortic. The most important advantage of the pulmonary autograft over the stented bioprosthetic valve is the fact that it is viable and autogenic. A secondary advantage is that it is stentless, with what that entails in terms of accommodating to the changes in the mitral annulus with the cardiac cycle, and also less obstructive in smaller sizes. The main disadvantages of the operation are that it is a relatively prolonged 2-valve operation, and the pulmonary homograft or heterograft is not permanent.
Freedom from reoperation curves in our study and the Ross registry. Survival curves in our study and the Ross registry.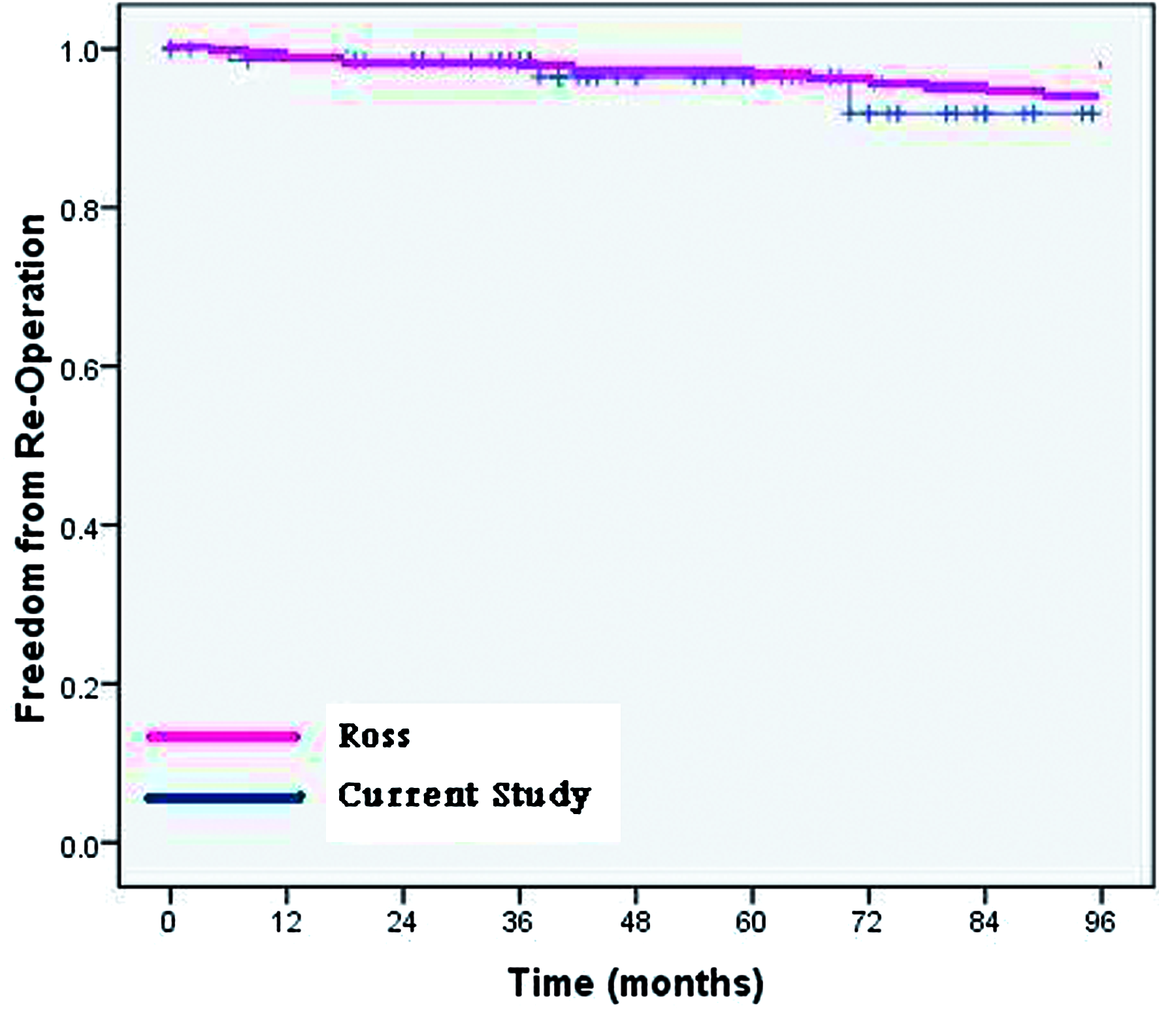
It would seem that the best candidates for this operation are patients who cannot be placed on proper anticoagulation, those who are in sinus rhythm, between 30 and 50 years of age, and have no involvement of other valves or other comorbid conditions. Below 30 years of age, the MV can often be repaired, and there is the lurking danger of resurgent rheumatic activity. Above 50 years of age, the quality of the pulmonic valve is in doubt, and the advantages over the stented bioprosthesis become less obvious. There is no question that there will be a small percentage of our rheumatic patients (especially among the very young) who will have recurrent rheumatic activity that will affect the autograft, just as is the case with the classic Ross procedure. 18 However, this mishap can probably be largely avoided by proper prophylaxis, and we do not believe it is a good reason to deny the benefits of the operation to the majority of our mitral patients. Whether patients with atrial fibrillation should be offered this operation remains an issue. At least 60% of these patients can now be cured with various forms of ablation therapy applied during the operation. Furthermore, anticoagulation for those who fail to be ablated is not as contentious as it is for patients with mechanical valves. Still, there is no escaping the fact that the benefits of the Ross II operation decrease appreciably if patients sustain their atrial fibrillation postoperatively.
One indication for this operation which has not yet been fully explored, is the complex irreparable congenital MV defect. 19 Our series included 2 children with complex congenital malformations, and we attempted to manage the problem of potential growth of the conduit by slitting the Dacron tube on one side in one child, and on 2 sides in the other. However, we did not have the opportunity to observe autograft/conduit growth in these children because in one case, the autograft had to be explanted for endocarditis, and the other child was lost to follow-up. If a way can be found to allow the autograft/conduit to grow with the child, our operation would provide a valuable option for pediatric cardiac surgeons facing a previously insoluble situation.
Presented at the 5th Biennial Meeting of the Society for Heart Valve Disease, Berlin, Germany, January 27–30, 2009.
Footnotes
Acknowledgment
The authors are grateful to Ms Randa Jaafari for her assistance in preparing the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.