
Abstract
Aneurysms of the thoracic aorta can have various manifestations, some of which may simulate esophageal diseases, clinically and radiographically. Aortoesophageal fistula is rare and usually fatal. We report a case of aortoesophageal fistula presenting with progressive dysphagia and intermittent episodes of upper gastrointestinal bleeding.
Introduction
The clinical presentation of aortic aneurysm varies and may mimic other more common diseases. Aortic aneurysm is often discovered as an incidental finding on routine physical examination or chest radiography. Aneurysms of the thoracic aorta may simulate esophageal diseases, clinically and radiographically. This could be due to compression of the esophagus by an aneurysm or aortoesophageal fistula.
Case Report
A 54-year-old woman presented with progressive dysphagia and 2 episodes of upper gastrointestinal bleeding 2 months earlier. She had history of a traffic accident 10 years earlier. She reported no significant recent weight loss. A barium study showed irregularities in the middle to distal portion of the esophagus, highly suggestive of malignancy. Upper gastrointestinal endoscopy showed only hiatus hernia and suspicious points at which biopsies were taken. Chest computed tomography with contrast revealed a large air-mixed non-homogenous mass adjacent to the proximal third of the descending aorta, with compression of adjacent structures, suggestive of advanced malignant tissue. Transthoracic echocardiography showed mild aortic insufficiency and mild mitral regurgitation, a left ventricular ejection fraction of 55%, and no regional wall motion abnormality. Repeat upper gastrointestinal endoscopy was refused by a gastroenterologist for fear of aortic pseudoaneurysm rupture. Computed tomographic angiography showed 2 large out-pouchings at the start of the descending aorta (Figure 1). Serology tests for syphilis were negative. Because of another episode of upper gastrointestinal bleeding and to avoid further delay, aortography was not performed. Emergency surgery was undertaken with a high suspicion of aortoesophageal fistula. Early exploration through a left posterolateral thoracotomy showed no evidence of advanced malignancy with mediastinal extension. Partial cardiopulmonary bypass was established through the left groin, and the patient was cooled to 32°C. Exploration revealed 2 large out-pouchings: a smaller one just posterior to the origin of the left subclavian artery, extending toward the posterior mediastinum; and a larger one just in the isthmus, extending toward the medial side of the descending aorta and anteriorly. The descending thoracic aorta was opened, and the larger anterior outpouching was found to contain a large clot. After evacuation of the clot, the proximal third of the descending aorta was replaced using a 24F Dacron tubular graft. The patient was discharged in good condition on oral fluconazole. She was asymptomatic and in good health with no evidence of infection or mediastinitis at 1 month postoperatively. Subsequent upper gastrointestinal endoscopy was normal.
(A–E) Computed tomographic angiography showing two large out-pouchings at the start of the descending aorta.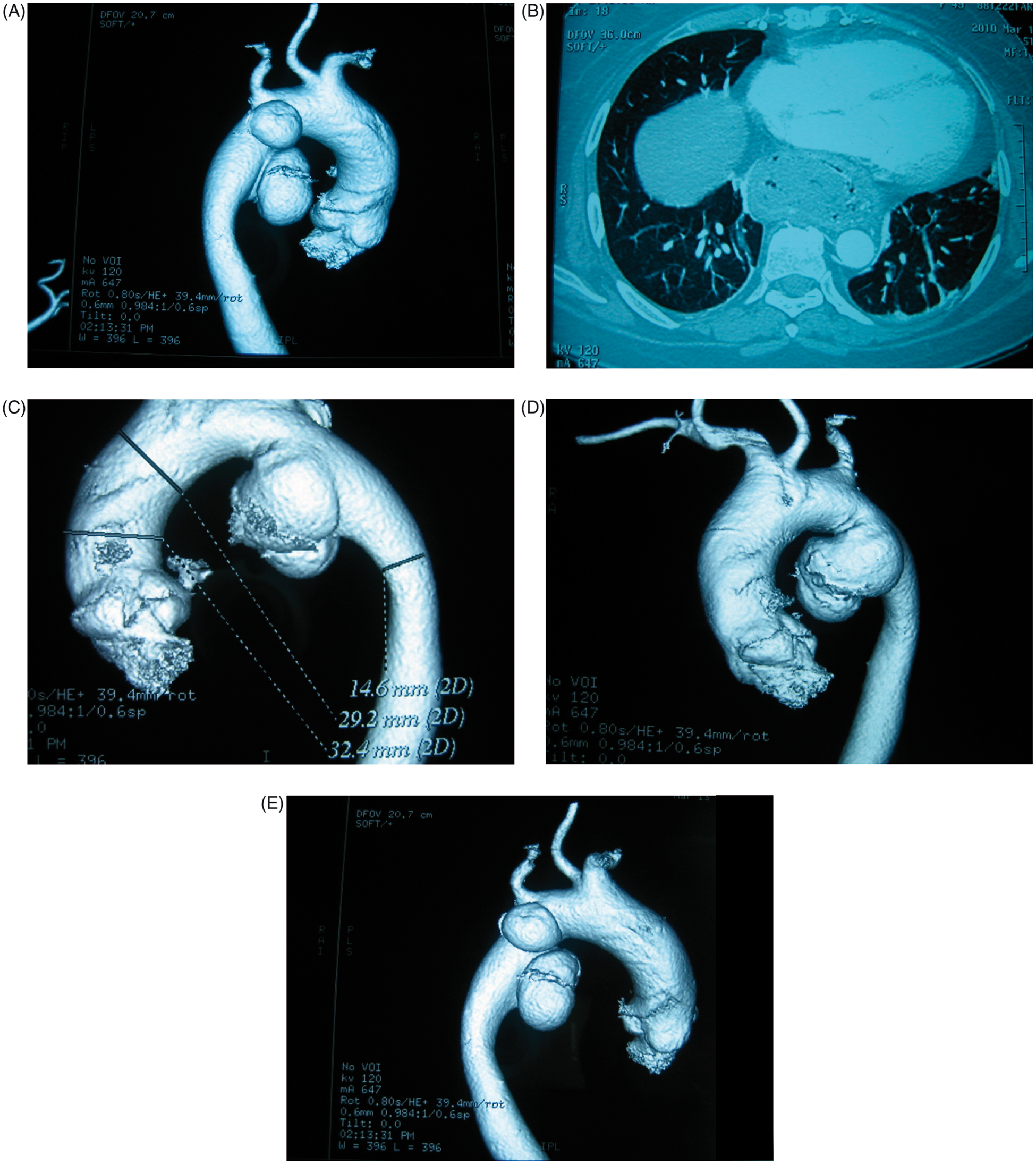
Discussion
Patients with thoracic aortic disease are difficult to treat because they are frequently older with multiple comorbidities. Aortoesophageal fistula is a devastating complication resulting from a variety of thoracic conditions, which is uniformly fatal unless promptly treated. Several primary causes for its development have been reported, with the instigating event arising from either the aorta (thoracic aortic aneurysm) or the esophagus (thoracic malignancy). The majority are due to secondary causes such as swallowing a foreign body or previous intrathoracic esophageal or aortic surgery. 1 Aneurysms were the most common cause of such fistulas in a series reported by Carter and colleagues. 2
With recent advances in intraluminal stent technology, a combination of aortic and esophageal stenting has been advocated for treatment of aortoesophageal fistula. Stent infection, migration, and immediate availability have limited their use. In a case report by Assink and colleagues 3 , computed tomography of a patient with massive upper gastrointestinal bleeding after swallowing a fish bone demonstrated a fistula from the proximal descending thoracic aorta to the mid esophagus. A 28-mm Talent stent-graft was delivered transfemorally to repair the aortic defect. Another report described a patient with esophageal carcinoma who developed massive hematemesis due to aortoesophageal fistula after irradiation therapy; emergency treatment with an endovascular stent-graft was successfully performed. 4 A review of all patients with aortoesophageal and aortobronchial fistulas undergoing thoracic endovascular aortic repair in 3 European teaching hospitals, concluded that this treatment can prevent immediate exsanguination in such patients. 5
Computed tomography in our patient showed no evidence of significant chest trauma but a large air-mixed non-homogenous mass around the aorta and central mediastinal structure, suggestive of advanced malignant tissue. A barium swallow was indicative of malignancy. The first endoscopy was suspicious for esophageal cancer, although another after the operation revealed only diffuse esophageal candidiasis. Given the ambiguous results and unstable condition of patient, we preferred emergency surgery. Dysphagia and gastrointestinal bleeding are rare presentations of thoracic aortic aneurysm. Cardiac surgeons should be aware of this rare cause of gastrointestinal bleeding and dysphagia, to avoid a catastrophic endoscopic biopsy. Aortography is useful to confirm the diagnosis, but a preoperative barium swallow is a simple and more comfortable means of achieving a diagnosis of aortoesophageal fistula. Immediate surgery is the only lifesaving intervention.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.