
Abstract
A 64-year-old man, who had received chemoradiation therapy for stage IIIB non-small-cell lung cancer, underwent stent insertion with a covered expandable metallic stent for post-radiation bronchial stenosis. Stenosis due to formation of granulation tissue at the distal stent site resulted in critical respiratory failure. The stent was removed after 43 months, using rigid bronchoscopy.
Introduction
Removal of a long-term covered expandable metallic stent (EMS) is hazardous, but occasionally indicated. We describe a case of successful EMS removal using rigid bronchoscopy.
Case Report
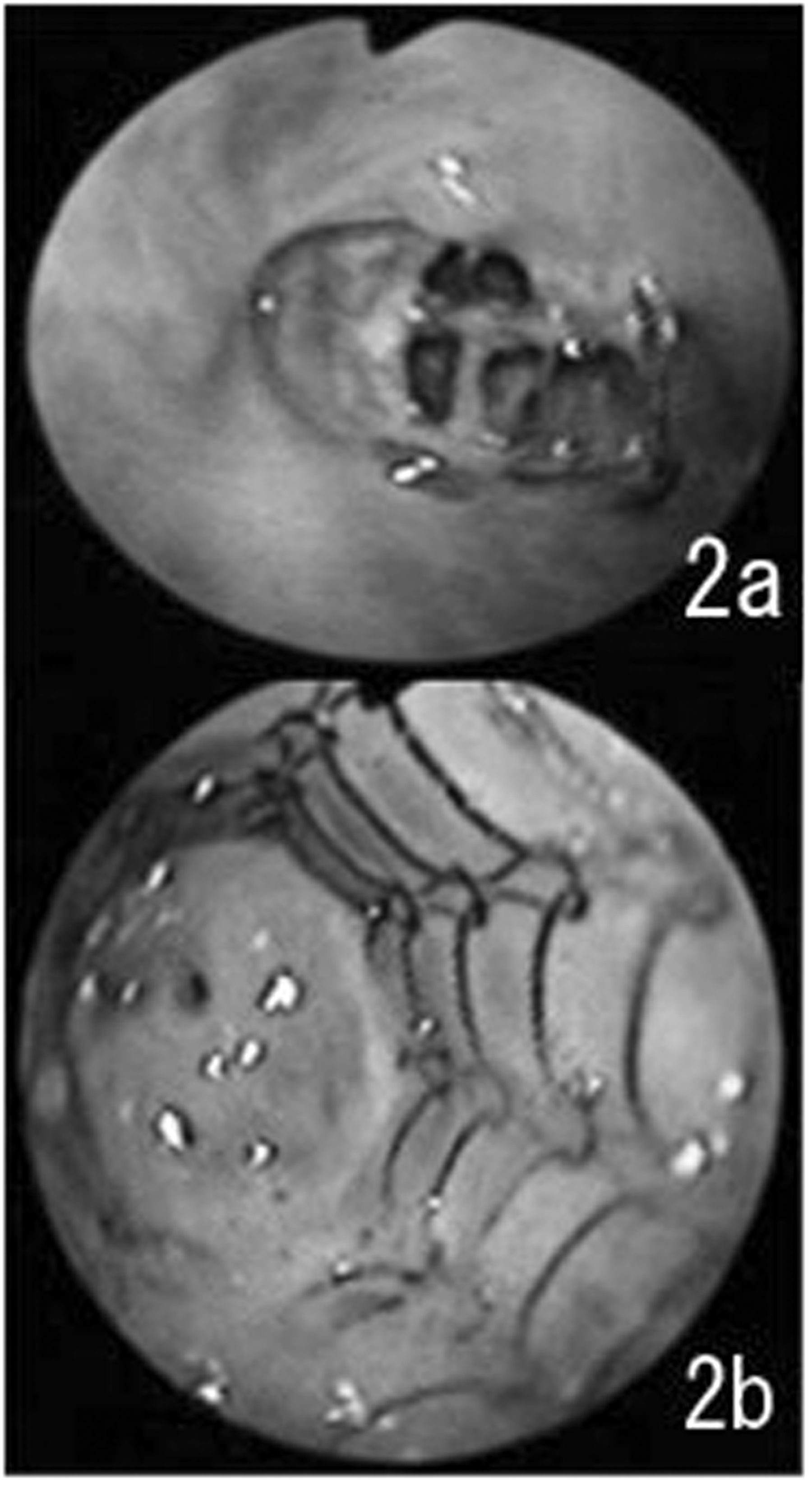
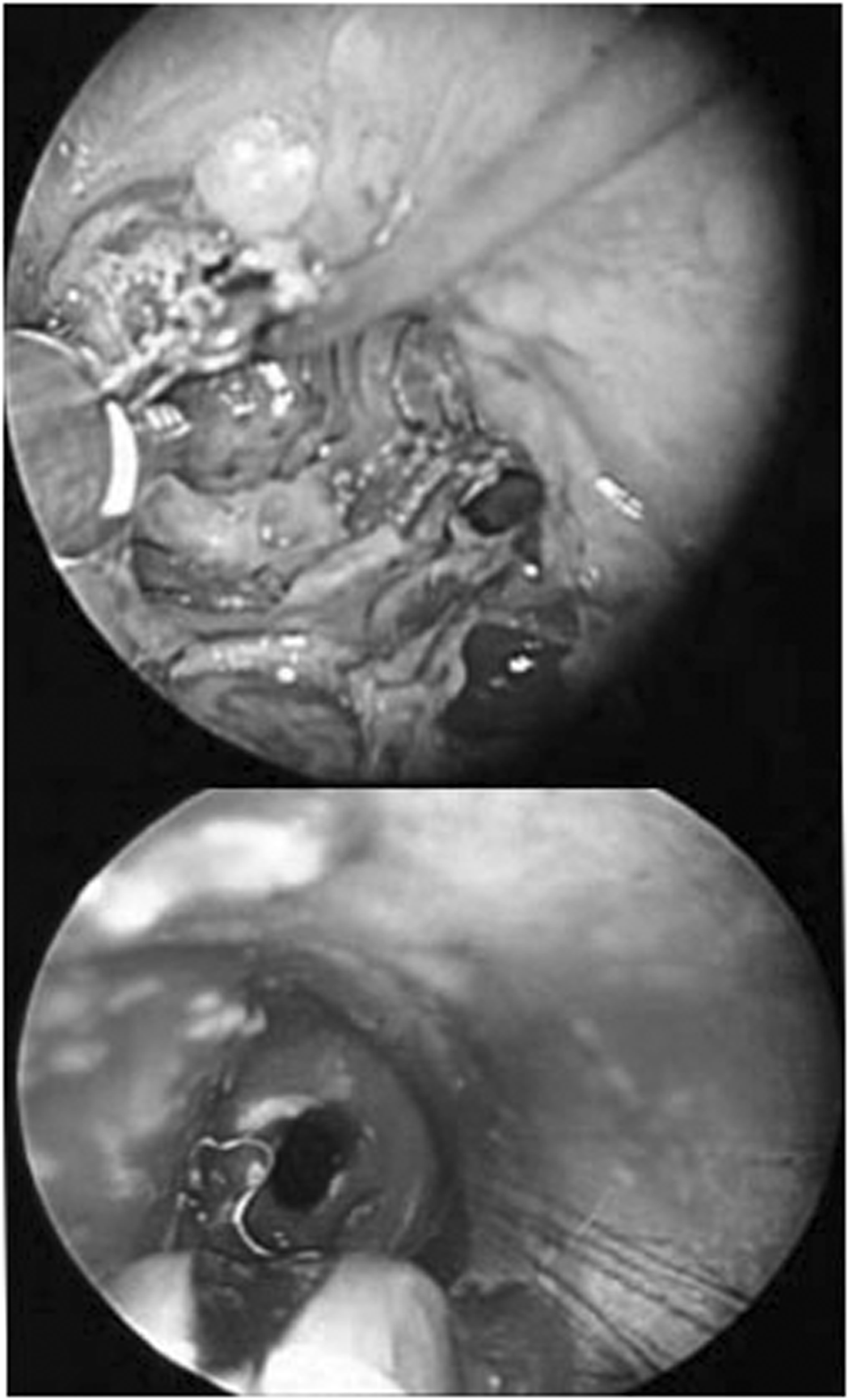
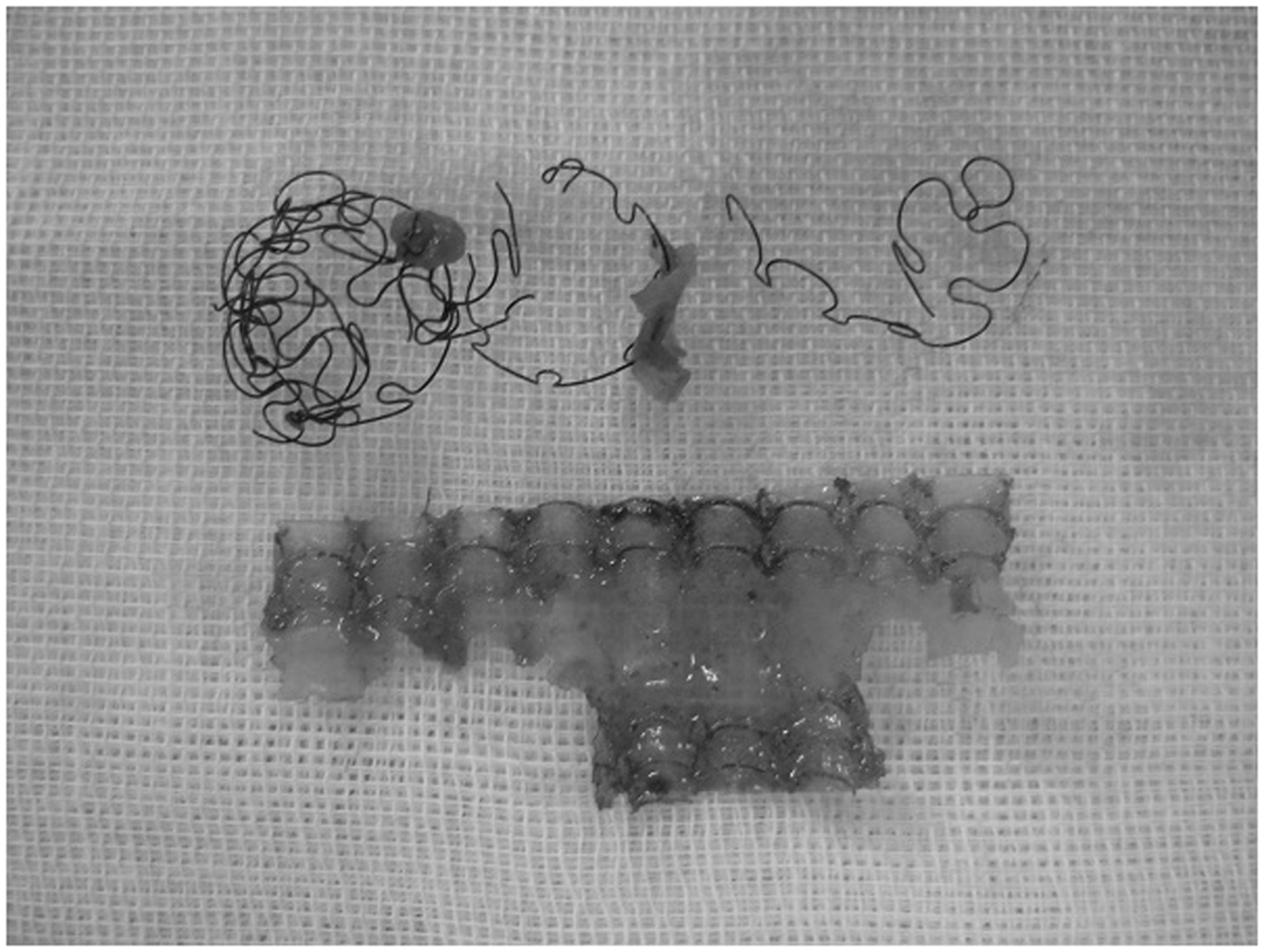
A 64-year-old man underwent chemoradiotherapy (3 cycles of carboplatin plus paclitaxel, and 60Gy of radiation) after a diagnosis of squamous cell lung carcinoma (c-T4N2M0 stage IIIB), achieving a complete response, at another hospital. He suffered scar contraction with left main bronchial stenosis, and a covered EMS (Ultraflex, 12 × 3 mm) was placed. He presented 18 months after stenting with respiratory symptoms of cough and sputum, and stent migration into the carina was found on computed tomography and fiberoptic bronchoscopy (Figure 1). Respiratory failure progressed, and home oxygen therapy was initiated 36 months after stenting. He was referred to our hospital 43 months after stenting, because no conservative treatment was available. He was wheezing with severe dyspnea on admission (performance status 3). Hypoxemia (PaO2 64.5 Torr, O2 1.5 L·min−1) was found on arterial blood gas analysis, which was slightly improved in the right lateral decubitus position, suggesting hypoventilation of the left lung. Computed tomography showed migration of the EMS into the trachea, with stenosis at the distal end and a suspected second primary lung cancer in the right upper lobe bronchus. Intraoperative fiberoptic bronchoscopy showed viscous white sputum at the proximal end of the migrated EMS in the trachea, and granulation tissue stenosis with a pin-hole at the distal end (Figure 2). Through rigid bronchoscopy, the EMS was removed in fragments, using rigid alligator forceps, but small fragments of the wire were left in the bronchial wall (Figures 3 and 4). The stenosis was bored out with the tip of the rigid bronchoscope, and a silicone stent (Dumon straight, 12 mm × 3 cm) was placed for prevention of bleeding and restenosis. Operative time was 138 min, with only minor blood loss. The patient showed improvements in general condition (performance status 1) and was discharged to the primary hospital without O2 inhalation on postoperative day 13. The tumor in the right upper bronchus was diagnosed as a second primary squamous cell carcinoma, and treated with chemotherapy. The silicone stent was removed 6 months later using rigid bronchoscopy, because of granulation tissue stenosis at the proximal end.
Findings on fiberoptic bronchoscopy and computed tomography 18 months after deploying the covered expandable metallic stent. The proximal end of the migrated stent is attached to the right side of the tracheal wall. Intraoperative findings on flexible bronchoscopy. (a) Migration of the expandable metallic stent into the trachea. (b) Severe granulation tissue stenosis at the distal end. Removal of the expandable metallic stent using rigid bronchoscopy. The covered expandable metallic stent being retrieved in piecemeal fashion.
Discussion
Placement of an EMS is widely used for the treatment of malignant airway stenosis, because the procedure is less invasive using a flexible bronchoscope. An EMS is also indicated for distal visible airway lesions because of its advantages of thinner walls and more flexibility compared to silicone stents. In principle, an EMS is applied for permanent placement and should not be used for benign disorders, according to the guidelines proposed by the USA Food and Drug Administration in 2005, because removal is considered dangerous. A removable silicone stent or surgery should be considered initially in patients with benign diseases. 1 However, some patients develop indications for stent removal (granulation formation, stent fracture or failure, or accomplishment of treatment). Alazemi and colleagues 2 retrospectively analyzed 46 cases and concluded that EMS removal was feasible but associated with significant complications and costs. Several approaches are available to retrieve EMS. 3 – 5 No major complications or operative deaths have been reported using a rigid bronchoscope. 6 – 8 Removal of an EMS after long-term placement (50 months) has also been reported, but is associated with a high risk of morbidity. 7,8
In our patient, respiratory failure had progressed rapidly because of granulation tissue stenosis at the distal end of the EMS. Although endoscopic balloon dilation of the stenosis was an option, restenosis was expected after palliative treatment. Removal of the EMS by thoracotomy was unfeasible due to hilar adhesions resulting from the irradiation therapy and proximal migration to the trachea. We removed the EMS in piecemeal fashion, using rigid bronchoscopy, although small fragments of wire remained in the bronchial wall. Complete removal as a single unit may be difficult after long-term placement of an EMS. In retrospect, a silicone stent would have been a better initial choice in this case, because of bronchial stenosis due to post-radiation scarring. We placed a silicone stent but restenosis was found at the proximal end 6 months later; remnants of wire from the EMS might have promoted granulation. Careful follow-up with computed tomography or fiberoptic bronchoscopy is necessary after re-stenting, because 40% of patients suffer restenosis and require stent replacement. 6 Removal of a covered EMS after long-term placement is a practical option, although the procedure is associated with the risk of complications.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflicts of interest statement
None declared.