
Abstract
Chest radiography in a 59-year-old woman with recurrent pneumonia showed infiltrates in her left upper lung field. Fiberoptic bronchoscopy and chest computed tomography revealed severe constriction in the upper bronchus and a nodule in the left upper lobe. After lobectomy, adenocarcinoma was confirmed, with multiple non-caseating granulomas in the lung parenchyma and lymph nodes. Bronchial constriction was thought to be due to a sarcoid-like reaction secondary to lung cancer, leading to granuloma formation.
Introduction
Sarcoidosis is a systemic inflammatory disorder characterized by non-caseating granuloma formation. 1 Non-caseating granulomas are also seen in patients with malignant neoplasms, mycobacterial infection, pneumoconiosis, and are referred to as a sarcoid-like reaction. 2 Distinguishing a sarcoid-like reaction from systemic sarcoidosis is difficult on pathologic examination, and making a diagnosis of sarcoidosis usually requires compatible clinical features and lack of an alternative explanation for non-caseating granulomas.
Case report
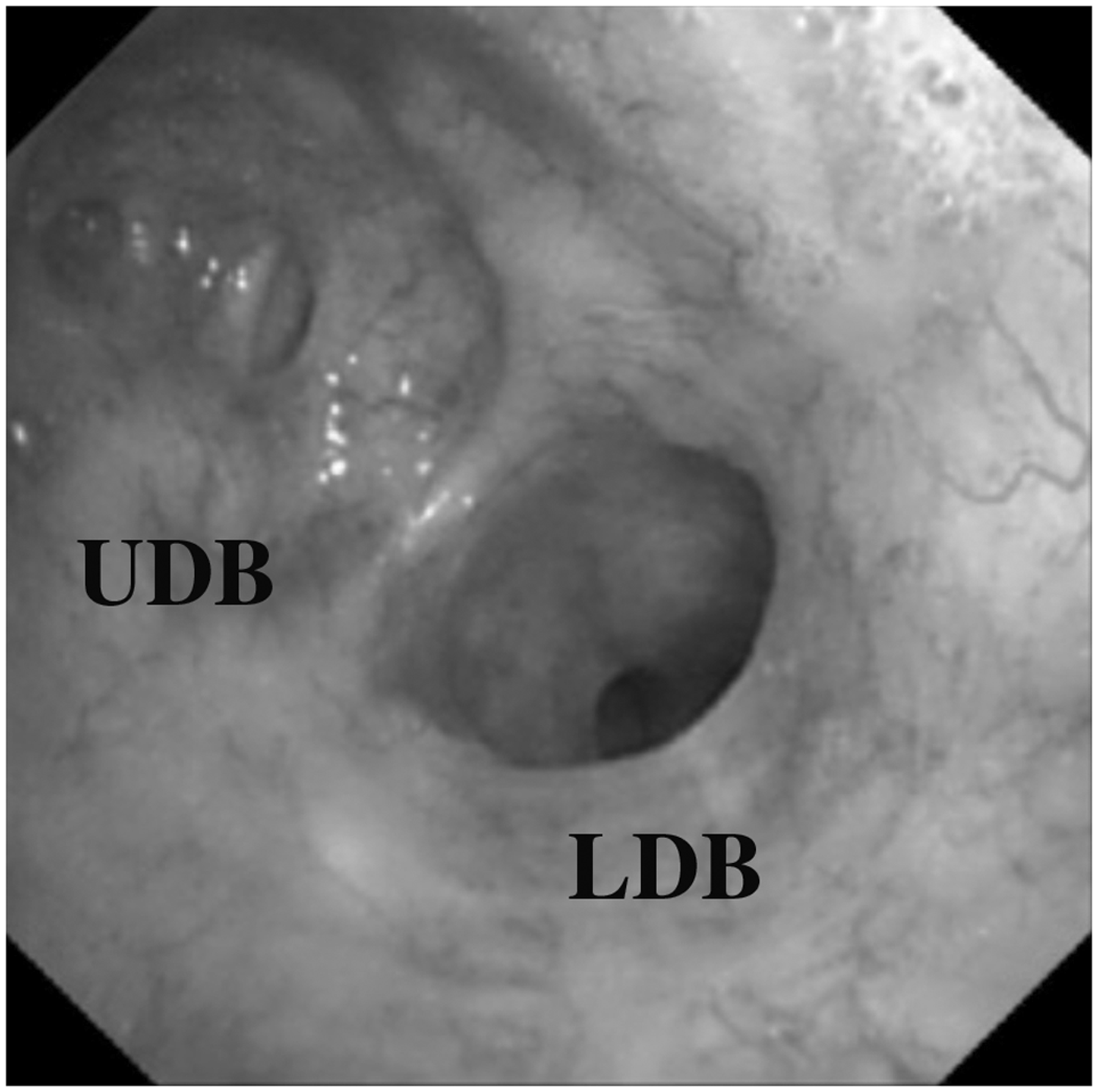
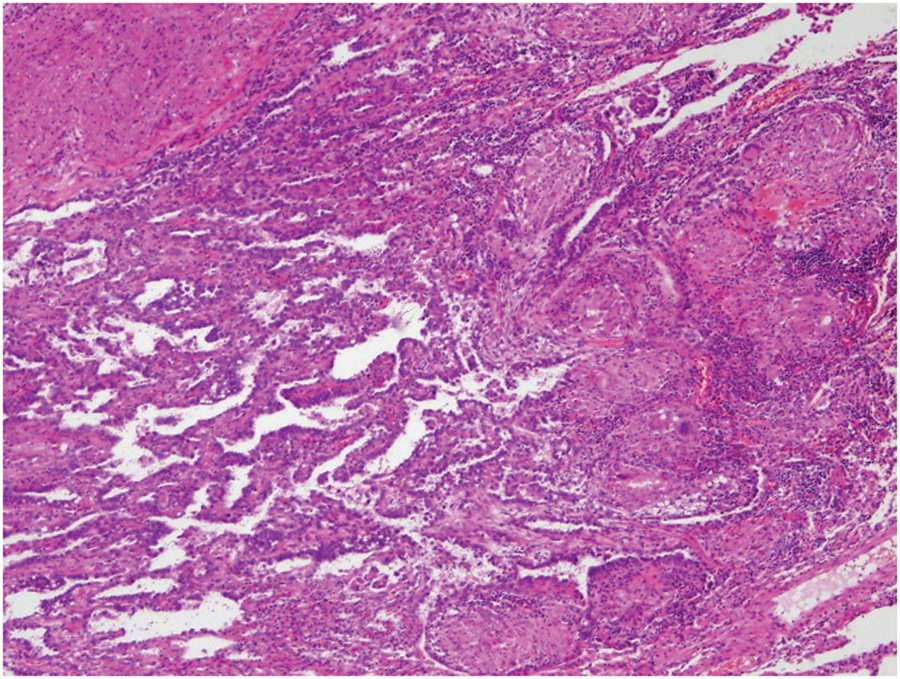
A 59-year-old woman with a high fever and productive cough was referred for treatment at our hospital. She had a history of recurrent pneumonia in her left upper lobe for 6 years. Chest radiography showed infiltrates in her left upper lung field. Laboratory tests revealed elevated white blood cell count and C-reactive protein. With a diagnosis of pneumonia, intravenous administration of antibiotic agents was initiated. Although her symptoms gradually improved, a nodular shadow in her left upper lung field on chest radiography remained. Chest computed tomography showed a solid nodule of 15 mm in diameter in her left upper lobe (Figure 1). Fiberoptic bronchoscopy revealed a severe constriction in the left upper division of the upper bronchus (Figure 2). Transbronchial lung biopsy was not achieved due to stricture of the airway. We considered that the history of recurrent pneumonia was due to the bronchial constriction and may continue to recur unless the stricture was managed. We also thought that the nodule in the left upper lobe could be lung cancer, so we conducted a left upper lobectomy with mediastinal lymph node sampling after obtaining informed consent. A 15 × 15 × 10 mm tumor was located in the apical-posterior segment of the left upper lobe. The upper division of the left upper bronchus showed extreme narrowing at its entry. Pathologic examination revealed that the lung nodule was an adenocarcinoma associated with multiple non-caseating granulomas in the lung parenchyma and lymph nodes (Figure 3). Non-caseating granulomas and fibrous thickening of the tissue were also noted at the site of the bronchoconstriction. No evidence of mycobacterial infection was seen on pathology. Sarcoidosis or a sarcoid-like reaction was suspected, so additional systemic examinations were conducted. No abnormal accumulations were found, including mediastinal-hilar lymph nodes on systemic gallium scintigraphy. No involvement of sarcoidosis was revealed in the eyes or heart. There was no elevation of serum angiotensin-converting enzyme or calcium. We concluded that the bronchial constriction was due to a sarcoid-like reaction secondary to lung cancer, leading to granuloma formation. The patient recovered uneventfully, and had remained well a year after the surgery.
Chest computed tomography showing a nodule, 15 mm in diameter, in the left upper lobe. Bronchoscopy showing a severe constriction in the left upper division of the upper bronchus. LDB = lingular division of the bronchus, UDB = upper division of the bronchus. Papillary adenocarcinoma and multiple non-caseating epithelioid cell granulomas around the tumor were observed on histopathological examination. Hematoxylin and eosin stain, original magnification×200.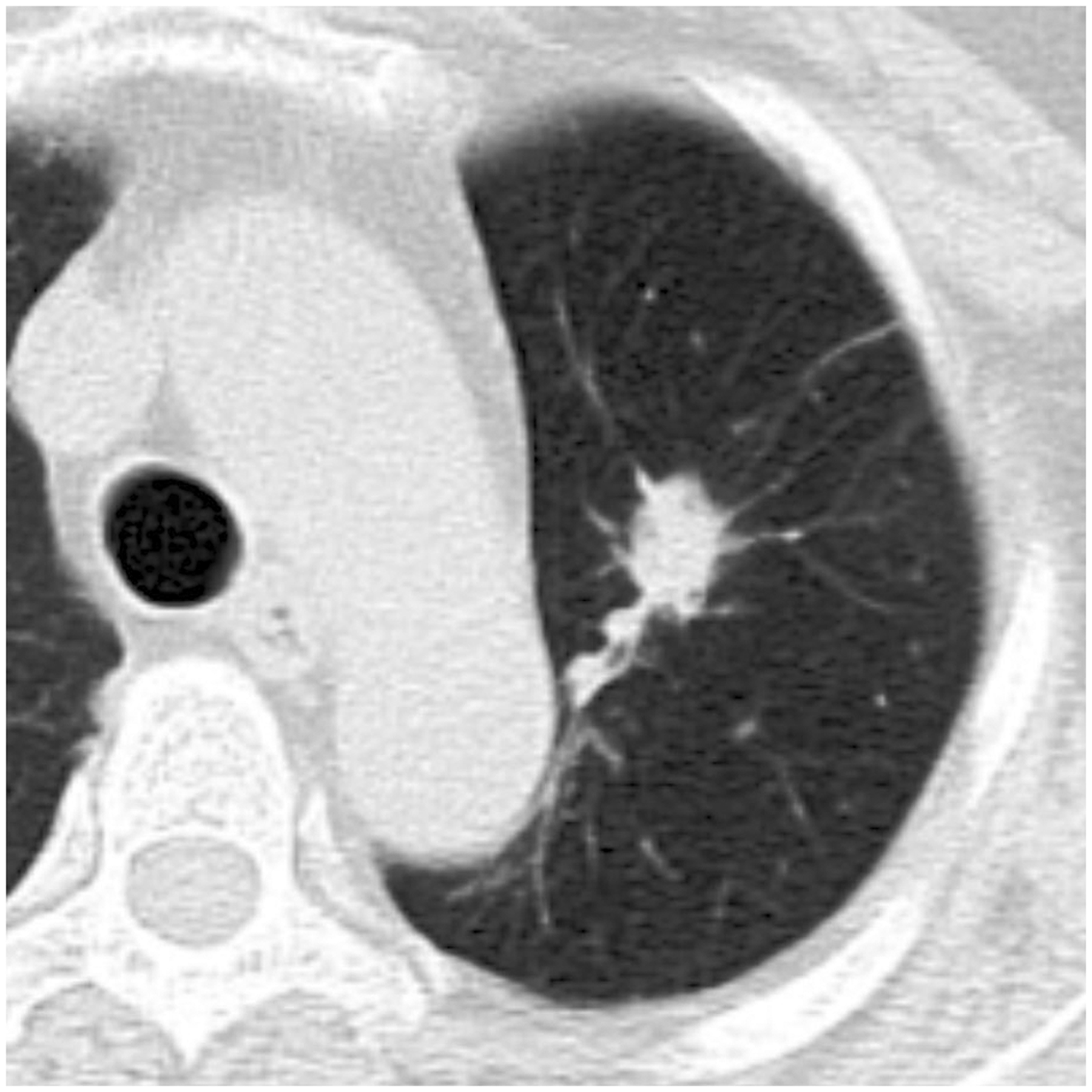
Discussion
Non-caseating granulomas are occasionally seen in tissue around a malignant neoplasm or in regional lymph nodes, and are referred to as a sarcoid-like reaction or sarcoid reaction, distinguishing them from systemic sarcoidosis. 2 In lung cancer, 1.3% to 3.2% of the regional lymph nodes have been reported to show a sarcoid-like reaction. 3,4 The pathogenesis of this sarcoid-like reaction in cancer-bearing patients is not fully understood, although it has long been speculated to be a local expression of an immune response to the neoplasm. 1 Making a diagnosis of sarcoidosis usually requires compatible clinical features and no evidence of other diseases that can lead to granuloma formation.
We recognize that whether the bronchial constriction in this woman was due to sarcoid-like reaction to lung cancer or to subclinical systemic sarcoidosis remains unclear. Because she did not manifest bilateral hilar lymph node swelling, accumulation on systemic gallium scintigraphy, or elevation of serum angiotensin-converting enzyme and calcium, makes it less likely that she had systemic sarcoidosis. She had been suffering recurrent pneumonia in her left upper lobe for 6 years, suggesting that her bronchoconstriction had developed 6 years earlier. If the patient had lung cancer not clearly detectable on imaging modalities at that time (2 mm in diameter for example), the volume doubling time of her tumor was calculated as 250 days. 5 The estimated volume doubling time is in line with reports of that for lung adenocarcinoma of 223 to 384 days. 6,7 Taken together, the presumption that her bronchial constriction was the result of a sarcoid-like reaction to lung cancer is reasonable. Nevertheless, the possibility that she has systemic sarcoidosis cannot be discarded completely considering that airway constriction in sarcoidosis is often seen in the left upper bronchus, and repeated obstructive pneumonia is a risk factor for lung cancer; 8 thus making continuous follow-up indispensable.
Footnotes
Acknowledgment
We thank Dr. Tomoyuki Murakami for his helpful advice on pathologic assessment.
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflicts of interest statement
None declared.