
Abstract
Two girls aged 1 and 15 years with heart murmurs were diagnosed with aortico-left ventricular tunnel. In the 1-year-old, the tunnel had an intracardiac aneurysm within the right ventricular outflow tract; both openings were closed The 15-year-old had no aneurysmal dilatation, but she had mild aortic regurgitation; the aortic opening of the tunnel was closed with a patch. Both girls had uneventful postoperative courses with excellent early results.
Introduction
Aortico-left ventricular tunnel (ALVT) is a congenital abnormally endothelialized communication between the ascending aorta and the left ventricle. We report 2 cases of ALVT with successful surgical treatment.
Case report
Case 1
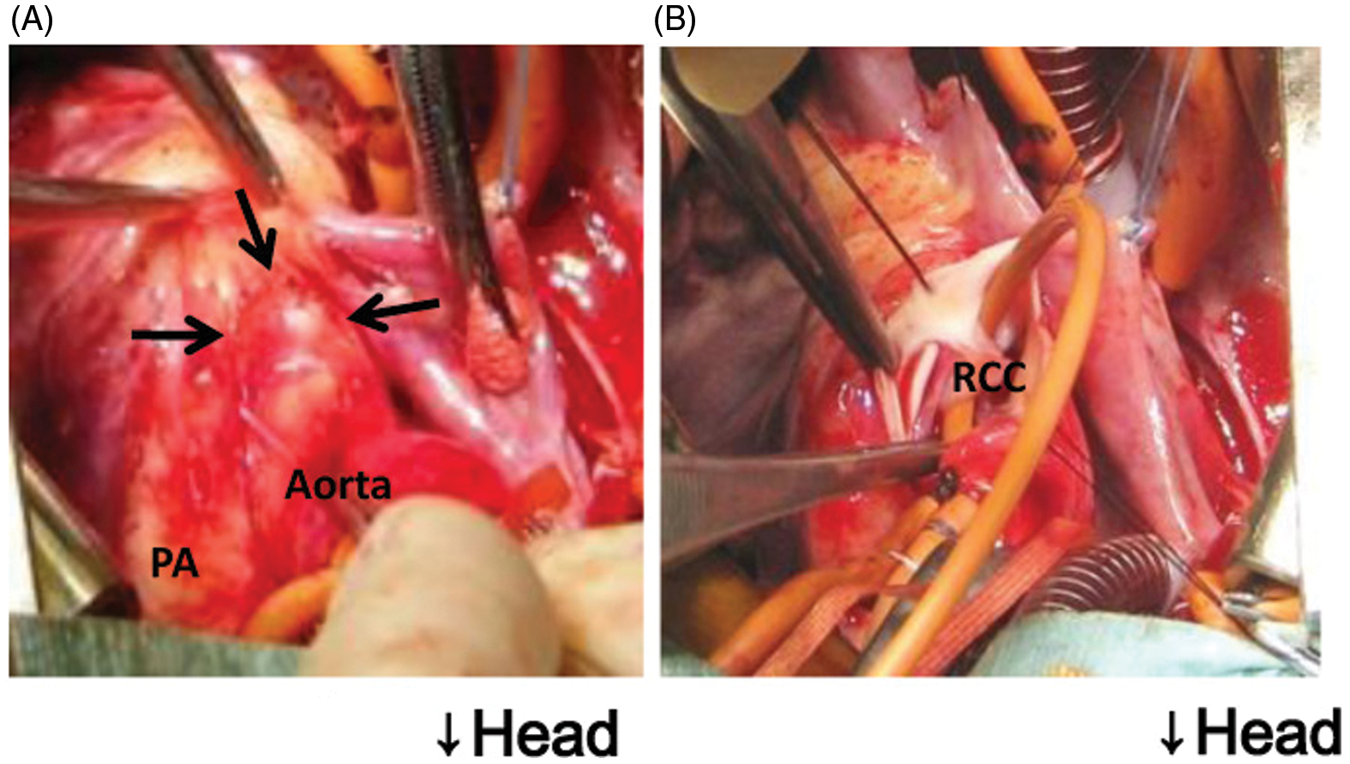
A 1-year-old girl with a heart murmur was referred to our institute without any symptoms. On examination, the presence of ALVT was revealed by computed tomography and cardiac catheterization (Figure 1). The tunnel had an intracardiac aneurysm, and it projected into the right ventricular outflow tract (type III). There was no pressure gradient in the right ventricular outflow tract, no ventricular septal defect, and no aortic regurgitation (AR). Her left ventricle was dilated with a left ventricular end-diastolic volume of 161% of the normal value. Surgery was performed at the age of 1 year. A small external bulge was found at the aortic root. After initiation of cardiopulmonary bypass and crossclamping of the aorta, the aortic root was transversely incised and the aortic opening of the tunnel was recognized just below the right coronary artery orifice. The opening was 5 mm in diameter (Figure 2). The tunnel extended into the intracardiac aneurysmal cavity and communicated with the left ventricle just below the commissure of left and right coronary cusps. The tunnel was closed at both openings; the aortic side was closed primarily with pledgeted stitches, the left ventricular orifice was closed with an expanded polytetrafluoroethylene patch. The postoperative course was uneventful. Postoperative echocardiography showed no residual abnormal blood flow in the tunnel and no AR.
Preoperative computed tomography scans. (A) Arrows indicate the intra- and extracardiac aneurysm formation in the aortic-left ventricular (LV) tunnel underneath the right coronary artery (RCA). (B) Arrowheads indicate the cavity of the aortic-left ventricular tunnel. The aortic opening is beneath the RCA. The LV opening is just below the commissure of the left coronary cusp (LCC) and right coronary cusp (RCC). Intraoperative views. (A) Arrows indicate the extracardiac bulge. (B) The tunnel openings are seen through the aortotomy. A flexible catheter was passed from the aortic opening to the left ventricular opening. PA: pulmonary artery; RCC: right coronary cusp.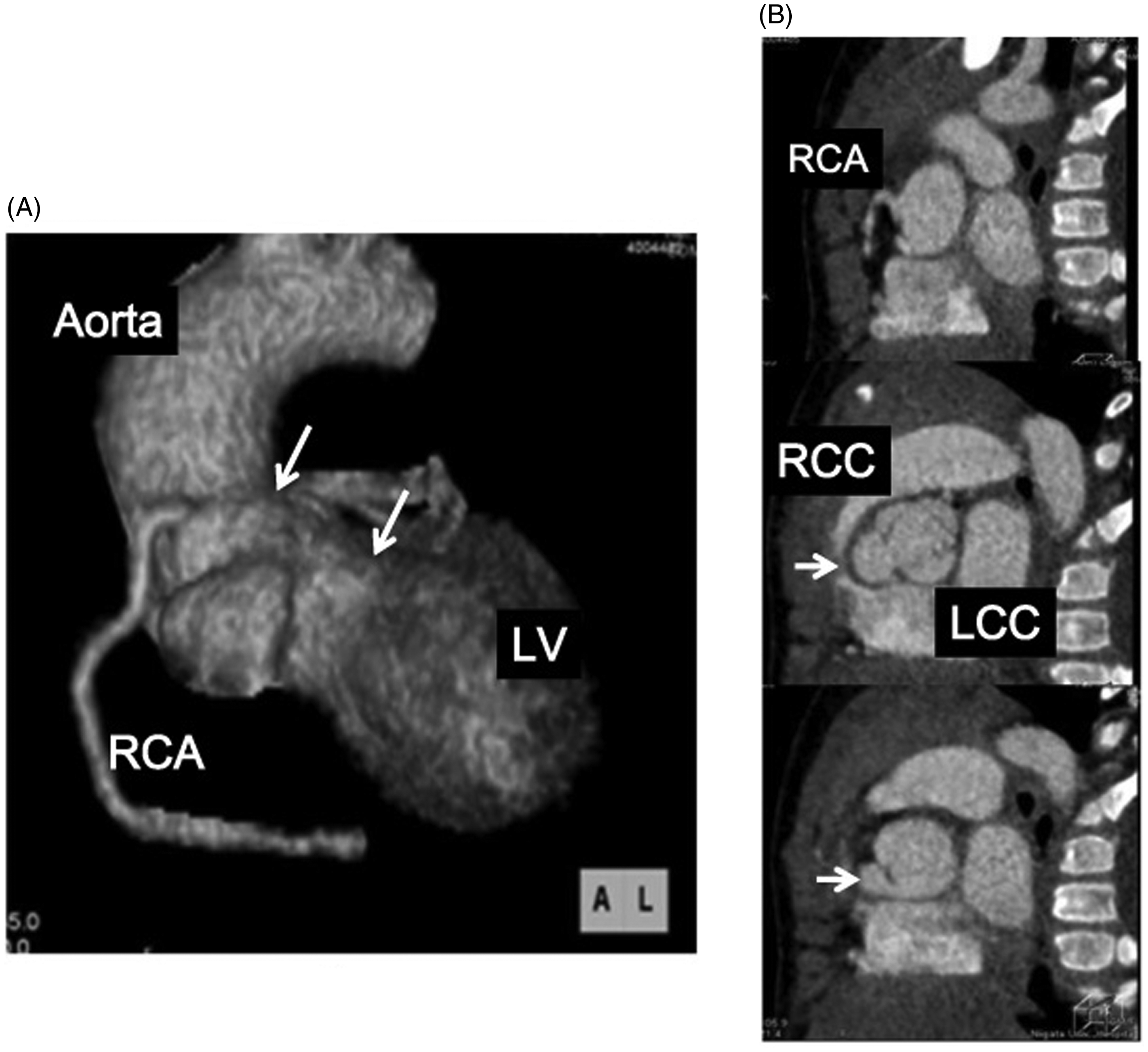
Case 2
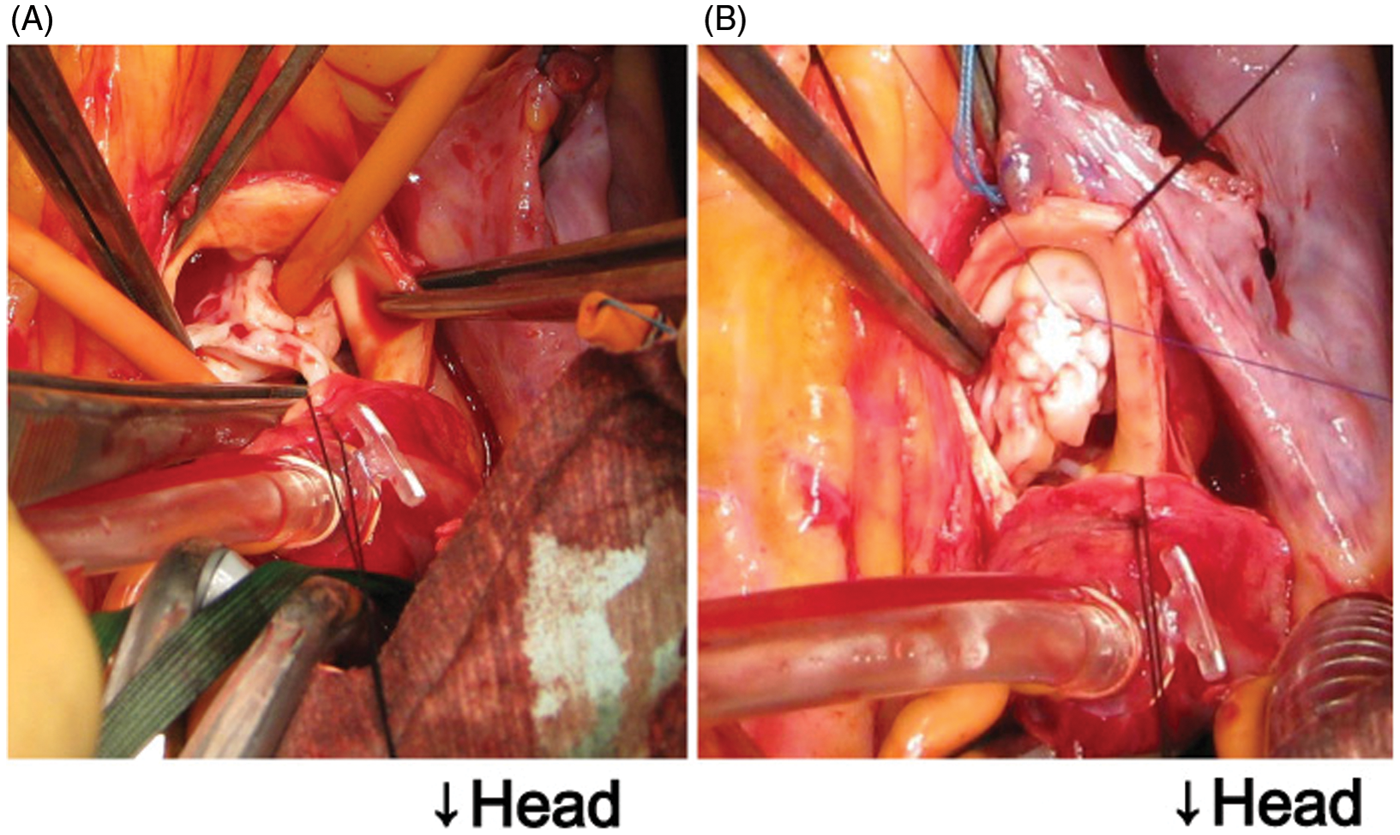
A 15-year-old girl was referred to our hospital for cardiac evaluation. A heart murmur had been noticed at the age of 10 years, and she was diagnosed as having AR. She was followed up for 4 years, and recently, she complained of general fatigue and dyspnea on effort. Echocardiography and computed tomography showed ALVT (Figure 3). Cardiomegaly was also seen, and the left ventricular end-diastolic volume index was 166 mL·m−2. An intracardiac aneurysm of the tunnel was not found, but mild AR was recognized. Surgery was performed at the age of 15 years. Cardiopulmonary bypass was initiated and an aortotomy was made after aortic crossclamping. The aortic opening of the tunnel was found just above the commissure of the right and noncoronary cusps (Figure 4). The left ventricular opening of the tunnel was below the right coronary cusp. Both openings of the tunnel were 5 mm in diameter. The right and noncoronary cusps were slightly thickened and shortened. The aortic opening of the tunnel was closed with an expanded polytetrafluoroethylene patch. The postoperative course was uncomplicated. Postoperative ultrasound showed a tiny residual tunnel flow and mild aortic regurgitation.
Preoperative computed tomography. (A) Arrowheads indicate the cavity of the aortic-left ventricular tunnel. (B) Ventricular opening of the tunnel present just below the right coronary cusp (RCC). Intraoperative views. (A) Through the aortotomy, the tunnel openings are seen. A flexible catheter is passed from the aortic opening to the left ventricular opening. (B) Aortic opening closed with a patch.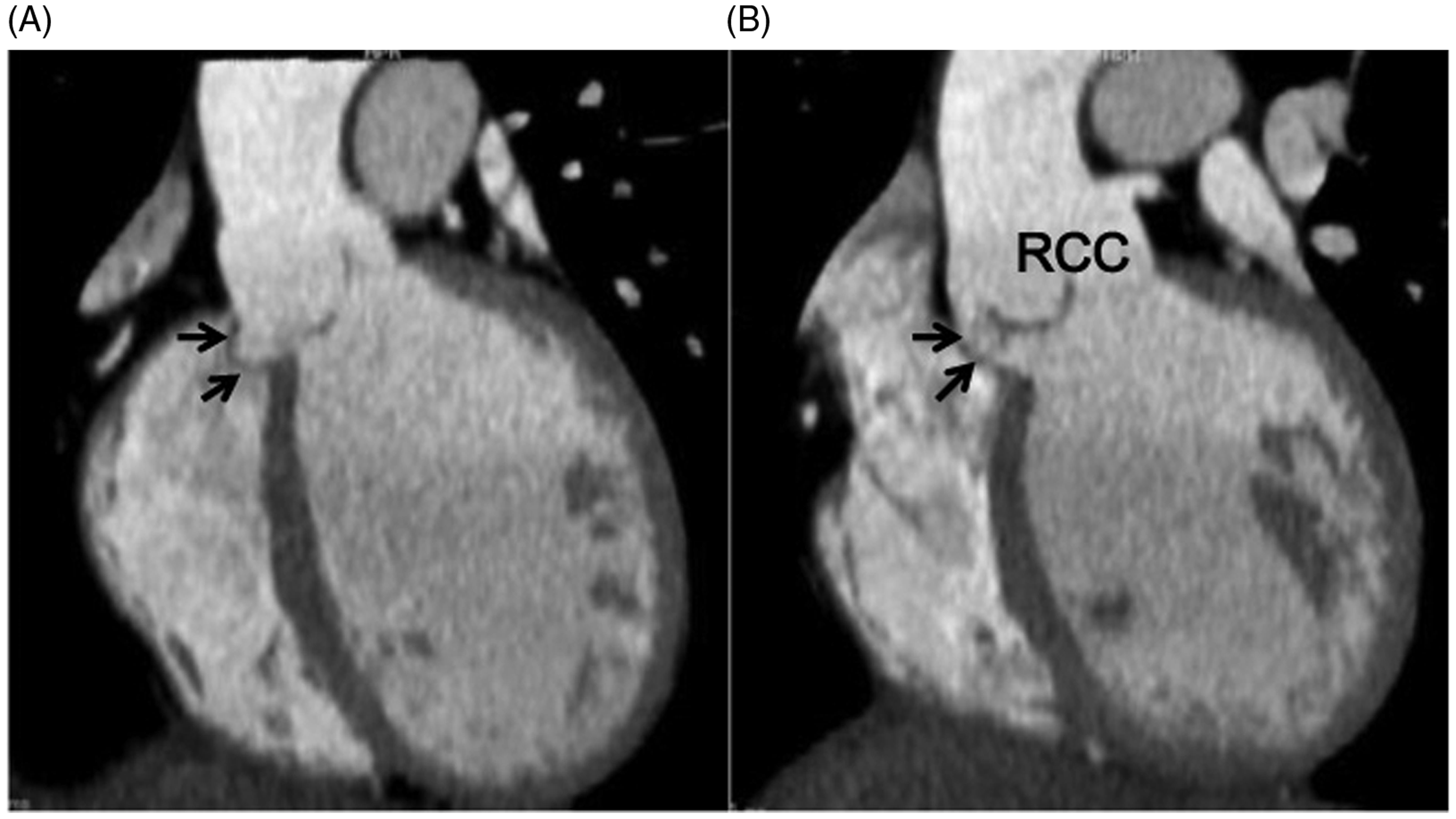
Discussion
ALVT is a rare congenital abnormal communication between the ascending aorta and the left ventricle, first reported by Levy and colleagues 1 in 1963. Up to 130 cases have been reported to date; the incidence of this defect is estimated to be 0.11% of congenital heart diseases. 2,3 On the basis of anatomic characteristics, Hovaguimian and colleagues 3 proposed a classification. Both case 1 and case 2 were type III (intracardiac aneurysm of the septal portion of the tunnel with or without right ventricular obstruction).
ALVT is usually diagnosed in early infancy due to heart murmur and the symptom of heart failure from AR, although some patients are diagnosed later, such as case 2. A significant amount of AR in infants should be suspected as ALVT, sometimes misdiagnosed as ventricular septal defect with AR. This defect can be diagnosed by transthoracic, transesophageal, and fetal echocardiography, magnetic resonance imaging, and multislice computed tomography. 4,5 Preoperative investigation of the relationship between the tunnel opening and coronary orifices is important for the selection of an adequate operative strategy and to avoid compromising myocardial revascularization. In our cases, 3-dimensional multislice computed tomography was useful in determining the detailed morphology and relationship with surrounding tissues, especially the coronary orifice.
Techniques of surgical closure include combinations of direct suture or patch closure of the aortic opening of the tunnel, obliteration of the tunnel, and occlusion of the ventricular opening. These techniques should be selected according to the tunnel size, morphology, and relationship with surrounding tissues or organs. 6,7 Aortic regurgitation is a major late problem after surgical closure of ALVT. The incidence of AR after surgery ranges from 16%–60%, requiring valve replacement in up to half of reported cases. The cause of AR after surgical closure is considered to be the coexistence of aortic valve disease, dilatation of the aortic root and Valsalva sinuses, and distortion of the aortic cusps at surgery. 8 –10 Furthermore, deviation of the unsupported segment of the aortic annulus may be an important cause, as in one of our cases. These cases highlight that echocardiography, cardiac catheterization, and multislice computed tomography can identify the detailed morphology, relationship with surrounding tissues, and associated lesions in ALVT.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.