
Abstract
Bronchogenic cysts are embryological remnants occurring as developmental abnormalities of the primary foregut. The most common locations of these cysts are the mediastinum, lung parenchyma, and inferior pulmonary ligament. An intrapericardial location is an extremely rare finding. We describe the case of a 76-year-old man with aortic valve stenosis and coronary artery disease, in whom an intrapericardial bronchogenic cyst was found incidentally during the open heart procedure.
Introduction
Bronchogenic cysts are congenital lesions resulting from an abnormal budding of the ventral diverticulum of the foregut or the tracheobronchial tree during embryogenesis. They are usually located in the mediastinum (65%), lung parenchyma (27%), or inferior pulmonary ligament (8%). 1 In the literature, there are only a few reports of an intrapericardial or left ventricular location.
Case report
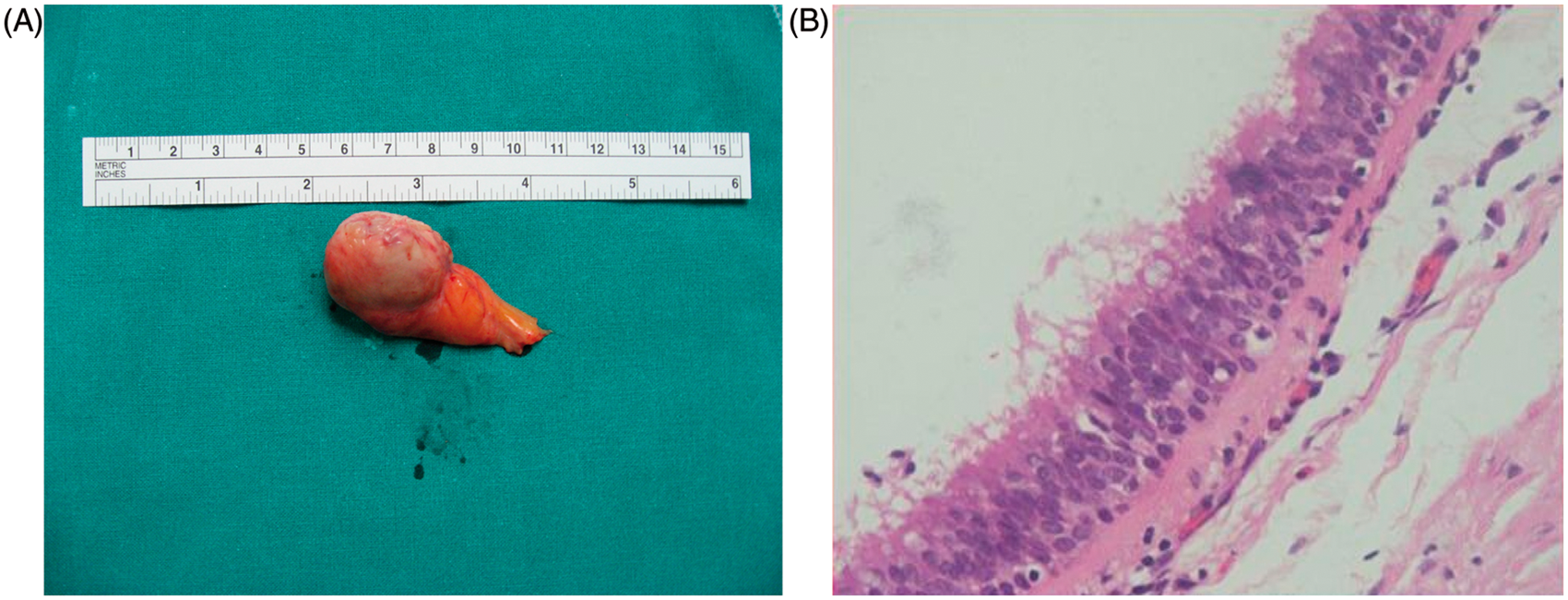
A 76-year-old man with severe aortic valve stenosis and 3-vessel coronary artery disease was referred to our hospital for aortic valve replacement and coronary artery bypass grafting. Preoperative transthoracic echocardiography revealed a calcified tricuspid aortic valve with severe stenosis (peak gradient, 125 mm Hg) and ventricular hypertrophy. A coronary angiogram showed significant stenosis in all major coronary branches. An intraoperative transesophageal echocardiogram revealed a round intrapericardial mass causing compression of the right atrium (Figure 1(a)). After pericardiotomy, a pedicled mobile cystic mass (30 × 28 × 20 cm) was identified (Figures 1(b), 2(a)). The pedicle originated from the pericardium of the transverse sinus, and the mass lay anteriorly and to the right of the aorta, compressing the right atrial appendage. The content of the cyst had a mustard-like appearance. Histopathological studies confirmed a cyst lined by respiratory mucosa with cartilage and bone in the wall (Figure 2(b)). The cyst was completely resected, the aortic valve was replaced with a bioprosthesis, and triple-coronary artery bypass grafting was performed. The perioperative course was uneventful, and the patient was discharged on the 7th postoperative day.
(A) Transesophageal echocardiogram showing a round intrapericardial mass (white arrow), causing compression of the right atrium. (B) Cystic mass (white arrow) compressing the right atrium. (A) Macroscopic appearance of the cystic mass. (B) Photomicrograph showing the cystic wall lined by respiratory epithelium. Hematoxylin and eosin stain, original magnification ×400.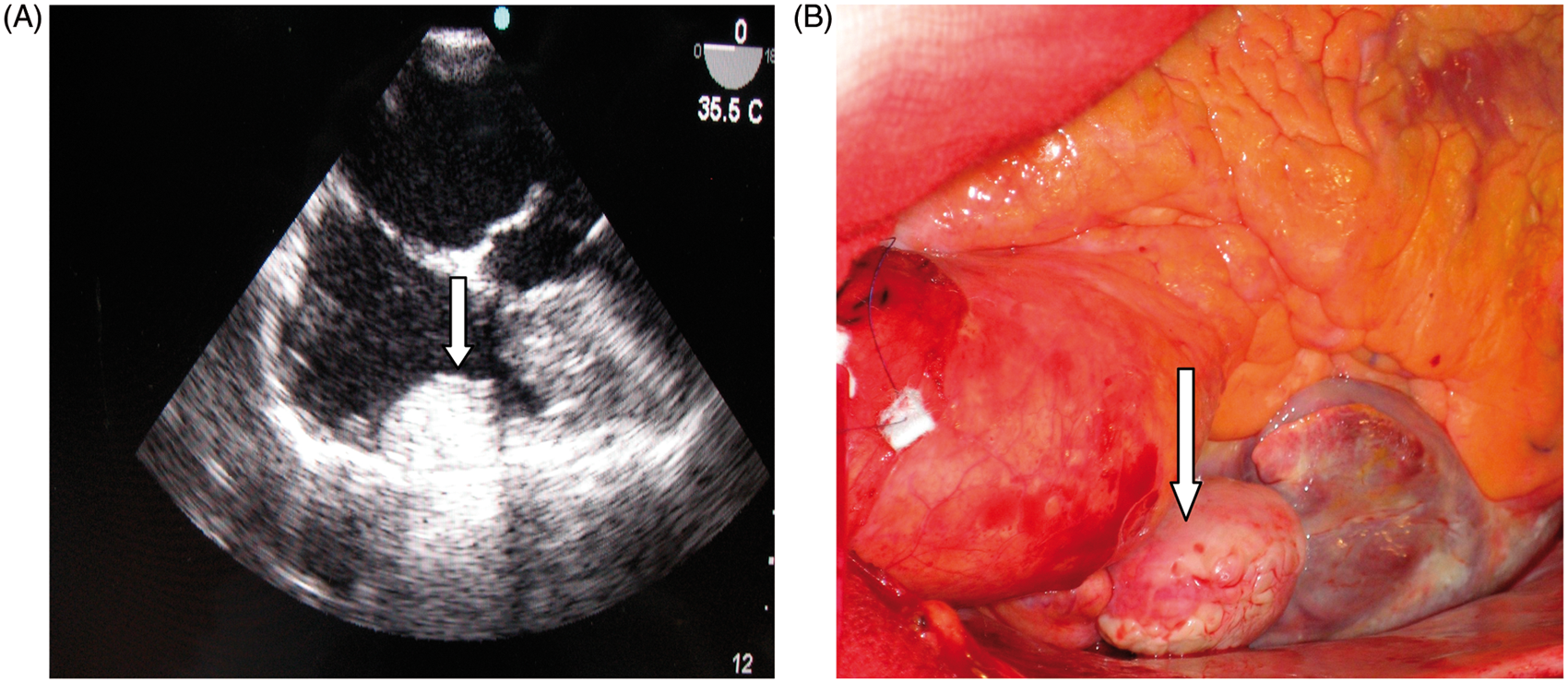
Discussion
Most bronchogenic cysts are found in the mediastinal, pericarinal, or paratracheal regions, intrapulmonary, along the esophagus, and below the diaphragm. 2 Rarely, they may also develop within the pericardium or the left ventricle. Bronchogenic cysts are usually lined by ciliated pseudostratified epithelium (characteristic of the respiratory tract). Occasionally, they may be lined by esophageal or gastric mucosa. Cartilage and smooth muscle may also be found in the walls.
The majority of these cysts remain asymptomatic. However, depending on the size of the cyst and possible compression of adjacent cardiac structures, symptoms such as chest pain, cough, dyspnea or acute respiratory distress, atrial fibrillation, superior vena caval obstruction, or spontaneous pneumopericardium have been reported. 3 – 5 The differential diagnosis must include cardiac tumors such as myxomas and teratomas, metastatic tumors, Morgagni diaphragmatic hernias, and thymic carcinomas. In our case, the existence of a pedicle meant that the cyst easily fitted between the cardiac structures, and this together with the rare incidence of such findings explains why it was not identified by transthoracic echocardiogram preoperatively.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.