
Abstract
Keywords
Introduction
Temporary vascular access for hemodialysis invariably requires the placement of a central venous catheter. The prevalence of venous stenosis or thrombosis after hemodialysis catheter use ranges from 10% to 50%. 1 Both direct trauma from the large-diameter catheters and intravascular turbulence during dialysis appear significant in the etiology of central vein stenosis (CVS). 2 The likelihood of developing CVS has been shown to be proportional to the number and duration of central vein catheters and the number of catheter-related infections. 3 In addition, cannulation of a subclavian vein or the left internal jugular vein has been associated with an increased risk of CVS. 4,5 While CVS is often asymptomatic in non-dialysis patients, occlusion of a major thoracic vein may produce facial swelling or unilateral upper limb edema ipsilateral to an arteriovenous fistula (AVF). More than half of those with catheter-related CVS may experience symptomatic resolution upon removal of the device, with or without anticoagulant therapy, obviating the need for invasive treatment. 6 Nonetheless, after catheter removal, 28% of all patients have radiological evidence of CVS persisting beyond 3 months. 3 In symptomatically refractory cases, intervention is required. Percutaneous transluminal angioplasty with or without stenting is now accepted as the initial intervention for patients with CVS of benign etiology, including those undergoing hemodialysis. 7 Restenosis, however, is common and multiple interventions are to be expected. 8,9 This study aimed to identify factors that contribute to CVS risk within the hemodialysis population of the National University Hospital, Singapore. We hypothesized that central vein catheterization and surgically-created hemodialysis access are significant in the etiology of CVS. We also aimed to identify the outcome of interventions directed at CVS in our patients.
Patients and methods
Clinical characteristics of patients with and without central vein stenosis.
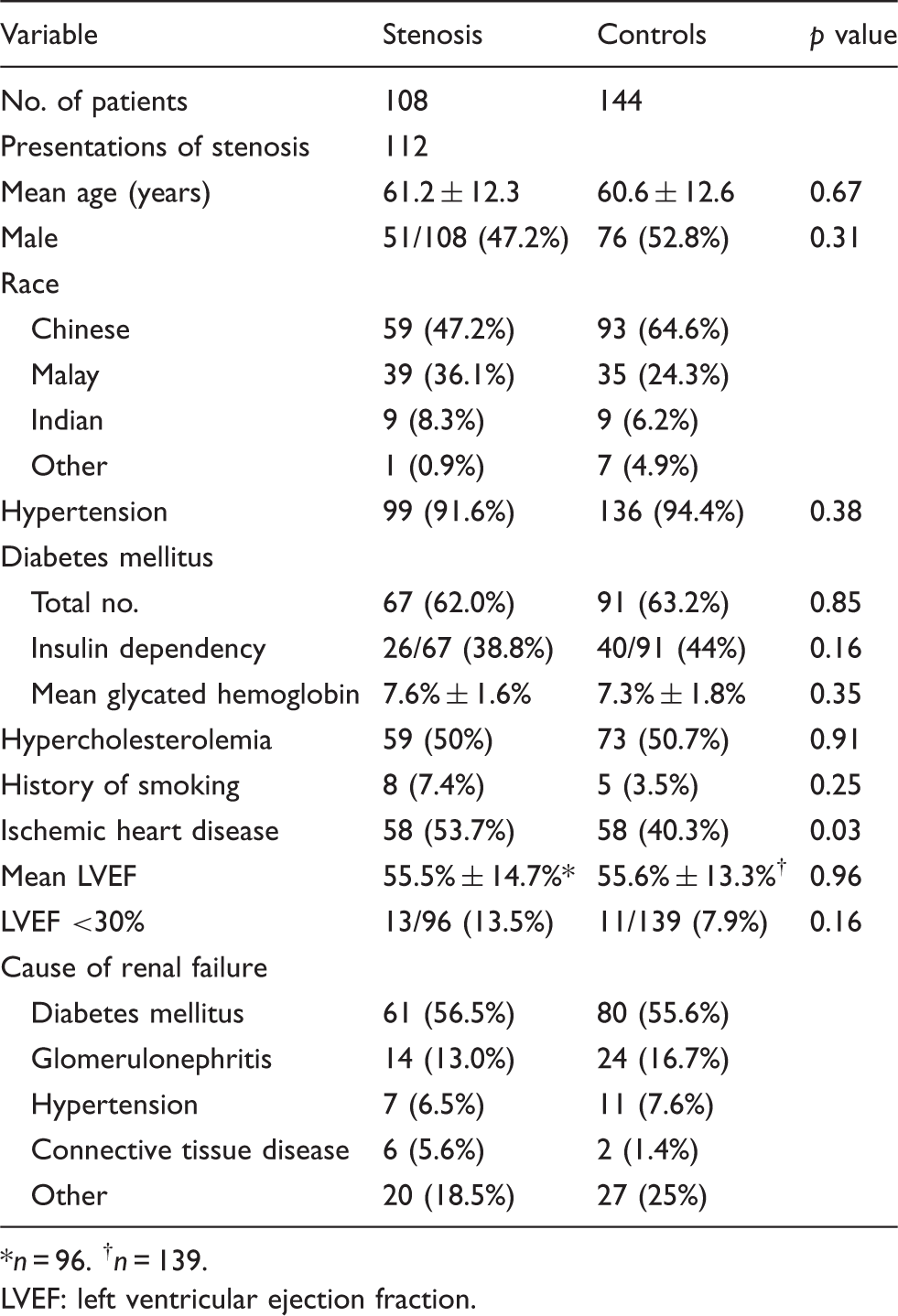
n = 96. † n = 139.
LVEF: left ventricular ejection fraction.
With regard to hemodialysis, we analyzed the following variables: the duration of RRT, the number and side of permanent hemodialysis catheters (PHC) inserted, history of PHC sepsis, the time between commencement of RRT and surgical access creation, the number and side of access operations prior to the diagnosis of CVS, and peritoneal dialysis catheter use. The exact duration of PHC use was not available for most patients. PHC were preferentially placed in the right internal jugular vein (IJV). The left IJV was used if the right IJV or right brachiocephalic vein (BCV) was severely stenosed or occluded, if a right-sided PHC was removed due to sepsis, or if an AVF was to be created in the right arm. A subclavian vein was used if no IJV was available. AVF were preferentially created on the non-dominant arm.
CVS was diagnosed by magnetic resonance venography or conventional venography. Data were compiled from contemporaneous reports by consultant radiologists. In the group of patients who underwent central vein angioplasty, we analyzed the type of intervention, the patency after intervention, and the requirement for further procedures. Balloon angioplasty was performed under systemic anticoagulation. The criterion for technically successful angioplasty was less than 30% residual stenosis. A S.M.A.R.T. nitinol stent (Cordis Corp) was placed if more than 30% residual stenosis was present. Stent size was determined by the diameter of the adjacent normal vein and the length of the stenosis. Failures were defined as lesions that could not be crossed with a guidewire. Stent patency was determined clinically. Venography was only performed when clinical manifestations of CVS (including failing AVF) became evident. Primary patency was defined as the length of time from angioplasty until reintervention, restenosis, or the time of measurement of patency.
Measured values are reported as percentages, mean ± one standard deviation, or median and interquartile range (IQR; 25th to 75th quartile). Differences between groups were compared by the chi-squared or Fisher’s exact tests for categoric variables, Student’s t test for continuous parametric variables, and the Wilcoxon test for nonparametric continuous variables. Logistic regression was used to examine the influence of interventions to establish hemodialysis access on the development of left and right BCV stenosis against the control population. Primary patency after central venoplasty was analyzed by the Kaplan-Meier method. Statistical analysis was performed using NCSS software (Kaysville, Utah, USA). 10 A value of p < 0.05 was considered significant.
Results
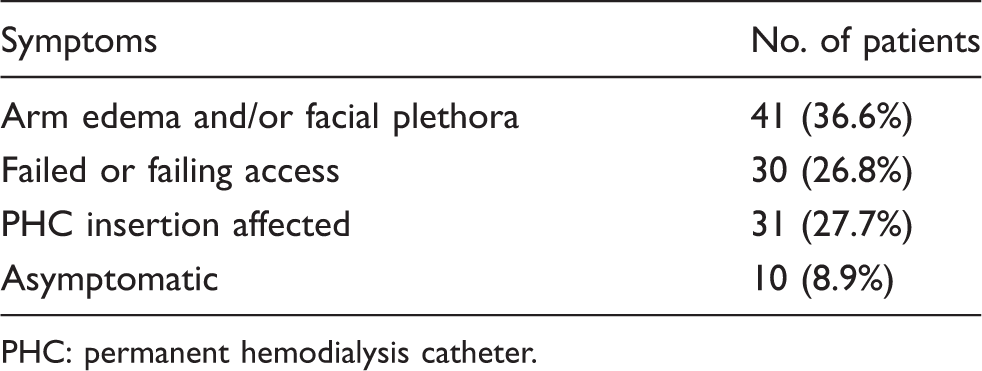
The most common clinical finding was swelling of an upper limb in which an AVF was present (n = 36). Facial plethora appeared concurrently in 5 patients, while it was the only presenting symptom in a further 5. Ten patients were asymptomatic at the time of diagnosis; in 9, CVS was revealed on imaging while planning AVF surgery, and one had CVS discovered on a computed tomography pulmonary angiogram (Table 2). One hundred and ninety-four venous stenoses were identified in 108 patients (Figure 1). The right BCV was the most commonly affected central vein, constituting 35.1% of all stenoses, followed in frequency by the left BCV (28.3%). At presentation, 60 patients also had a stenosis of at least one IJV.
Distribution of central vein stenosis: diagram of the central thoracic veins, demonstrating the distribution of 194 venous stenoses identified on imaging. Presentation of central vein stenosis in 112 patients. PHC: permanent hemodialysis catheter.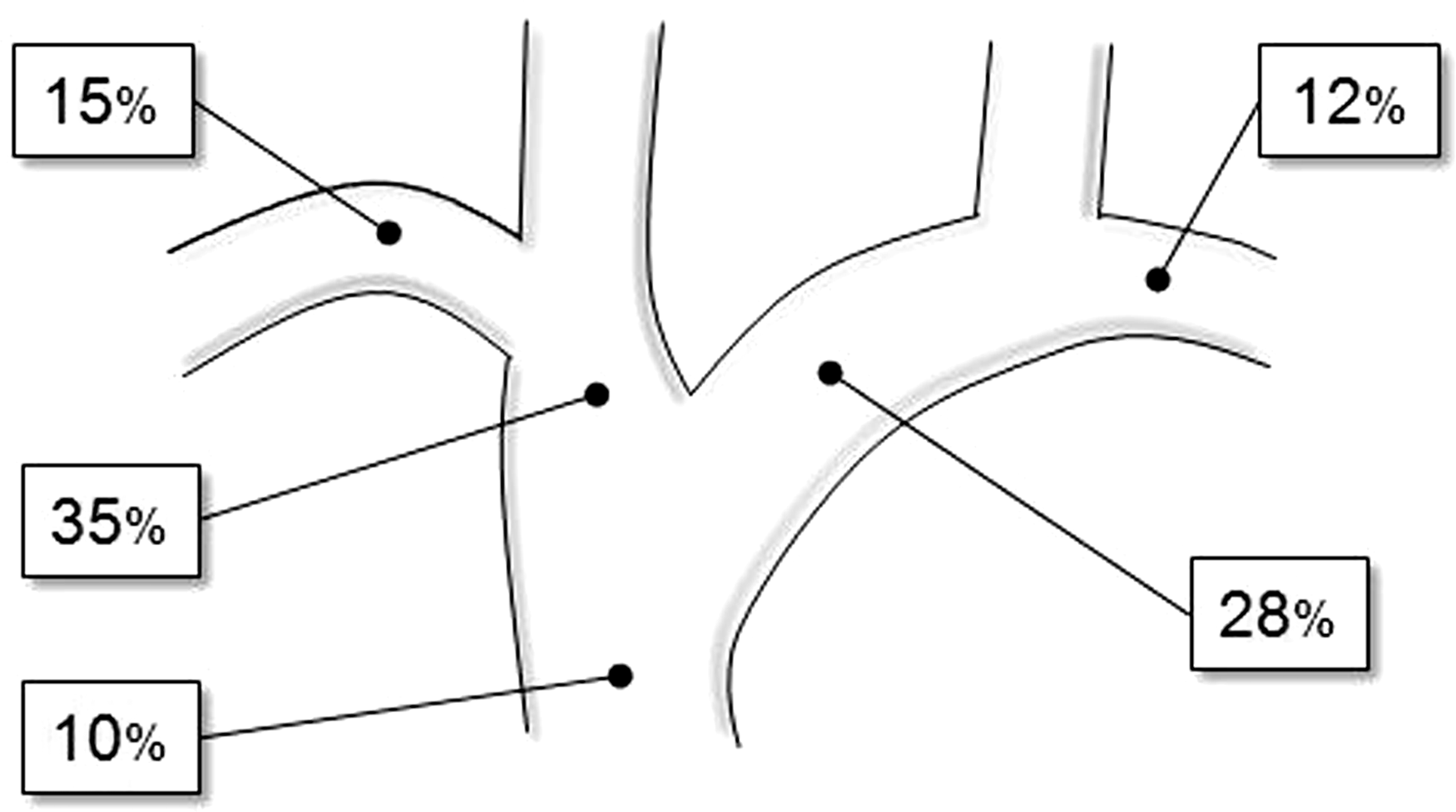
Prior dialysis access in patients with and without central vein stenosis.
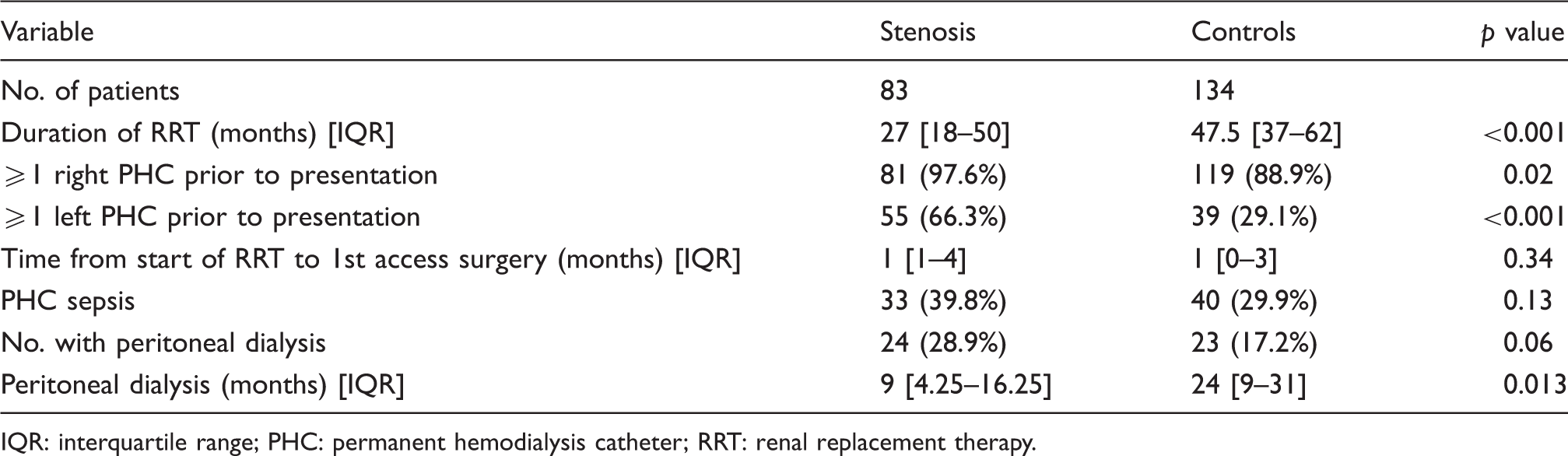
IQR: interquartile range; PHC: permanent hemodialysis catheter; RRT: renal replacement therapy.
Sixty-two patients had at least one moderate-to-severe BCV stenosis or occlusion. Sixteen patients had bilateral BCV stenoses, 13 of which were identified concurrently. The median duration of RRT was shorter in the BCV stenosis group than the control group (p < 0.001). Right- and left-sided PHC placement was more frequent in those who subsequently developed BCV stenosis than in controls (p < 0.001 for each), as was the frequency of surgery to create right and left arm AVF (p = 0.043 and p < 0.001, respectively; Figure 2). Despite the shorter duration of RRT, left-sided PHC insertion was significantly more common among the left BCV stenosis group (30/37 patients, 81.1%) than controls (39/134 patients, 29.1%). In only 2 cases was BCV stenosis not preceded by ipsilateral central vein instrumentation or AVF creation. Compared to controls, right BCV stenosis was associated with higher frequencies of left PHC insertion: hazard ratio (HR) 4.7, 95% confidence interval (95%CI) 1.3–16.4; and left AVF creation: HR 4.0, 95%CI 1.3–12.4; but not right AVF creation (HR 2.0, 95%CI 0.46–8.5) and right PHC insertion (HR 1.9, 95%CI 0.9–4.1). Left BCV stenosis was strongly associated with left-sided PHC insertion (HR 58.4, 95%CI 9.2–372) but no other factor reached statistical significance.
Frequency of interventions to establish hemodialysis access in 62 patients with central vein stenosis (CVS) and 134 controls. Median frequency of permanent hemodialysis catheter (PHC) insertions (top row) and arteriovenous fistula (AVF) operations (bottom row) in patients who subsequently developed brachiocephalic vein stenosis (dark bar) and controls (light bar), with interquartile range (IQR; line).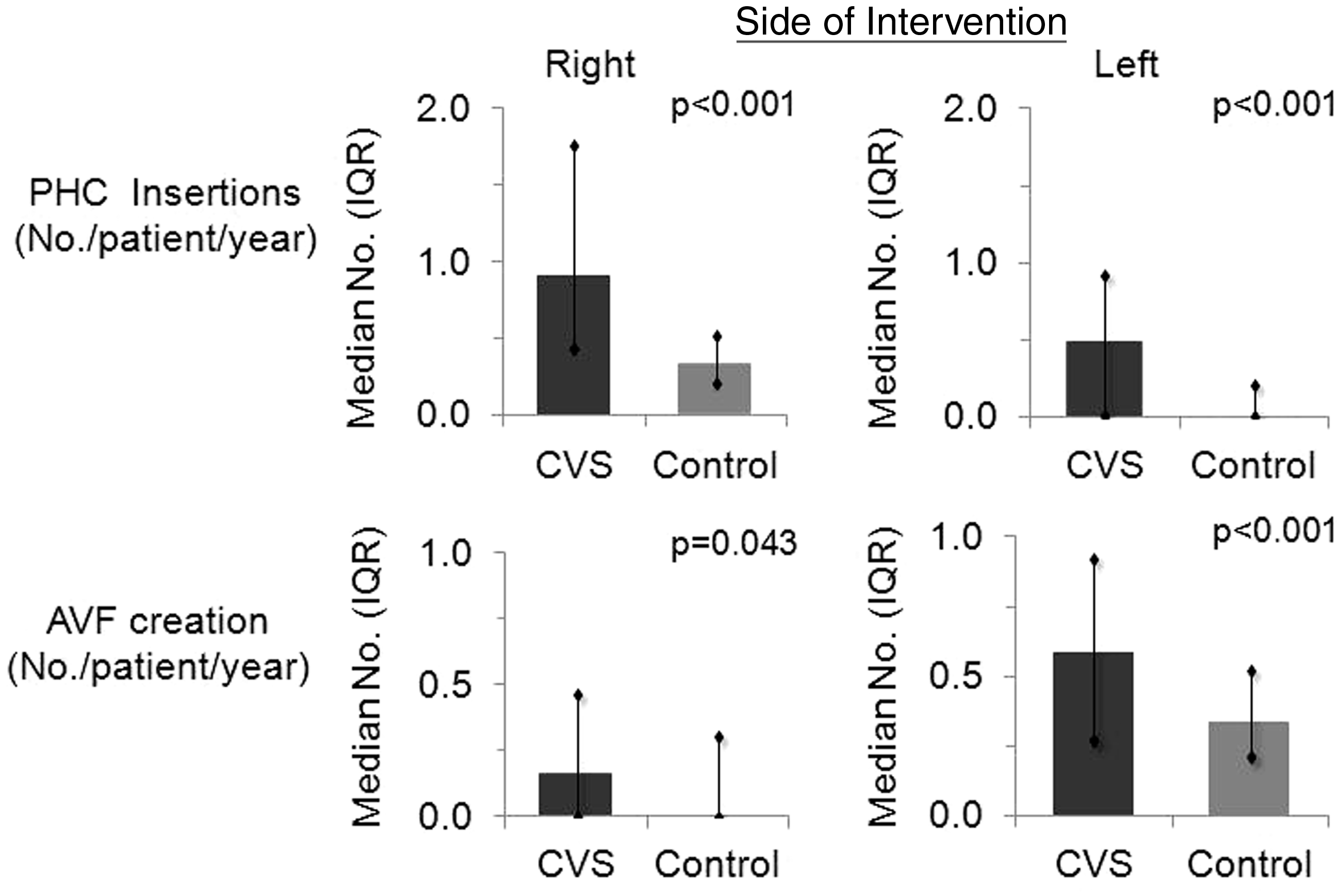
There were 53 interventions in total. There were 44 successful angioplasties; in 22 (50%) of these, a Smart stent was placed. There were 9 procedural failures. After successful angioplasty, an AVF on the upper limb of the affected side was functional in 14/44 (31.8%) cases, whereas in the failed angioplasty group (n = 9), only one patient who initially presented with a failing access continued to use the affected AVF. There were 23 reinterventions in 15 patients. The median intervention-free patency was 14 months (Figure 3).
Kaplan-Meier analysis of intervention-free patency of central venous stenosis angioplasties.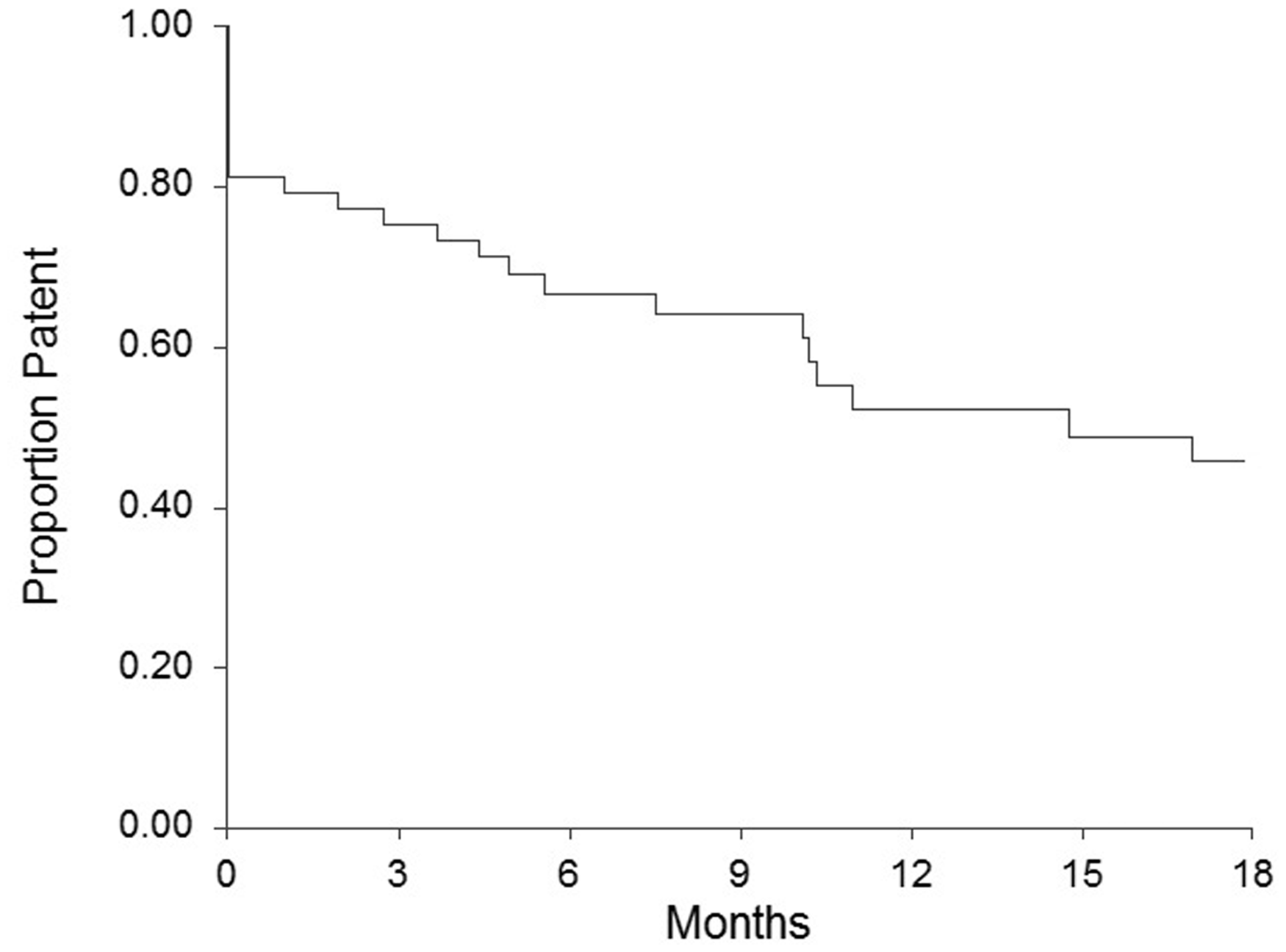
Discussion
Complications of vascular access, including infection, hospitalization, and death, are more prevalent among those who are dialyzed by central venous catheter than by other means. 7,11 Several studies have associated stenosis of the central thoracic veins with dialysis by PHC. The risk of CVS has been shown to relate to the number of catheters, the site of insertion and the duration of dialysis by PHC. 3,5 Within our cohort, the rate of PHC insertion was significantly higher among those who developed CVS than in controls. AVF surgery was also more frequent in the CVS group. Unfortunately, we do not have accurate data on the length of time that a central vein was exposed to a PHC or a functioning fistula (our hospital records indicate that 30%–40% of AVF failed to mature). However, one may hypothesize that the duration of PHC use will rise in proportion to the total number of hemodialysis access procedures, especially as a maturing or failed AVF necessitates alternative access for RRT. Thus, the combined rate of procedures to establish dialysis by PHC and AVF may be viewed as a surrogate for the duration of central vein catheterization.
To further delineate the effect of hemodialysis interventions on the development of CVS, we analyzed factors that may contribute to the development of BCV stenosis, as both IJV and subclavian vein catheters pass through the brachiocephalic veins. As a reflection of our access algorithm, PHC were inserted more commonly on the right side than the left. It is notable that only 29% of those without CVS had a history of left-sided PHC placement. That left PHC placement was associated with the development of both left and right BCV stenosis is indicative of our practice of reserving left-sided catheters for occasions when right PHC insertion was not desirable or technically possible.
Many studies have demonstrated the relevance of PHC location to central vein stenosis. Salgado and colleagues 5 analyzed the outcomes of 479 IJV catheterizations and found a higher prevalence of CVS after left-sided catheter placement. It has been postulated that this is possibly as a result of the more tortuous route of a left-sided catheter, the length of vein that the catheter traverses, and the degree of catheter movement with head rotation. 12 The role of prior contralateral catheterization cannot be discounted. In Salgado’s study and in our cohort, those with a left-sided PHC were more likely to have had a contralateral catheter than those with a right IJV catheter.
Despite the well-documented morbidity associated with dialysis by PHC, 77% of patients who presented for initial AVF construction during the period of this study had already commenced hemodialysis via a central venous catheter (unpublished data). This is significantly higher than that recommended by international guidelines. 7 The reasons behind the low rate of preemptive AVF formation within our pre-dialysis population have yet to be elucidated. However, it is important that the barriers to timely AVF construction are identified if we are to reduce the prevalence of dialysis by PHC.
Percutaneous transluminal balloon angioplasty is the first-line management for patients with CVS. 7,9,13,14 The propensity of CVS to recur after endovascular therapy has been well documented, and multiple interventions are often required. 8,14,15 For lesions that do not respond to angioplasty or recur quickly, stent placement is indicated. 8,14 We employed a policy of selective stenting after angioplasty. Twenty-two of 44 (50%) patients required a stent at the time of balloon angioplasty. The primary patency was 52% at one year, a rate comparable to those of other studies, where 12-month primary patencies of 11%–71% have been achieved. 16
This observational study has several limitations. Firstly, cases were only included if they were symptomatic or had CVS diagnosed incidentally, and follow-up imaging after central vein angioplasty was reserved for those with recurrent symptoms. Consequently, a number of asymptomatic cases may have been missed. The demographic data also contained some deficiencies. While more than 90% of patients had been diagnosed with hypertension, the degree of blood pressure control was not recorded. Our findings would have been strengthened by data on the exact length of time central veins were exposed to catheters and flow from functioning fistulas. This was difficult to obtain because most patients attended independently run satellite centers for dialysis. However, criteria for the selection of controls ensured that the chance of bias from a comparatively shorter duration of RRT was eliminated. It was concluded that multiple access interventions, associated with prolonged residency of PHC, are significant in the etiology of CVS. While endovascular intervention is largely successful in treating CVS, a program aimed at timely AVF construction should significantly reduce the morbidity associated with prolonged dialysis by central venous catheter.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.
Presented at the 11th Annual Congress of the Asian Society for Vascular Surgery, Kyoto, Japan, 29 June–2 July 2010.