
Abstract
We describe a case of bronchial artery aneurysm presenting as a solitary lung mass (4 × 5 cm) in a 53-year-old man with symptoms of cough for 3 months. The aneurysm was only detected at surgery, and resected by performing a middle lobectomy.
Introduction
Bronchial artery aneurysm (BAA) is a rare vascular abnormality. Although it can be asymptomatic, it often presents first as hemoptysis, hematemesis, or shock secondary to hemothorax. 1 The majority present as an extrapulmonary mediastinal mass. 2 We describe a rare presentation of BAA as a solitary intraparenchymal lung mass.
Case report
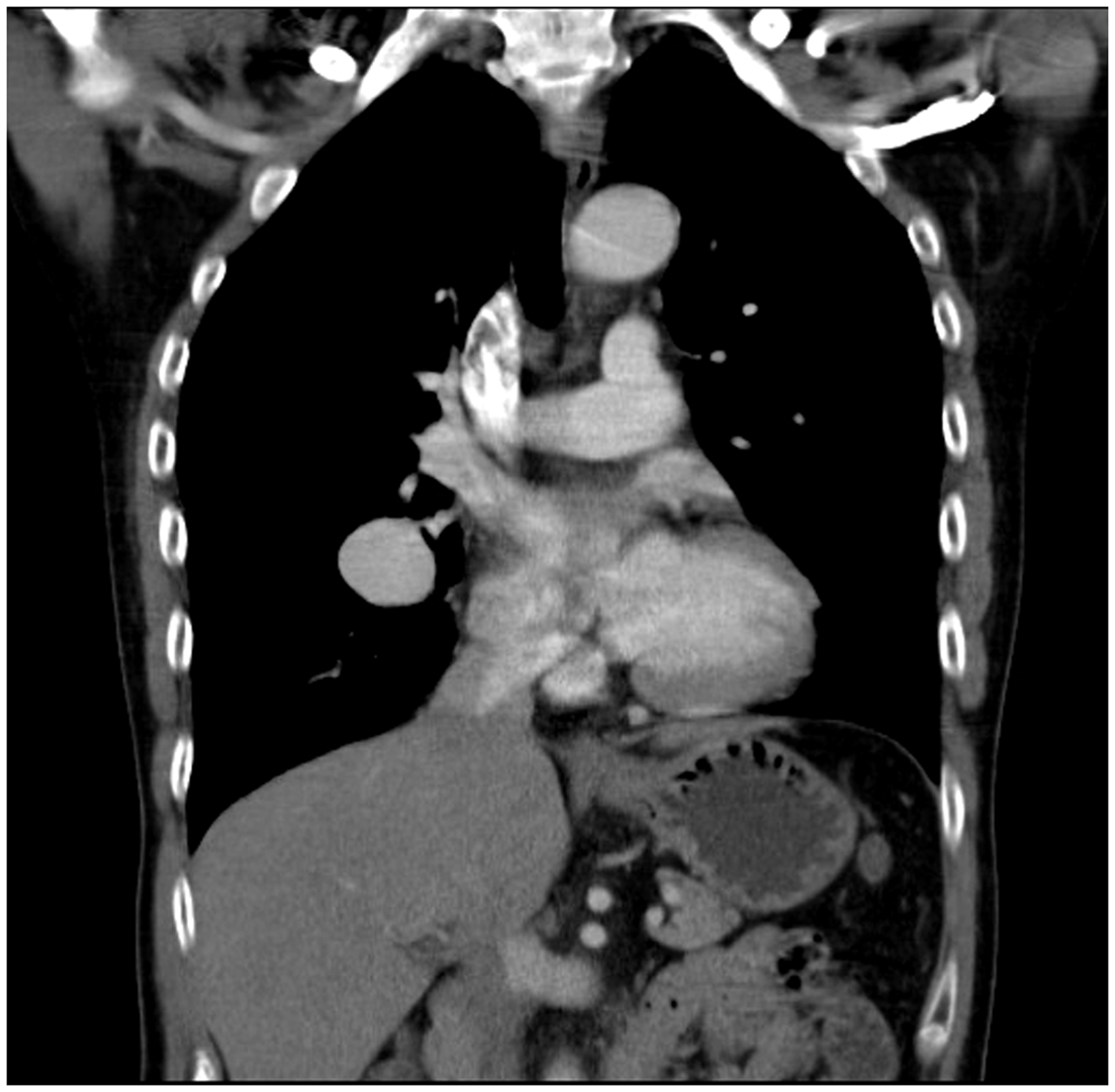
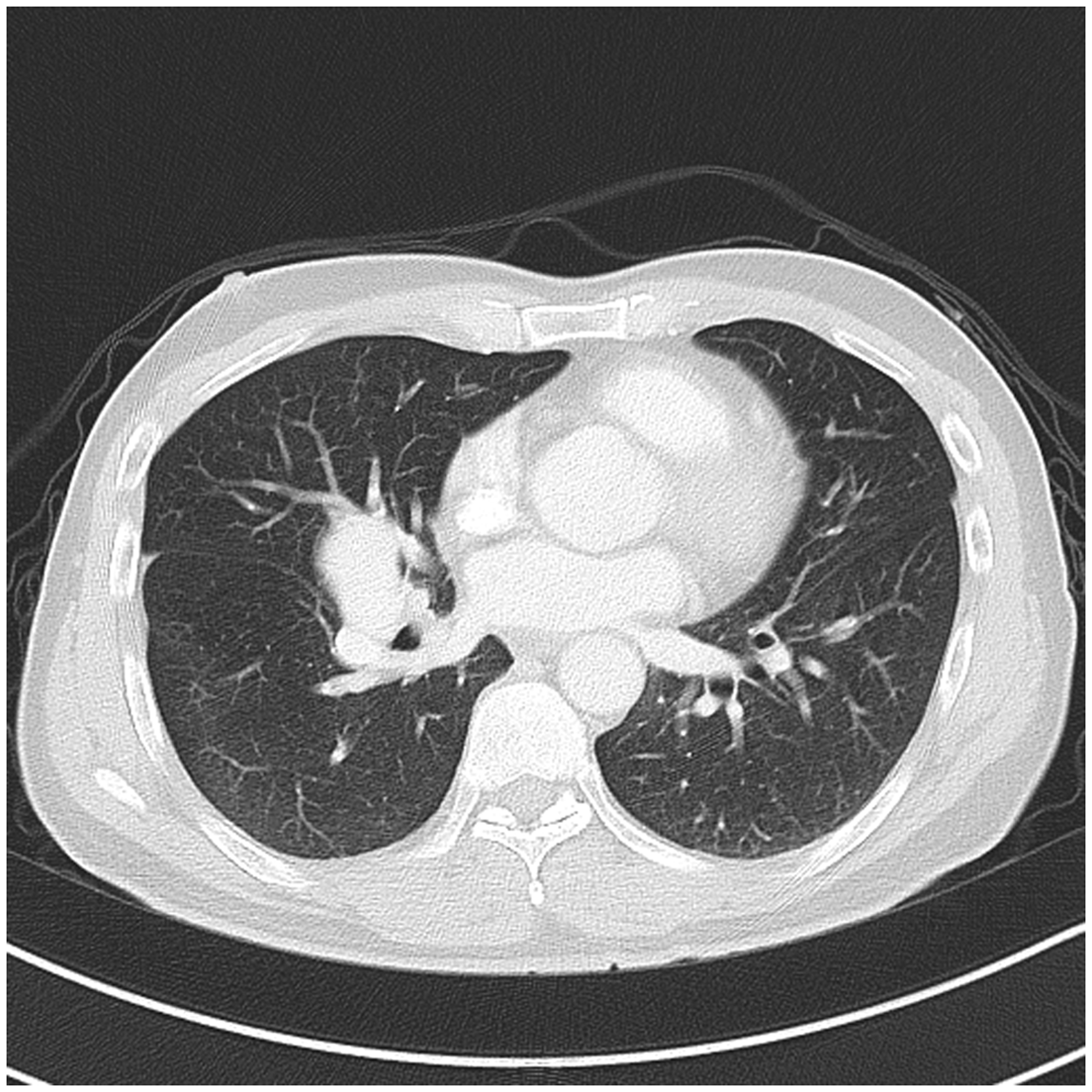
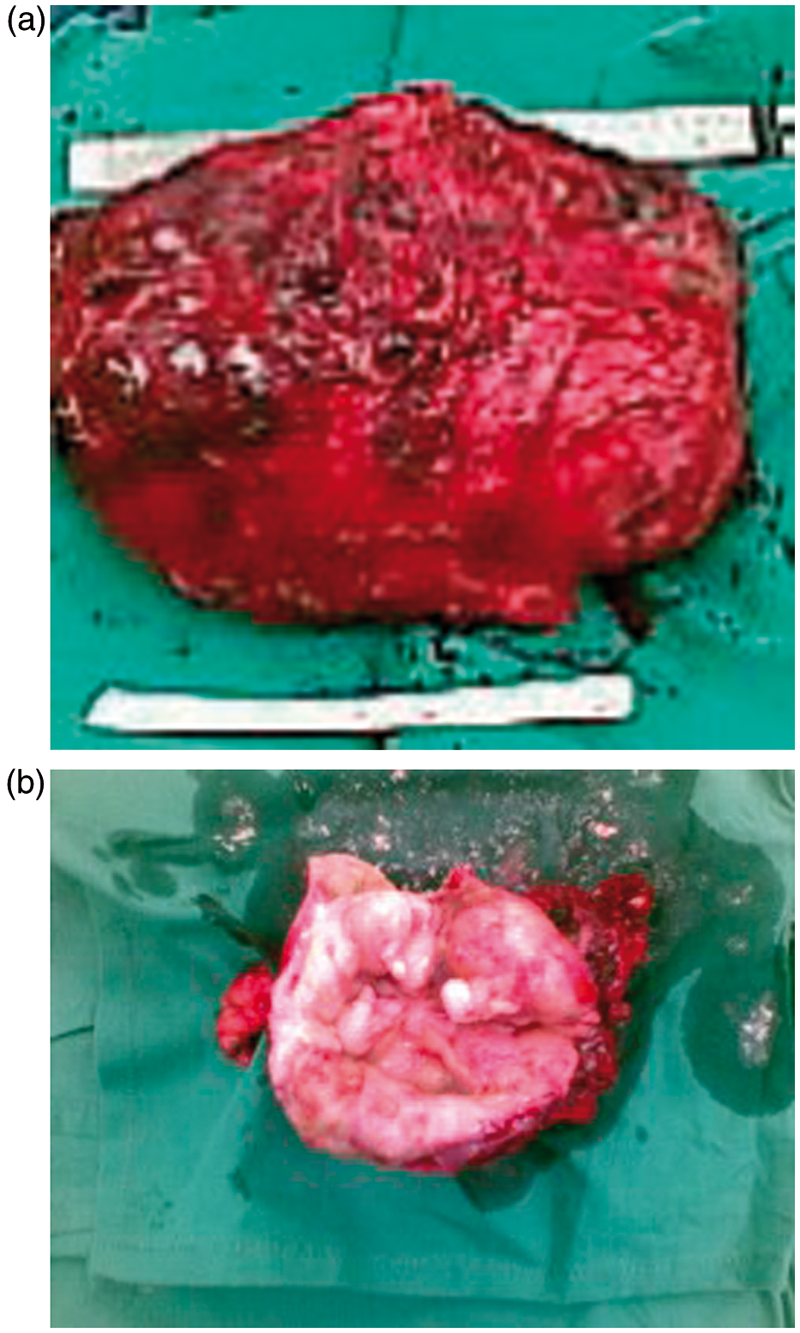
A 53-year-old man, a nonsmoker with no previous medical history, presented with a 3-month history of nonproductive cough. There was no associated chest pain or hemoptysis. There were no systemic signs such as weight loss or fever. Chest radiography showed a round well-encapsulated right lung lesion (Figure 1). Computed tomography of the thorax demonstrated a smooth enhancing 4.2 × 2.9 × 3.3-cm lesion in the hilum of the lateral segment of the middle lobe, suggestive of a neoplastic process (Figure 2). The rest of the middle lobe and lung parenchyma were normal. No lymphadenopathy was seen. Although some enlarged vessels were noted in the subcarinal space, they were not seen coursing into the mass (Figure 3). The patient underwent elective video-assisted thoracoscopic surgery. Intraoperatively, a 4 × 3-cm middle lobe mass was found with a hypertrophied bronchial artery (1.5 cm) supplying the middle lobe. Inadvertent rupture of the aneurysm occurred during manipulation of the middle lobe. Conversion to an open thoracotomy was carried out to ligate the feeding bronchial vessel in the subcarinal area, followed by a middle lobectomy. This was possible because the aneurysm was partially thrombosed and the bleeding was not as severe as it might otherwise have been. The patient’s postoperative recovery was uneventful. Histology showed a large true aneurysm in the middle lobe, measuring 3 × 3 × 2.5 cm with a thin 1-mm fibrous wall with a smooth inner surface and areas of intimal thickening, myxoid degeneration, and focal wall lipid deposits. The rest of the middle lobe was essentially normal, showing mild dilation of the airspaces (Figure 4).
Preoperative chest radiograph showing the right middle lesion. Chest computed tomography in coronal view, showing a 4.2 × 2.9 × 3.3-cm lobulated enhancing mass in the central aspect of the middle lobe lateral segment. Transverse section of the computed tomography scan of the chest, showing the right middle lobe lesion with a hypertrophied aneurysmal vessel. (a) The bronchial artery aneurysm specimen. (b) Cut section of the specimen.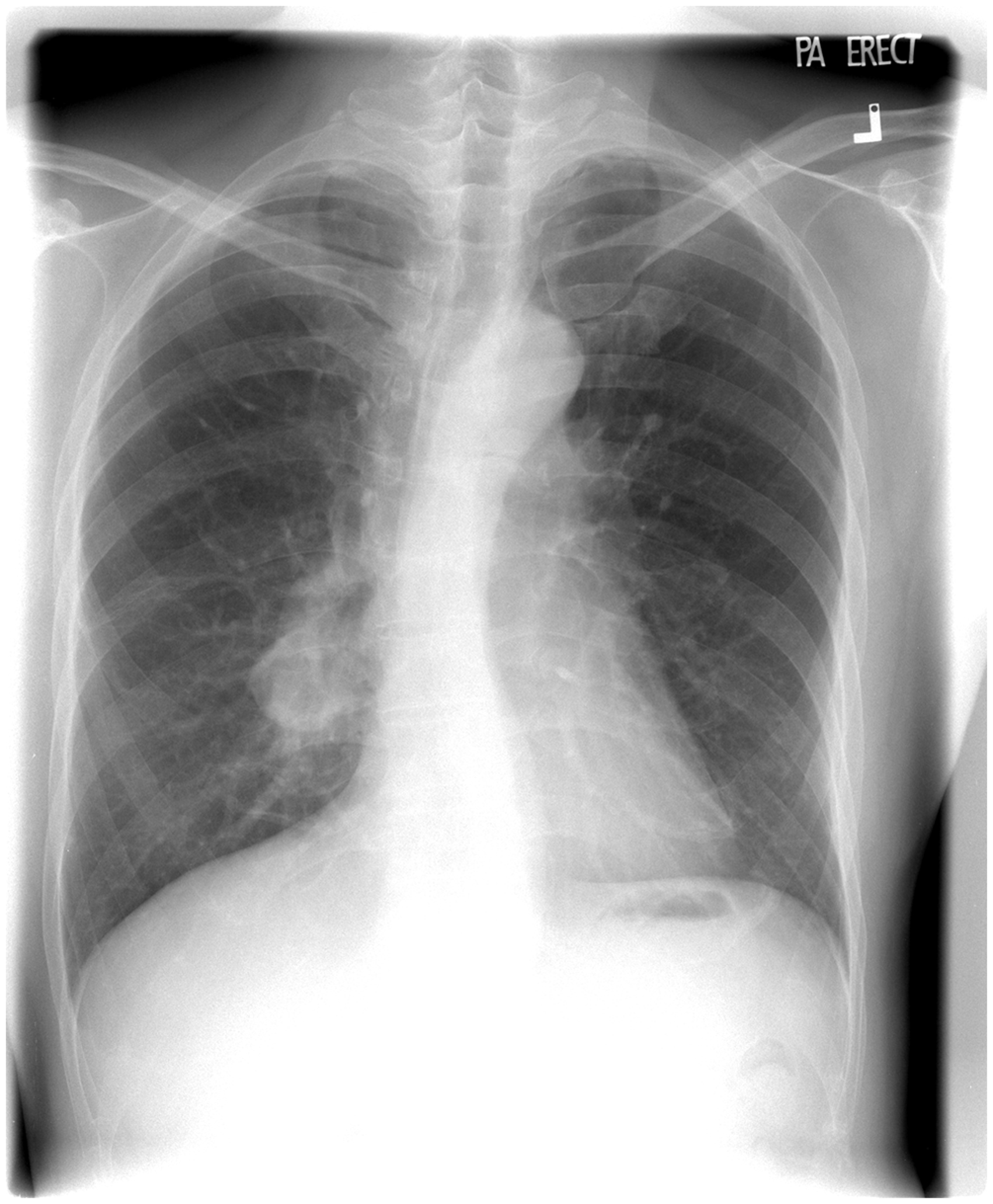
Discussion
The first case of BAA was described in 1930 in a patient with syphilis, and since then, approximately 50 cases have been reported. 3 Although its true incidence is unknown, it can be seen in up to 1% of bronchial artery angiograms. 4 BAA is a rare true aneurysm involving the entire wall of the bronchial artery. Most are located in the mediastinum in the vicinity of the aorta and esophagus where the bronchial arteries arise from the aorta. Here the vessel tend to be larger in its extraparenchymal course, and subjected to higher systemic arterial pressures. Aneurysm of the intraparenchymal course of bronchial vessels is very rare because the vessels tend to be smaller, with the walls buttressed by the surrounding lung parenchyma. Although bronchial arteries are small to medium systemic vessels, large giant asymptomatic BAA can arise from them, as in our case. Most present after rupture but some present pre-rupture with symptoms of compression, such as chest or back pain mimicking aortic dissection, or superior vena caval obstruction. 5,6 Because most are located in the mediastinum, when they rupture they present as shock secondary to hemorrhage. Rarely, they are intraparenchymal where they can be either asymptomatic (detected on chest radiography) or present as hemoptysis or hematemesis if they erode into the bronchus or esophagus. 7 When the aneurysm is thrombosed, it will not enhance with intravenous contrast medium on computed tomography, thus simulating a benign lung or esophageal tumor. 8
BAA are true aneurysms and are usually due to underlying chronic inflammatory lung conditions such as tuberculosis, sarcoidosis, or bronchiectasis, where there is inflammatory injury to the walls of hypertrophied bronchial arteries. 9 Arthrosclerotic change is another commonly cited etiology because pathological studies of excised aneurysmal sacs show degenerative atherosclerotic changes. Other rarer etiologies include congenital pulmonary artery agenesis, mycotic and hereditary hemorrhagic telangiectasia. 10,11 Although our patient had no underlying chronic inflammatory lung disease, atherosclerosis might be a possible etiology due to the histological findings in the aneurysmal wall. The risk of rupture of BAA is independent of the size and diameter of the lesion. As the risk of fatal catastrophic hemorrhage with rupture is high, all patients should be treated early with radiological transcatheter arterial embolization, irrespective of symptoms, with good results. 12 Urgent embolization, after initial hemodynamic stabilization and insertion of a chest tube, is also the treatment of choice in an emergency setting. 13 Transcatheter embolization can successfully obliterate the blood flow and excluded the aneurysm if the segment between the aneurysm and aorta is judged sufficiently long on bronchial arteriography. For an aneurysm arising close to origin of aorta, successful occlusion has been achieved by endovascular deployment of covered stents into the aorta. 14 Surgery should be reserved for cases in which embolization fails or the spinal medullary artery arises from the aneurysmal bronchial vessels. Embolization in the latter case would risk spinal cord ischemia. The operation can be performed by video-assisted thoracoscopic surgery or thoracotomy, with early proximal ligation of the feeding vessels to avoid inadvertent rupture of the aneurysm during mobilization. Surgery for intraparenchymal BAA, in addition to ligation of proximal vessels, should include resection by lobectomy or segmentectomy, depending on the size and site. This is because of the retrograde blood supply from intraparenchymal bronchopulmonary collaterals.
Although infection and neoplasm remain the main etiologies for solitary lung masses, it is important to keep in mind rare vascular causes such as BAA, especially when there is contrast enhancement, chronic inflammatory disease, or hypertrophied tortuous bronchial vessels on computed tomography. When clinically suspected, the patient should undergo an elective bronchial artery angiogram and embolization to prevent rupture and avoid emergency surgery.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.