
Abstract
A 1-month-old neonate was admitted in respiratory distress. Two-dimensional echocardiography and computed tomography scan showed a mass anterior to the left ventricle and right ventricular outflow tract. A biopsy revealed an inflammatory myofibroblastic tumor. A tuberculin test showed an 18-mm diameter induration. Three of the 6 household contacts were also positive for pulmonary tuberculosis. Antituberculosis medication was started. After 1 year, echocardiography and computed tomography scan showed complete resolution of the mass.
Introduction
Tuberculosis (TB) is at least as old as mankind. It is thought to be the oldest of human diseases, which has waxed and waned in its incidence, but has remained a perpetual threat from age zero to beyond. 1 More than 2 billion individuals worldwide are infected with the TB bacilli, with children <15-years old representing 9.6%–11% of all cases. 2 Congenital tuberculosis is diagnosed based on active tuberculosis in the mother, active tuberculosis in the neonate, and no source of tuberculosis other than the mother. Neonatal tuberculosis, however, does not demand these criteria, and infection may be acquired following exposure to Mycobacterium tuberculosis from a number of sources. Neonatal tuberculosis is relatively rare, with fewer than 200 cases reported in the English literature. 3 Inflammatory pseudotumor, originally identified in the lung, has been described in multiple extrapulmonary anatomic locations. It is a rare, mass-forming lesion, and a result of etiologically diverse processes. Infection-associated inflammatory pseudotumors are caused by a wide array of infectious agents, including Mycobacterium tuberculosis. 4
Case report
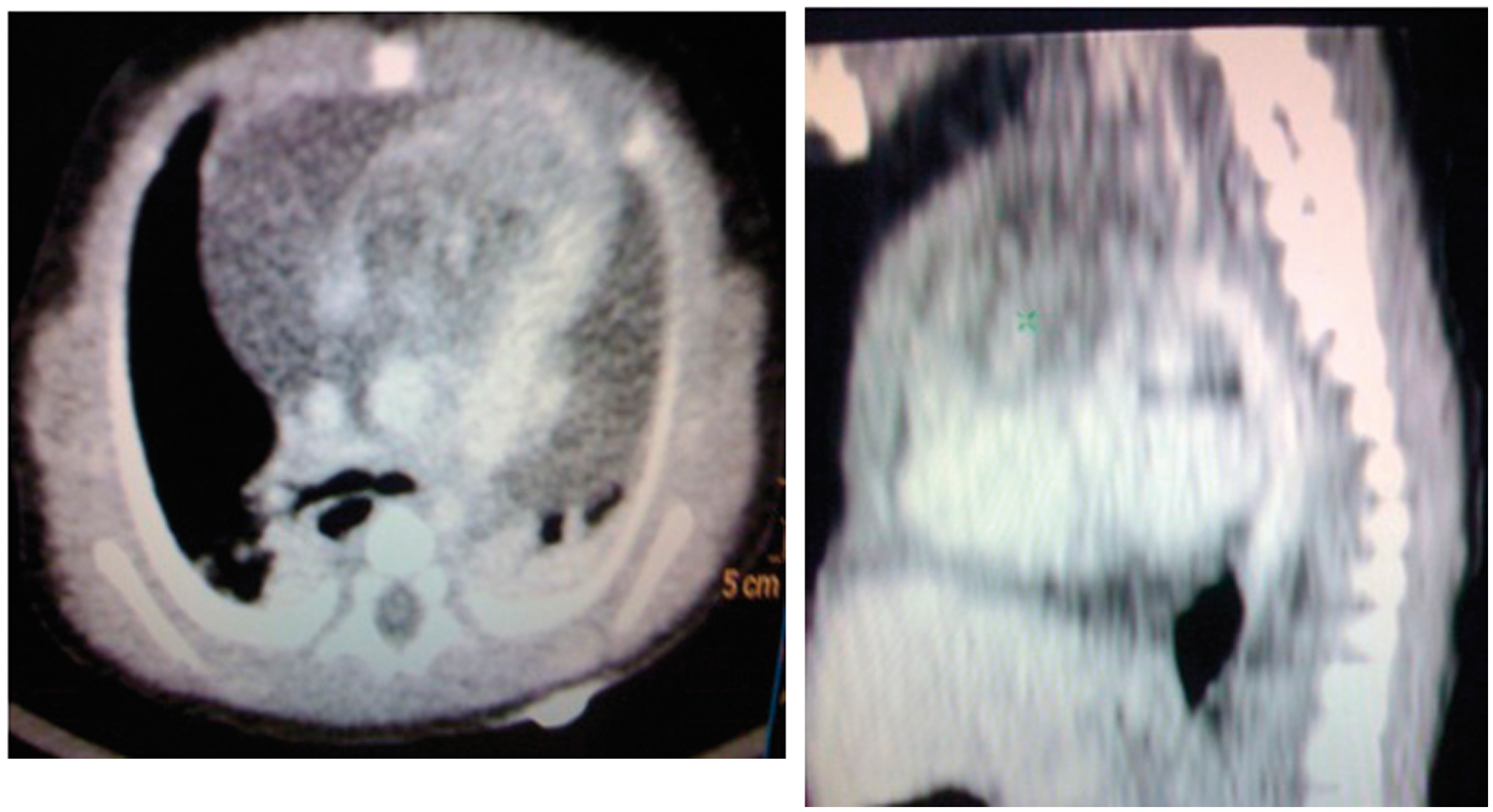
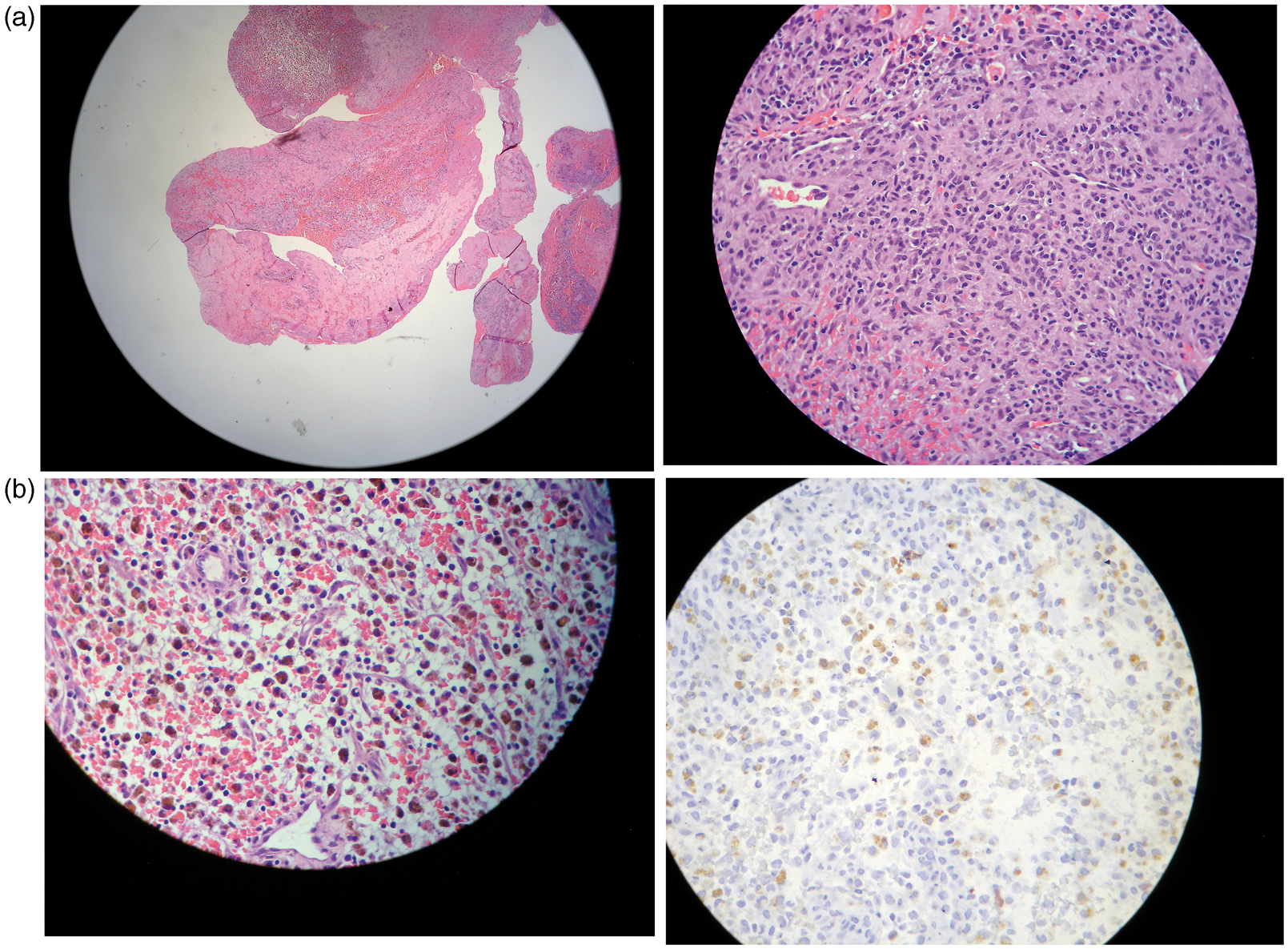
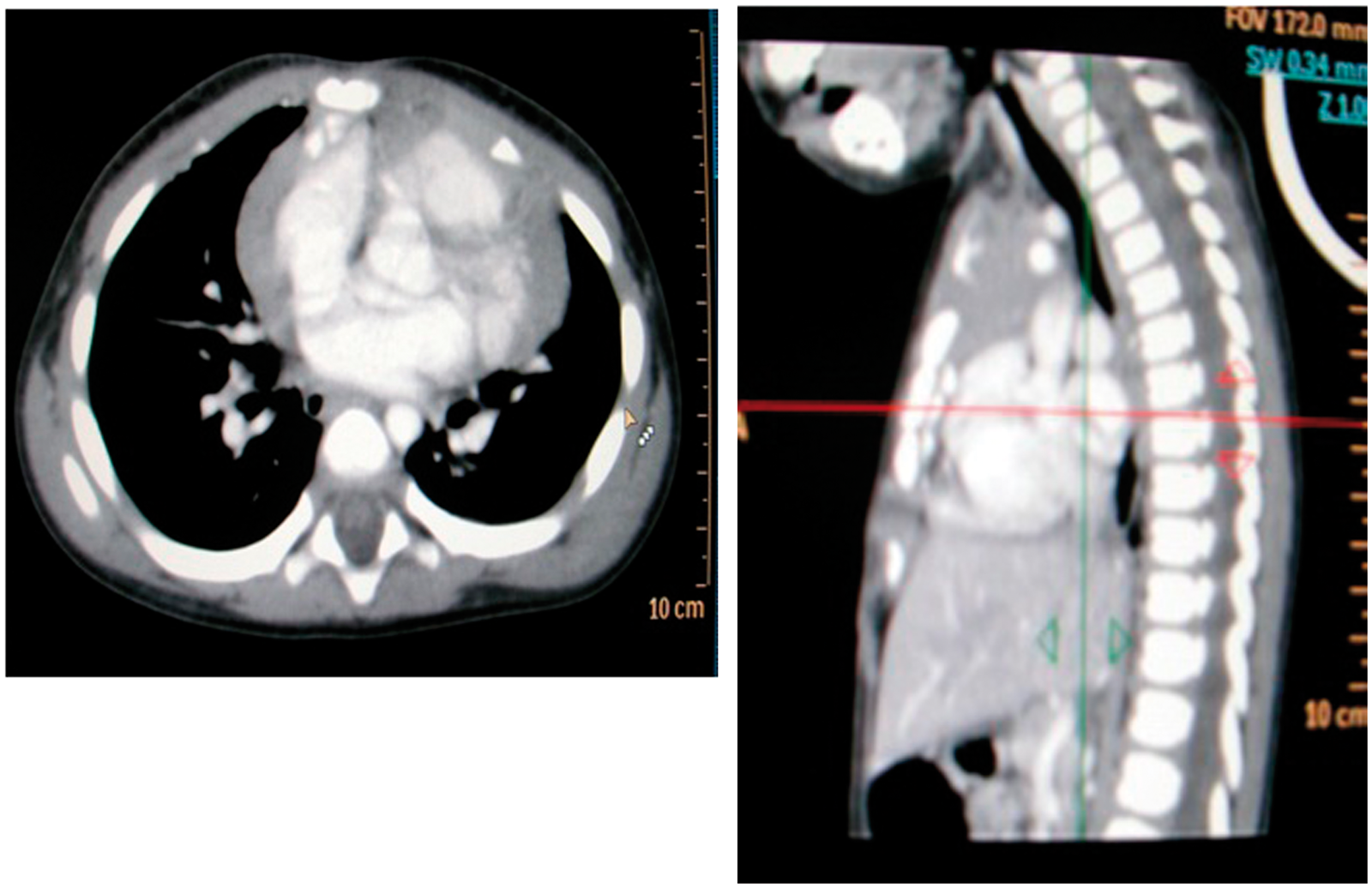
A 12-day-old girl was noted to be dyspneic. She was admitted in respiratory distress, and intubated. Electrocardiography showed supraventricular tachycardia. Two-dimensional echocardiography showed a 1.4–1.6 × 2.8-cm mass in the right ventricular outflow tract with pericardial effusion. Chest radiography showed a convex soft tissue density in the left upper to mid lung, which appeared to be contiguous with the left cardiac border. In the lateral view, a soft tissue density occupied the anterior and middle mediastinum (Figure 1). Computed tomography of the chest confirmed these findings. (Figure 2). Laboratory data showed normal C-reactive protein, blood culture, complete blood count, urinalysis, HIV screening, thyroid stimulating hormones, and cardiac markers. Alpha fetoprotein was markedly elevated at >400 IU·mL−1, but beta human chorionic gonadotropin was normal (<2 IU·mL−1). A biopsy showed a large anteriorly located intramyocardial mass covering the right ventricular outflow tract, great vessels, and a portion of the right atrium. Histopathology revealed an inflammatory pseudotumor, myofibroblastic in nature. Smooth muscle actin was positive in many localized spindle cells, indicative of their myofibroblastic nature. Histiocyte markers CD68 and S100 were both negative. (Figure 3) A search for the possible source of infection was carried out, but cultures yielded no growth. A Mantoux test showed an induration of 18 mm at 48 and 72 h. Chest radiographs of the 3 of 6 household contacts revealed bronchiectasis suggestive of tuberculosis. The patient was started on antituberculosis therapy (isoniazid, rifampicin, and pyrazinamide). After 1 month, the serum alpha fetoprotein level decreased significantly to 135.21 IU·mL−1. A repeat two-dimensional echocardiogram showed a decrease in the size of the mass from 1.9 × 2.6 to 1.3 × 2.2 cm, with resolution of the pericardial effusion. In the 5th month of treatment, a repeat echocardiogram showed a 50% decrease in the mass (1.3 × 1 cm). After 1 year of antituberculosis treatment, a chest computed tomography scans, plain and contrast, showed interval resolution of the mediastinal mass in the region of the right ventricle (Figure 4). Two-dimensional echocardiography also showed that the mass was no longer visible.
Chest radiograph showing a convex soft tissue density in the left upper to mid lung, which appears to be contiguous with the left cardiac border. In the lateral view, a soft tissue density occupies the anterior and middle mediastinum. Chest computed tomography of the patient showing a noncalcified mass overlying the right ventricle, with an enhancing tubular structure that appears to traverse the mass from the region of the right ventricle to the aorta. (a) Showing the polymorphous cell infiltrates composed of round cells, spindle cells, lymphocytes, plasma cells, and few neutrophils. Sprinkled out are numerous hemosiderin-laden macrophages (in arrows). (b) Immunostaining with calretinin show few positive round cells (in arrows) indicative of their mesothelial nature. Repeat chest computed tomography scan with contrast, showing interval resolution of the previously noted mediastinal mass in the region of the right ventricle.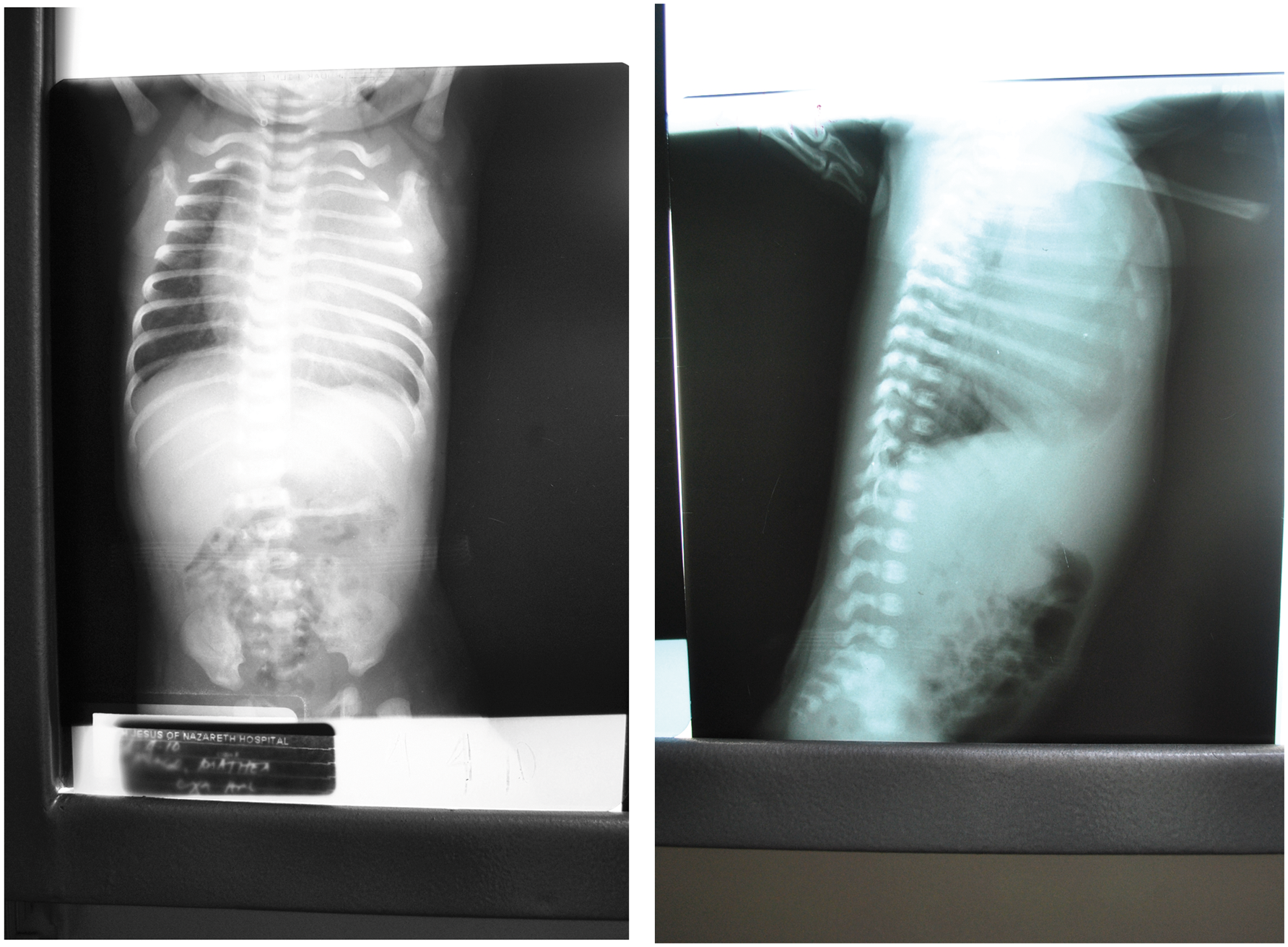
Discussion
This case highlights a rarity of sorts, in that the patient is a neonate. In a study by Agrons and colleagues 5 in 61 patients with inflammatory myofibroblastic tumor, 25 (42%) were aged 18 years or less, and the peak incidence was in the second decade. There has been no case of inflammatory myofibroblastic tumor reported in a neonate so far, and there is no sex predilection. Cough, fever, dyspnea, and hemoptysis are the usual presenting manifestations of inflammatory myofibroblastic tumor. Our patient presented with supraventricular tachycardia.
Mycobacterial pseudotumors are uncommon presentations of Mycobacterium tuberculosis or nontuberculous mycobacterial infection. Worldwide, there have been only 2 cases of mycobacterial inflammatory pseudotumors reported so far, both in adults. Neonatal tuberculosis in this patient was diagnosed based on a positive tuberculin skin test, and overwhelming exposure when contact screening was performed; the presence of the inflammatory pseudotumor was suggestive of granulomatous disease, and indicated a trial treatment of antituberculosis agents. Further work-up such as nucleic acid amplification tests, nucleic acid probes, T-cell-based assays, and tissue culture must be carried out to support the diagnosis. However, because of the high index of suspicion of malignancy, tissue TB culture was not undertaken in this patient.
Inflammatory pseudotumor rarely arises in cardiac tissue. Only 4 cases of cardiac involvement have been reported, all in children aged 4 months to 17 years. Two were asymptomatic and were diagnosed during evaluation for a murmur. The 3rd patient showed signs of vasculitis, polyarthritis, and thrombosis, and had multiple pseudotumor masses seen on echocardiography. The 4th patient had fever, anemia, and prominent abdominal veins. Three of the pseudotumors were located in the right atrium, one was in the right ventricle, and 2 arose from the left ventricle. 6
Tuberculosis involving the heart is rare, accounting for only 0.5% of extrapulmonary TB. The main presenting finding is pericardial involvement, most commonly pericardial effusion. Arrhythmia is also a common manifestation in patients with cardiac tuberculosis. Ventricular tachyarrhythmia was found in a patient with right ventricular involvement of tuberculosis, similar to our patient. 2 In many of the studies reviewed, fine-needle aspiration biopsy, sonography, computed tomography, and magnetic resonance imaging can be used in the preoperative work-up, but in most cases, a definite diagnosis is made based on the histopathological findings from either a resected tumor or needle biopsy. As to prognosis, Coffin and colleagues 7 reported a 25% recurrence rate, and Meis and Enzinger 8 noted 37% recurrence, with at least 1 local recurrence, at a median of 5 months after excision. In general, the primary therapeutic approach is surgery for complete resection if the anatomic location is amenable. Inadequate resection has been shown to be a risk factor for recurrence. Other treatment modalities, such as steroids, have yielded inconsistent results. Radiation therapy may be warranted when resection is not possible, but chemotherapy has not been shown to be useful for treating inflammatory pseudotumors. 8
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.