
Abstract
Background:
While surgery for elderly patients has become more common with the aging of populations, the relatively high frequency of postoperative complications prevents broad application. We retrospectively evaluated prognoses after surgery for non-small-cell lung cancer in patients older and younger than 75 years, to investigate whether age contributes to the risk of a poor outcome.
Patients and methods:
From January 1998 to September 2009, 727 patients underwent curative resection for non-small-cell lung cancer in our department; 119 were over 75-years old (group 1) and 608 (group 2) were aged less than 75 years.
Results:
The rates of postoperative complications (49% in group 1 and 40% in group 2) were not significantly different. Age conferred no significant risk, with an odds ratio of 1.129, whereas smoking, blood loss during surgery, and lymph node dissection exhibited significant associations. Those aged over 75 years had a 1.9-fold higher risk of mortality (p < 0.01), but significance did not extend to disease-specific survival (p = 0.117).
Conclusions:
Postoperative complications in elderly non-small-cell lung cancer patients are dependent on factors such as smoking, blood loss during surgery, and lymph node dissection, but not age. Elderly patients should not be considered ineligible for surgical treatment due to their age alone.
Keywords
Introduction
As in many developed countries, lung cancer is now the leading cause of cancer mortality in Japan, with more than 65,000 deaths recorded annually. Approximately 26,000 patients undergo surgery for lung cancer every year. 1 Since the number of elderly patients with non-small-cell lung cancer (NSCLC) has risen with increasing life-expectancy; surgical treatment of such individuals is a challenge for thoracic surgeons. Recent studies have demonstrated the efficacy and safety of surgery for elderly patients with early stage disease.2,3 According to the Japanese Joint Committee of Lung Cancer Registry, 602 (4.5%) octogenarians underwent pulmonary resection in 1999. 3 However, aging results in physiological changes in the cardiovascular and respiratory systems, and increases the frequency of associated diseases, raising the possibility of increased risk of various complications after surgery. Considerable divergence exists in reported 5-year mortality rates for lung cancer, ranging from 2.8% to 3.7%.3,4 Resection factors predictive of major morbidity are age (10-year increase), body mass index (10 kg·m−2 increase), steroid exposure, chronic heart and/or coronary artery disease, recent smoking, and surgical method, according to the Society of Thoracic Surgeon General Thoracic Database. 5 More information regarding short- and long-term postoperative outcomes is necessary to help surgeons select subgroups of elderly patients suitable for pulmonary resection. In this study, we retrospectively analyzed the surgical results of patients younger and older than 75 years who underwent curative resection for NSCLC in a single institution, and evaluated whether old age contributes to the risk of postoperative complications.
Patients and methods
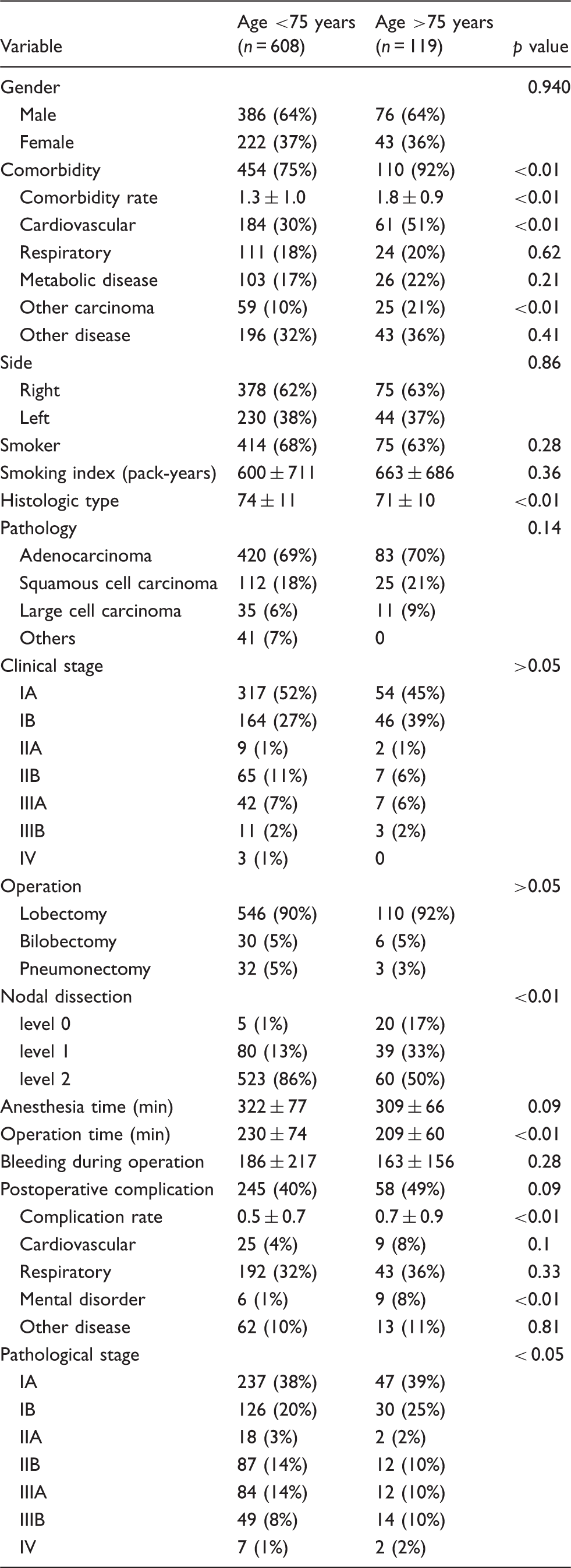
Characteristics of 727 patients undergoing curative resection for non-small-cell lung cancer.
Curative pulmonary resection included lobectomy, bilobectomy, and pneumonectomy by open thoracotomy, but we excluded segmentectomy, wedge resection, and completely video-assisted thoracoscopic surgery. According to the criteria for surgical resection at our institute, the eligibility for surgery was determined based on clinical stage, respiratory function, electrocardiogram, Zubrod or Eastern Cooperative Oncology Group performance status (PS), echocardiography, cardiac scintigraphy, double Master electrocardiography, coronary angiography, and pulmonary ventilation-blood flow scintigraphy when necessary. To determine the clinical stage, all patients underwent blood analysis, chest radiography, chest computed tomography (CT), brain CT or magnetic resonance imaging, and bone scans or positron-emission tomography. 6 Regarding respiratory function tests, those who were predicted to have a postoperative forced expiratory volume in 1 s < 700 mL·m−2 were not indicated for surgical resection. A preoperative PS of 0–2 was regarded as a criterion for surgery. All patients with preoperative comorbidities were treated appropriately. For current and ex-smokers with poor respiratory function, respiratory rehabilitation or tiotropium inhalation was performed for improvement before surgery.
Histological typing was carried out according to the World Health Organization histological classification. 7 Clinical and pathological stages were defined according to the TNM 6th edition criteria of the International System for Staging Lung Cancer. 6 Viability status was determined based on all-cause related death, and survival time was defined as the interval from the date of surgery to the date of death or the end of follow-up. A follow-up examination was usually carried out every 2 or 3 months for the first 2 years and every 4 to 6 months thereafter. The follow-up included physical examinations, tumor marker assessment, and chest radiography. Chest and brain CT scans, bone scintigraphy, and positron-emission tomography were conducted once or twice a year after the operations.
Comorbidities and postoperative complications were diagnosed and recorded daily with laboratory, radiologic, and physiological examinations. Comorbidities included cardiovascular diseases (ischemic heart disease, arrhythmia, chronic heart failure), respiratory diseases such as chronic obstructive pulmonary disease (forced expiratory volume in 1 s < 70% of predicted), interstitial pneumonitis (apparent interstitial shadow detected by chest CT scan), metabolic disorders such as diabetes mellitus (hemoglobin A1C ≥ 6.0%), hyperlipidemia, gout, carcinoma development, and others. Postoperative complications included any of the following diagnoses made after surgical resection: wound infection (accompanying wound failure), postoperative hemorrhage (≥200 mL·h−1), prolonged air leakage (≥1 week), chylothorax (≥1000 mL·day−1), pulmonary embolism, empyema, pneumonia (presenting as an abnormal shadow on chest radiography), respiratory failure (needing mechanical ventilation ≥3 days), myocardial infarction, and cerebral infarction.
Clinicopathological parameters were assessed by Pearson’s chi-squared test or Fisher’s exact test, as appropriate. To determine whether age over 75 years was an independent risk factor for complications, multivariate logistic regression analysis was performed by adjusting for other clinicopathological variables such as sex, smoking, preoperative complications, histological type, PS, operation method, anesthesia time, blood loss during surgery, lymph node dissection, and pathological stage. Long-term prognoses after surgical resection were evaluated with cumulative survival probability using the Kaplan-Meier estimate, and differences in survivor function between the age groups were assessed using the logrank test. Five-year cumulative survival probability was estimated using the life table method with the interval set at 1 month. Among the study population, 305 patients had postoperative complications, with a maximum of 30 variables to be included in the multivariate regression model. Analyses were performed independently at the Kitasato Clinical Research Center using SPSS version 19.0 software (SPSS, Inc., Chicago, IL, USA). A 2-sided p value of <0.05 was considered to be statistically significant, unless otherwise specified.
Results
Comorbidities occurred more frequently in group 1 (p < 0.001; Table 1). There were no significant differences in smoking, preoperative PS, clinical stage, histology, side, and surgical methods. Surgical procedures were not significantly different between the 2 groups. There was a significant difference in the degree of nodal dissection in the 2 groups (p < 0.01; Table 1). There were no differences in terms of anesthesia time, blood loss or pathological stage. Postoperative complications were observed in 49% of group 1 and 40% of group 2; the difference was not significant. The numbers of patients suffering from cardiovascular, respiratory, psychiatric, and other complications were 34, 237, 15, and 75, respectively. Among these, mental disorders (mostly delirium) were more frequent in group 1 (p < 0.01). The mean number of postoperative complications in group 1 was greater than in group 2 (0.72 vs. 0.52 per patient; p < 0.01). Thirty-day mortality and surgery-related death in group 1 vs. group 2 were: 0% vs. 0.1% and 0% vs. 0.6%.
Univariate and multivariate analyses of postoperative complications.
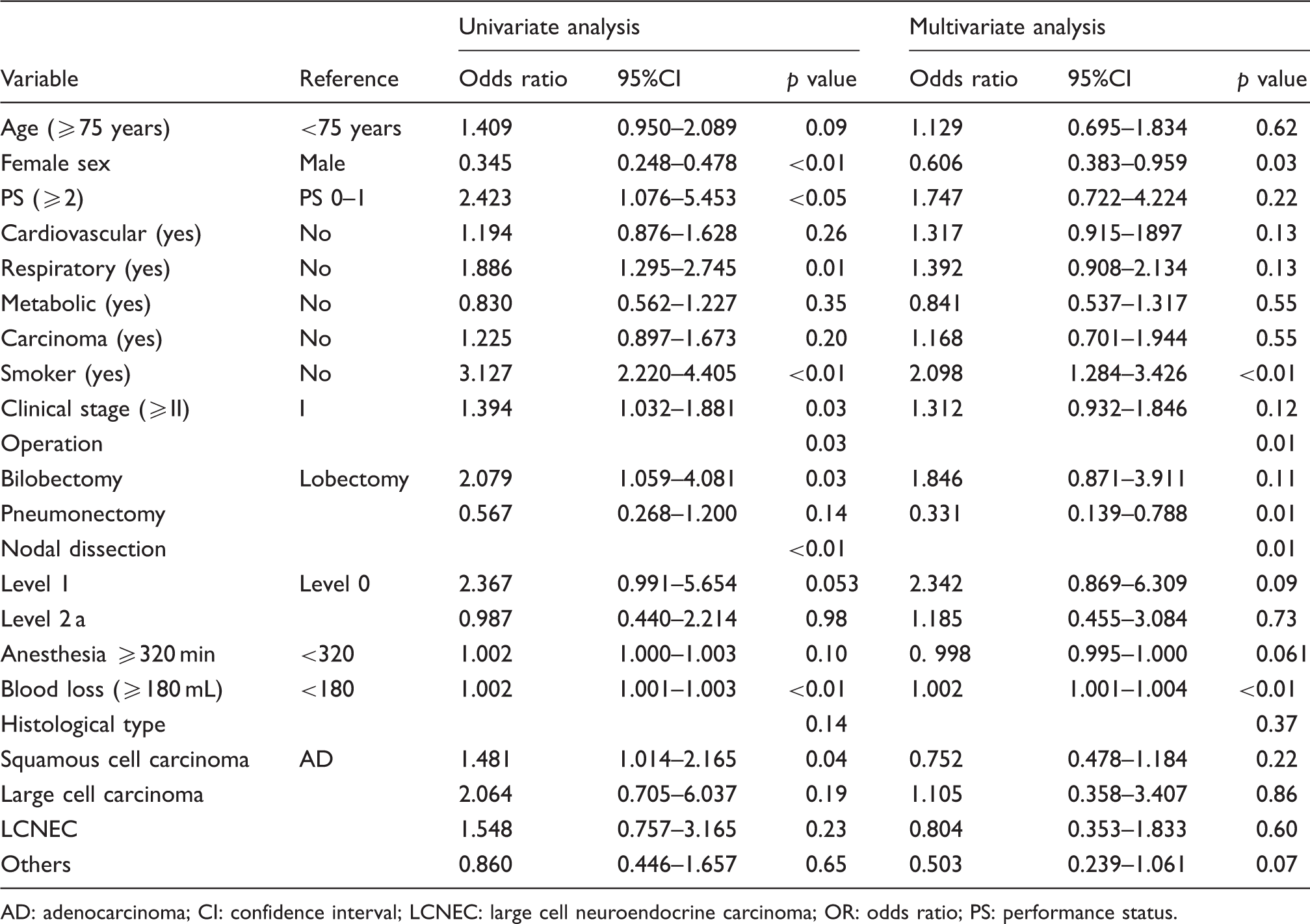
AD: adenocarcinoma; CI: confidence interval; LCNEC: large cell neuroendocrine carcinoma; OR: odds ratio; PS: performance status.
The mean follow-up duration was 38 months. The follow-up time at which 25% of patients had died, in terms of overall mortality, was 23.0 months (95%CI: 16.7–28.3 months) for group 1, but this was not reached in group 2. The 5-year overall survival was 53% for group 1 and 71% for group 2; the difference was significant (p = 0.001, logrank test; Figure 1(a)). With reference to disease-specific survival, the follow-up time was 37.0 months (95%CI: 21.8.7–52.2 months) for group 1 when 25% patients had died from NSCLC with surgical resection, while more than 75% of group 2 were alive by the end of follow-up; however, there was no significant difference between the 2 groups (p = 0.146; Figure 1(b)). For patients with clinical stage I disease, there was a significant difference between the 2 groups in overall 5-year survival (58% and 77%, respectively; p < 0.01), but not for disease-specific 5-year survival (73% and 79%, respectively; p = 0.14).
Five-year survival curves for all cases. (a) Note the significant difference in overall 5-year survival between the groups but (b) the lack of any significant difference in disease-specific 5-year survival.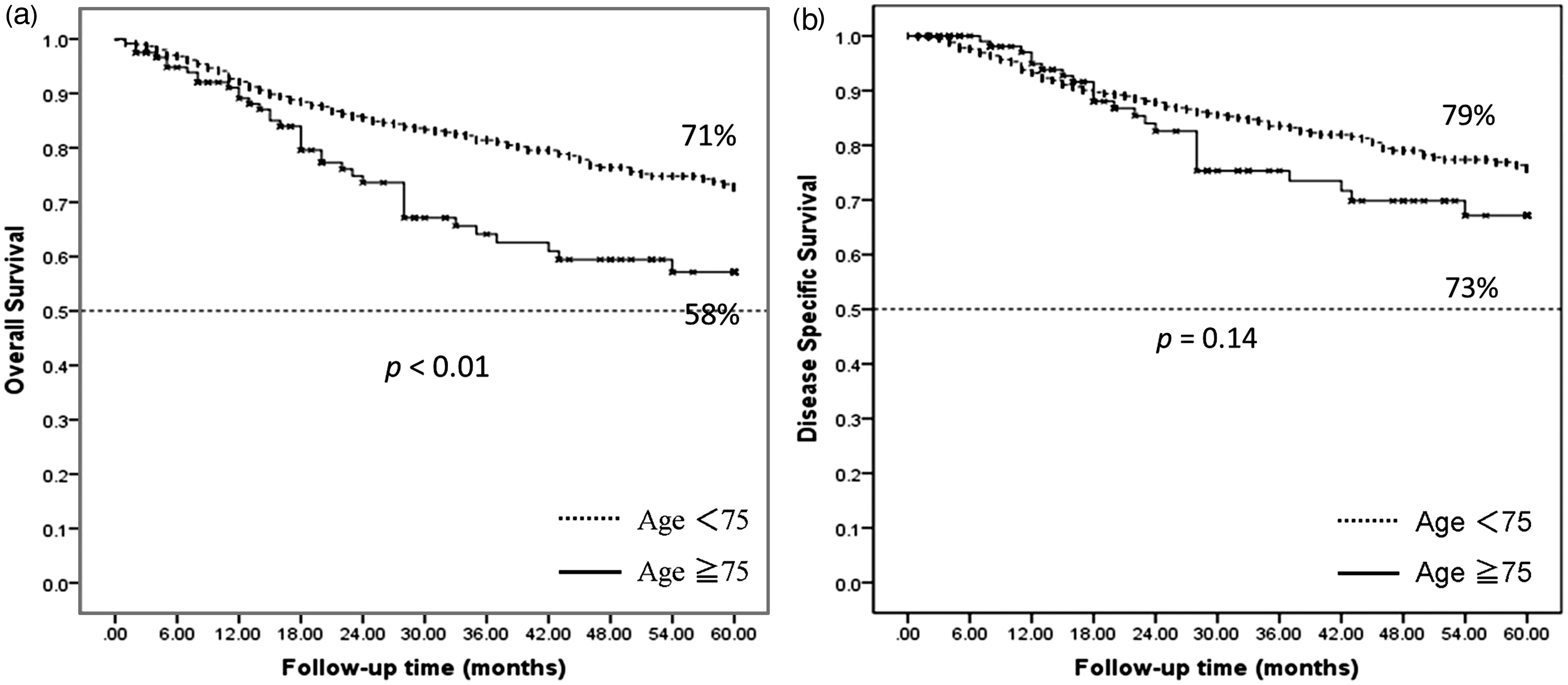
Discussion
In this study, the elderly group was found to have more frequent underlying morbidities than their younger counterparts. Postoperative complications also tended to occur more frequently (49% vs. 40 %) and their mean number was significantly greater (0.72 vs. 0.52, p < 0.01). However, multivariate logistic analysis indicated that age did not independently confer risk. Furthermore, in terms of long-term outcome, while the 5-year survival of elderly and younger patients was 53.3% and 70.5% (p < 0.01), respectively, 5-year disease-specific survival did not differ significantly (p = 0.13). Apart from age, smoking, operative method, lymph node dissection, and blood loss were significantly related to postoperative complications, indicating potential causal relationships. The adverse effect of smoking in NSCLC patients is well-known, and it is suspected that the younger the age at which patients take up the habit, the more serious the postoperative complications will be. Smoking significantly increases the risk of postoperative respiratory, cardiovascular, and other complications, and also impairs wound healing. 8 Data from several observational studies indicate that 4–8 weeks of smoking abstinence before surgery are required to reduce the risk of postoperative complications. 9
A previous study from the Japan Lung Cancer Registry indicated that lobectomy or pneumonectomy was a predictor of a good outcome for patients with stage I disease in the general population. 10 Consequently, minimizing the surgical intervention should be considered for elderly patients with early-stage NSCLC. Regarding lymph node dissection, previous studies in elderly patients have indicated that mediastinal lymph node dissection was a risk factor for postoperative complications, in line with our findings, and there was no long-term survival benefit from radical lymphadenectomy combined with pulmonary resection for elderly patients, because of recurrent nerve exposure, devascularization of the bronchial wall, and increased surgical exudates or bleeding. 11 Recently, advanced technologies such as positron-emission tomography and endobronchial ultrasound-guided transbronchial needle aspiration have become available to evaluate hilar and mediastinal lymph nodes. These modalities could help in selecting patients who can be cured without mediastinal lymph node dissection. In this context, it should be stressed that more accurate evaluation of clinical stage may help to avoid postoperative complications. Although the recommended surgical treatment for early-stage NSCLC is lobectomy accompanied by mediastinal lymph node dissection, lobectomy and a lesser extent of lymph node dissection (level 0–1) are more commonly performed in clinical practice for the elderly than for the general population. Scott and colleagues 12 suggested that there might be an increased risk of local recurrence after surgery, but it is an option to reduce perioperative mortality and morbidity.
The prognostic value of anemia in surgery, both cardiac and non-cardiac, has been emphasized. 13 Although we did not encounter any deaths due to blood loss during operations in our series, we did make efforts to reduce bleeding during surgery. Besides these factors, although not evaluated in this study, to achieve overall long-term benefits of pulmonary resection, it may be valuable for surgeons to consider PS, comorbidities, and clinical stage when selecting patients preoperatively.14,15
Generally, elderly patients at high surgical risk are not indicated for lung resection, and it should be stressed that nonsurgical local therapies are currently used in the treatment of stage I disease.16–18 Because considerable numbers of elderly patients with NSCLC are in poor physical condition, they tend to undergo radiotherapy. Even with recent technological advances greatly improving the long-term results of this modality with low treatment-related mortality, the 5-year survival benefits of radiation were reported to be 23%–42% for elderly patients with stage I NSCLC, and 7%–17% for stages I–IIB NSCLC.19,20 When we compared our surgical data for clinical stage I disease, the outcome was obviously much better (67%), strongly indicating the benefit of surgery. The fact that video-assisted thoracic surgery and limited resection are becoming more and more popular and considered useful for elderly patients with high-risk NSCLC, underlines the necessity for careful assessment of the option of pulmonary resection.
Several limitations of this study need to be considered. Firstly, because of its retrospective nature, we lost approximately 7% of patients who suffered from recurrent cancer and other diseases, which may have resulted in a better estimate of long-term outcome. Further prospective studies with more accurate data are necessary to validate our findings. Secondly, since this was an observational study, we were unable to control for all confounders of postoperative complications. Nevertheless, we feel that the results provide important evidence for surgeons to help in reliable decision-making. We concluded that because aging was not associated with significantly elevated risks of postoperative complications in this study, surgical resection should be weighed as favorable for the management of elderly NSCLC patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.
Acknowledgements
The authors thank Dr Malcolm A Moore for linguistic assistance. The authors also thank Dr Hideki Amano, MD, PhD, Department of Clinical Research Center, Kitasato University School of Medicine, for clinical assistance; and Dr Keika Hoshi, DDS, MDS, PhD, Department of Preventive Medicine, Kitasato University School of Medicine, for helpful advice with the statistical analyses.