
Abstract
Two days before surgery in a 70-year-old man with renal cell carcinoma, transthoracic echocardiography showed a dense mass in the inferior vena cava, lying proximally, but no mass was observed in the right atrium. Intraoperative transesophageal echocardiography revealed unexpected tumor thrombi in the right atrium, and the surgical plan was changed. This case highlights the importance of intraoperative transesophageal echocardiography in patients with renal cell carcinoma.
Keywords
Introduction
Renal cell carcinoma comprises 3% of all adult malignancies, and 4%–10% cause metastases to the inferior vena cava; 1% of patients experience right atrial tumor thrombus. Early diagnosis and surgical treatment are essential for renal cell carcinoma, which has the highest mortality rate amongst urological cancers.1–3 Even though the localization of a thrombus has been determined by preoperative evaluations, there may be migration from the thrombus, and small or large ruptures may occur by the time of operation. 4 The aim of this case report is to highlight the importance of intraoperative transesophageal echocardiography (TEE) in a patient with renal cell carcinoma, which showed unexpected tumor thrombi in the right atrium, and changed the surgical plan.
Case report
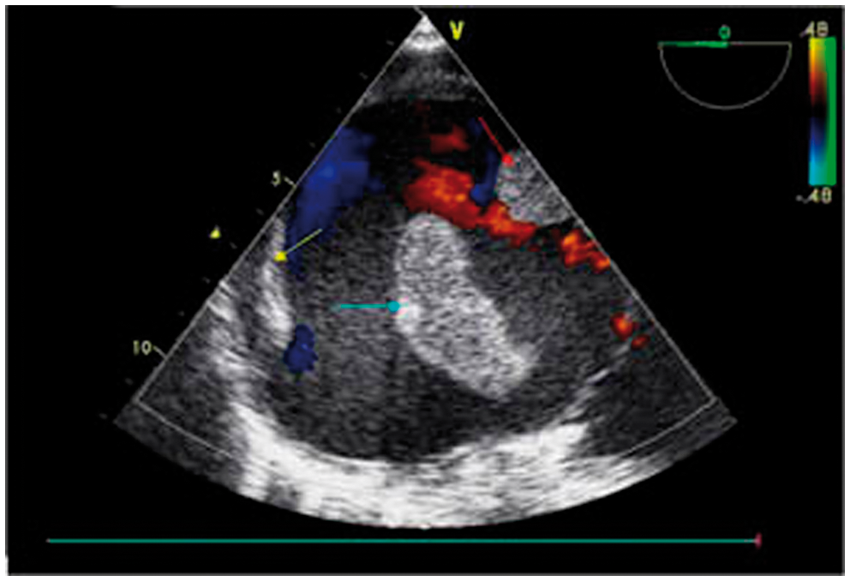
A 70-year-old man was scheduled for a right radical nephrectomy through a laparotomy and thrombectomy from the vena cava by urology and gastroenterology surgeons. Upper abdominal dynamic magnetic resonance imaging revealed a filling defect in the inferior vena cava (IVC) 2 days before the operation. Doppler ultrasonography showed a possible thrombus extending from the right renal vein-IVC junction to the hepatic level. Two days preoperatively, transthoracic echocardiography (TTE) revealed a dense mass in the IVC lying proximally, but no mass was observed in the right atrium. A transabdominal approach was planned, with infrahepatic clamping for resection because the tumor was lying under the junction of the hepatic vein and the IVC. After intubation, a multiplane TEE probe (Vivid 7; General Electric) was carefully inserted through the esophagus. TEE performed before surgical incision unexpectedly revealed possibly 2 tumor thrombi (1 fixed and 1 free-floating) in the right atrium. The freely moving thrombus extended into the right ventricle through the tricuspid valve, passing the leaflets and bouncing back from the ventricular wall. Fortunately, the mass was too large to be located in the ventricle (Figure 1, Video 1 (Available at: http://youtu.be/RPpBeLQdQSg)). The other mass was immobile and located between the coronary sinus and the IVC, on the wall of the atrium (Figure 2). In agreement with the preoperative ultrasonographic findings, a mass lesion was observed within the IVC, just above the hepatic vein, which did not completely occlude the lumen. Based on the TEE findings, we suggested that the operation should be performed under cardiopulmonary bypass to remove the atrial masses, with the help of cardiovascular surgeons. The surgery was completed with no complication during anesthetic maintenance, and the patient was transferred to the intensive care unit. He was extubated after 16 h, and discharged from the intensive care unit 2 days later. Ten days later, he was discharged home in a healthy state.
Mid-esophageal 2 chamber view at 120 degrees of the right atrium and right ventricle, showing the mass (yellow arrow) in the right ventricle. The tricuspid valve leaflets are indicated by green arrows. Mid-esophageal atrial view at 0 degrees (slightly rotated counterclockwise), shows a free mass (blue arrow) in the middle and a fixed mass (red arrow) attached at the dilated atrium above tricuspid valve. Note the pectinate muscle of the right atrial wall indicated by yellow arrow.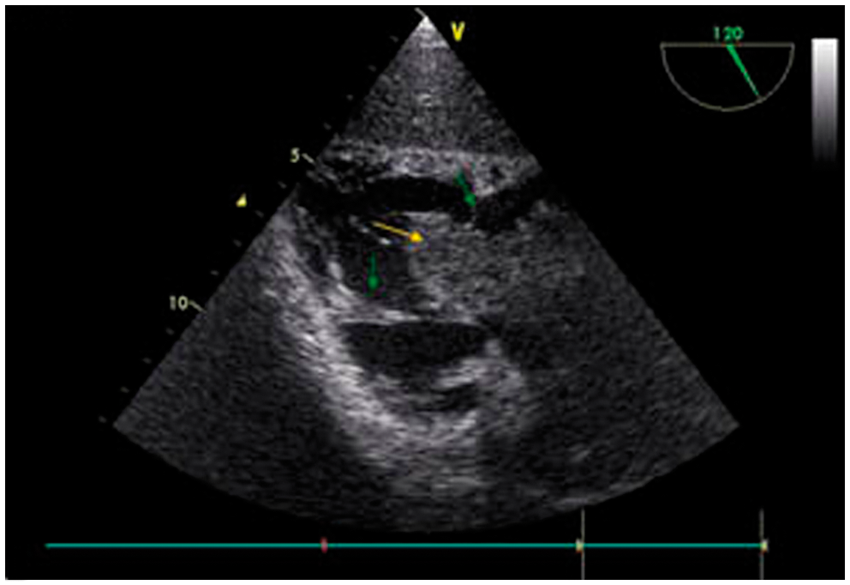
Discussion
Although many detailed preoperative techniques such as magnetic resonance imaging, TTE, computed tomography, and venography are used to detect the size of the tumor, TEE seems to be mandatory to evaluate the heart and inferior vena cava in renal cell carcinoma patients. Because it may change the surgical plan and save the patient’s life, we emphasize that TEE is an essential tool in such cases.
In patients with thrombus, a dreadful complication for the anesthesiologist is pulmonary emboli caused by particles breaking off from the thrombus. Because renal cell carcinoma has vigorous prothrombotic properties, breakage, enlargement, or migration of a tumor thrombus may occur even a few days after determination of the location. 5 Therefore, it is very important to confirm the preoperative status by intraoperative TEE when available. Preoperative magnetic resonance imaging and computed tomography are extremely useful and highly sensitive for detection of intracardiac masses or tumor thrombi in patients with renal cell carcinoma, but were not carried out in this case. Nonetheless, separated fragments of thrombus always pose the risk of pulmonary embolism.
In our case, the fragment was confined to the right atrium. During voiding, it moved into the right ventricle, but its movement was limited by the papillary muscles attached to the tricuspid valve, and it bounced back from the right ventricular wall, and thus was confined to the right atrium. It caused second-degree tricuspid insufficiency, but did not cause a collapse because it did not remain in the ventricle during systole. In this case, the thrombus was not small enough to pass into the pulmonary artery, and this saved the patient’s life. Preoperative TTE failed to detect the fixed mass, but it was almost impossible not to notice the mobile giant thrombus in the right atrium. Therefore, we argue that the mobile thrombus split from the main tumor after the TTE 2 days before the operation. TEE easily detects small fixed mass between the IVC and coronary sinus, which cannot be detected with TTE. Unlike TTE, TEE provides better overall visualization of masses, especially those located in the posterior cardiac structures. 6 Another reason might be that tumor invasion into the IVC enlarged in 2 days. Because these tumors are hypercoagulable in structure, a formed thrombus may expand rapidly, and even microembolism may occur. 4
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.